5
The psychogenics of wind turbine complaints
In this chapter, we turn to the data for clues as to why some residents report symptoms of ‘wind turbine syndrome’ while others do not. We examine temporal and geographical patterns of symptom reporting, the social context in which symptoms are reported, and the individual and personality differences that set apart those who do and do not report symptoms. We also describe experimental research that has tested the possible role of psychological expectations in triggering health complaints.
We consider how environmental health risks tend to be assessed and what factors can predict community outrage about perceived risks. We explore how windfarm health issues have been portrayed in the media, and how that narrative has shaped perceptions of health risks in some communities.
We then explore whether heightened risk perceptions can help to explain the emergence of health complaints in windfarm communities. Evidence shows that concerns about an environmental agent can lead people to report symptoms during exposure to that agent, even when the exposure is completely benign. When people are worried about exposure and expect to experience adverse health effects, they are more likely to notice and misinterpret common symptoms, including symptoms that may be caused by anxiety. This power of negative expectations to trigger symptom reporting in response to innocuous environmental agents, also known as the nocebo effect, has been seen throughout history.
In the case of windfarms, health complaints have tended to cluster in geographical areas where there has been targeted negative publicity about wind turbines, or where people are accessing negative health information about windfarms. This indicates that these clustered outbreaks are ‘contagious’, spreading via communication.
Finally, we summarise experimental research that tests whether socially transmitted negative expectations may be providing a pathway for symptom reporting in windfarm communities. The practical implications of these findings are considered in light of a case study demonstrating that, in a rural community in which a windfarm was being planned, the actions of anti-windfarm advocates generated negative media stories about the alleged health risks of windfarms, which in turn provoked fear in residents.
Outrage factors
As we discussed in Chapter 2, windfarms operated for many years before complaints about health effects emerged, with aesthetic objections being the dominant reason given for opposing windfarms in their early years. The environmental health scientists Loren Knopper and Christopher Ollson had attended numerous public consultation meetings about proposed windfarm developments in Canada when they noticed in 2011 that fears about health risks had started to become the primary focus of opposition at many of these meetings.1 As we saw earlier, these fears are often expressed in frightened, outraged language. To understand how unwarranted and disproportionate health concerns can take hold in a community, it is useful to consider how people assess risk. In general, public perception about the relative harm posed by exposure to environmental agents has little to do with actual toxicological evidence.2 Research in the area of risk perception and communication indicates that people are more likely to assess environmental health risks by the strength of community ‘outrage’ associated with the purported threat rather than in terms of objective risk of harm.3 Outrage can be predicted by the presence or absence of various factors, which in Table 5.1 we have applied to the case of windfarms.4 Peter Sandman5 has produced matrices of factors that have been often found to be associated with increased levels of community ‘outrage’ about putative environmental threats to health. Sandman distinguishes ‘primary’ from ‘additional’ factors, with primary factors being those that have been shown to be more strongly associated with increased levels of community concern.6
| Outrage higher if: | Outrage lower if: |
|---|---|
| Primary factors | |
| exposure is coerced (e.g. among those not electing to house turbines on their land)** | exposure is voluntary (e.g. among those electing to house turbines on their land)** |
| agent is industrial** | agent is natural |
| agent is exotic** | agent is familiar (e.g. higher outrage for newly built windfarms, less for long-running more familiar farms) |
| agent is memorable** | agent is forgettable |
| consequences are dreaded (e.g. cancer, birth defects) | consequences are not dreaded* |
| consequences are catastrophic (e.g. many people suddenly and badly affected) | consequences are chronic* |
| true hazard is unknowable (because of many confounders)* | true hazard is knowable (e.g. broad scientific consensus about effects) |
| hazard is controlled by others** | hazard is individually controlled |
| exposure is unfair (e.g. not all citizens exposed equally)** | exposure is fair |
| sources are seen as untrustworthy (e.g. wind companies)* | sources are seen as trustworthy |
| process is unresponsive (e.g. demands for action not quickly met)** | process is responsive |
| Additional factors | |
| affects vulnerable populations* | affects general population |
| health effects are delayed* | effects are immediate* |
| poses substantial risk to future populations | poses no threat to future populations* |
| victims are identifiable (e.g. named complainants)** | victims are statistical |
| not preventable | preventable* |
| few benefits | many benefits** |
| substantial media attention** | little media attention |
| opportunity for collective action** | no opportunity for collective action |
Table 5.1 Primary and additional components predicting community outrage about putative environmental risks to health: the case of wind turbines. (** = applies strongly to wind turbines; * = likely to apply less strongly)
Perceptions of the risks posed by environmental agents, particularly those not yet directly experienced by people, tend to be informed by information provided through the media. Given the public does not generally have direct access to scientific reports, which are often hidden behind paywalls in research journals, the media have, in effect, become the public’s proxy science interpreter, translating the current state of scientific knowledge for a lay audience.7 However, content analyses of media reporting about environmental health risks, such as those posed by new technologies, have consistently shown that the media often misrepresent the current state of scientific evidence and overstate the potential for harm.8
Relevantly, acoustician Geoff Leventhall has considered historical media reporting about infrasound.9 Although continuous exposure to sub-audible environmental infrasound is a normal part of everyday life, there continue to be pervasive misapprehensions about the nature of infrasound.10 Misperceptions are likely to have evolved from mid-20th century misrepresentations about infrasound in popular science journals and books.11 In the 1960s and 1970s, various sensational claims were made about infrasound, ranging from the completely absurd (e.g. that infrasound ‘vibrations’ mashed a technician’s internal organs into an amorphous jelly, leading to his spontaneous death) to the patently misinformed (e.g. that testing of infrasonic generators had broken all the windows within a half mile of the test site).12 The mischaracterisation of infrasound as a silent killer led to media speculation that infrasound exposure was responsible for a variety of maladies and calamities from brain tumours and sudden infant deaths to road accidents.13 A selection of UK press headlines from the period captures the mood:14
The silent sound menaces drivers (Daily Mirror, 19 October 1969)
Does infrasound make drivers drunk? (New Scientist, 16 March 1972)
Brain tumours ‘caused by noise’ (Times, 29 September 1973)
Crowd control by light and sound (Guardian, 3 October 1973)
Danger in unheard car sounds (Observer, 21 April 1974)
‘The silent killer all around us’ (Evening News, 25 May 1974)
‘Noise is the invisible danger (Care on the road, Royal Society for the Prevention of Accidents, August 1974)
Over the past decade, allegations that windfarm sound, particularly infrasound, causes health effects have proliferated through the media. Such claims have persisted despite consistent evidence, outlined earlier in this book, that there is nothing unusual about the levels of infrasound produced by windfarms and that infrasound generated by wind turbines does not significantly contribute to background levels of infrasound in the environment.15
Historically, unfounded media health scares were propagated through traditional broadcast and print media and so have generally had a limited lifespan, with public concern dying away when the media have finished covering the story (as the adage goes, ‘Today’s news is tomorrow’s fish-and-chip paper’). However, the advent of the internet has meant that media health warnings about windfarm sound have been perpetuated well past their date of initial publication or broadcast. The internet has also become a major conduit for the dissemination of misinformation about windfarm health effects by anti-windfarm activists. In particular, there has been a significant use of social media to propagate anti-windfarm messages.16 Those seeking information about windfarms by employing simple internet searches can very easily land on sites dedicated to disseminating anti-windfarm messages. Evidence also suggests that, after repeated exposure to the deceptive claim that exposure to windfarm sound poses health risks, there will be a default tendency to believe the information is correct, a phenomenon known as the illusory truth effect.17 In the face of such illusory truth, particularly if it is based on information from multiple sources, people may even abandon their prior belief or knowledge that such fears are unwarranted.18
The following exemplify news articles currently available on the internet:
Wind turbines cause heart problems, headaches and nausea, claims doctor … Wind turbines can cause heart problems, tinnitus, nausea, panic attacks and headaches among people living nearby, according to a US doctor who has studied their effects for five years. (Telegraph, 3 August 2009)19
Wind turbines are either making people sick or driving them crazy … For sufferers of ‘wind-turbine syndrome’, renewable energy is the stuff of nightmares. (Salon, 16 September 2013)20
Wind turbine infrasound’ may be making thousands sick in UK, US … If it is directed at you, you can feel your brain or your body vibrating. (Daily Caller, 11 August 2014)21
An ill wind blows as the surge of turbines stirs fears of silent danger to our health … Tens of thousands of Scots may be suffering from a hidden sickness epidemic caused by wind farms, campaigners have warned. (Express, 10 August 2014)22
Risk perceptions are also heightened when there is an impression that the scientific community does not fully understand the nature of a risk.23 As scientific understanding is rarely, if ever, complete this factor provides fertile ground for public anxiety. A media tendency to give equal weight to both sides of a story, even when the science overwhelmingly favours only one side, can result in what has come to be called ‘balance as bias’.24 Despite overwhelming empirical evidence confirming that wind turbine infrasound is not causing health effects, news stories often ‘balance’ the current state of the science with the counter-narrative by citing Pierpont, Laurie, or others. In some cases, the science is egregiously misrepresented. This is seen in an article published in the (UK) Telegraph in 2015 with the headline ‘Wind turbines may trigger danger response in brain’ and the strapline ‘The low frequency noises from turbine blades can be picked up and can trigger a part of the brain linked to emotions, scientists have found’, which misreported the science and the study it purported to summarise.25 The headline and strapline remain misleadingly intact online, despite the correction found at the foot of the article, which reads:
CORRECTION:
The University of Munich research mentioned in this article did not examine ‘noise levels similar to living near wind farms’, as reported in an earlier version, nor did it find that these ‘could lead to severe hearing damage or even deafness’.
Further, some anti-windfarm websites publish stories intended to create fear and undermine public trust. For instance, a story headlined ‘Is big wind the new big tobacco?’ on one such website conveys a disturbing picture of an attempted cover-up. It is a story designed to create suspicion that the public is being lied to.26 Such a story is bound to create unease, if not anger and fear, in some readers. Content analyses of media stories published in geographical areas where health fears are prominent have revealed a media tendency to publish negative stories likely to amplify health concerns. For instance, in Canada, where concern about the health effects of windfarms has led to a huge publicly funded epidemiological study, evidence indicates that media reports about windfarms contain factors likely to induce anxiety and concern about health risks posed by turbine sound.27 Further, the trend for newspapers to portray windfarms negatively has been shown to be even more evident in community newspapers covering local windfarm issues.28 This finding may explain regional differences in health-risk perception seen in Ontario, where opposition to windfarms has been stronger in smaller regional communities than in the population at large. In Australia, mainstream media reporting about windfarms has also been criticised for misreporting the scientific evidence about alleged health effects; in a recent case of misreporting, one national newspaper made the flagrantly erroneous statement that a ‘ground-breaking’ study had concluded that people living near windfarms faced a greater risk of suffering health issues caused by exposure to turbine-generated low frequency noise.29 Overall, there is currently a propensity, in the countries where concern about windfarms is highest, for some mainstream media to misreport the physiological effects of infrasound exposure, and to suggest that infrasound causes adverse health effects in residents living in proximity to wind turbines. Studies indicate that, as the issue receives more prominent treatment by the media, anticipatory fear of health effects become more evident in communities faced with the prospect of windfarm development.30 This is highlighted by reports from residents of West Lincoln in Ontario of stress-related health effects related to the idea of the construction of a proposed windfarm. Consider the statements made by some residents when interviewed by a community newspaper, Niagara This Week:
‘We are already affected by the turbines. Our stress is already high.’
‘I’ve been to the doctor. They told me to move. My stress level has skyrocketed. My physician told me my stress will kill me before the wind turbines.’31
Wind turbines can apparently make some people sick before they are even built.
Health concerns inform negative expectations
Groups opposed to wind turbines have galvanised opposition to proposed windfarms by calling public meetings and disseminating negative information designed to stimulate health concerns. Such fear mongering is designed to heighten anxiety and create specific concerns about potential symptoms. This was epitomised in a full-page advertisement in placed by the anti-windfarm group the Western Plains Landscape Guardians in the Pyrenees Advocate in Waubra in 2009, warning residents that they could expect to experience sleep disturbance, vertigo, irritability, nausea and a range of other symptoms if they lived within five kilometres of a turbine.
The question that logically follows is whether heightened concern can explain the appearance of health complaints in communities near windfarms.
Field research indicates that the more worried individuals are about the health effects of an environmental exposure, the more likely they are to report symptoms, even when no health risk is posed. As discussed in Chapter 4, a field study conducted in Germany revealed that residents’ concern about the health effects of proximity to mobile phone base stations adversely affected their sleep quality, while exposure to electromagnetic fields itself had no such negative impact.32 In another study, Keith Petrie and his colleagues investigated symptom reporting during a suburban insecticide spraying program.33 Worries about the health risks posed by aspects of modern life, such as environmental pollution, appeared to prime some residents to expect symptoms, so that they started to monitor their bodies for adverse health impacts. As a result, common symptoms and sensations were noticed and misattributed to exposure to the insecticide.
Our bodies are constantly subject to vague, diffuse, and fluctuating physiological sensations that generally go unnoticed.34 When we are worried about our health, particularly if we suspect we have been exposed to a pathogen or toxin, we are more likely to attend to and monitor our bodies to evaluate whether we are becoming ill. Normal bodily sensations that have previously passed undetected are then easily misinterpreted as a new and worrying reaction to a noxious agent. Experiencing physical symptoms is also common. A recent population survey conducted in New Zealand found that, on average, respondents experienced five different symptoms during the previous week. In fact, almost 90 percent of respondents experienced at least one symptom, and 23 percent reported ten or more symptoms.35 It is understandable that individuals would misattribute such symptoms to an innocuous environmental agent if they already have health concerns about exposure to that agent. In addition, increased anxiety about perceived toxic environmental exposure is in itself likely to cause an increase in symptoms such as dry mouth and rapid heartbeat.36 Evidence suggests that people may misinterpret symptoms of anxiety as signs of illness, particularly if the symptoms experienced are consistent with pre-existing health concerns.37 When symptoms stem from negative expectations, rather than from pathogenic exposure, this is a manifestation of the nocebo phenomenon, whereby ‘expectations of sickness and the affective states associated with such expectations cause sickness in the expectant’.38
Placebo and nocebo effects: an illustration from drug trials and pain studies
While people are often aware of the placebo effect (also called the ‘positive expectation’ effect),39 many are less familiar with the concept of the nocebo effect (or the ‘negative expectation’ effect).40 A good understanding of placebo and nocebo effects can be found by considering data from randomised controlled drug trials.
Participants in drug trials are generally randomly assigned to receive either the drug being tested or an inactive placebo, such as a sugar pill, to determine whether the active drug has any efficacy over and above an inert treatment. The participants are not told whether they are receiving the active drug or the placebo. Analyses of the results of drug trials have consistently shown that participants who receive a placebo often experience clinical improvements that can substantially enhance their treatment outcomes.41 A review of randomised placebo-controlled drug trials found that approximately one in five participants who received an inert placebo spontaneously reported experiencing side effects.42 Another study found that these side effects often mirror the side effects of the active treatment, and that between 4 and 26 percent of patients in placebo control groups discontinued use of the placebo because of the perceived side effects.43
Evidence indicates that participants in drug trials often have both positive and negative expectations: they anticipate improvements, and worry about the possible side effects of the drug being tested (because participants must give informed consent, they must be made aware of possible side effects).44 It is because expectations formed from informed consent processes provide an idea of the symptoms to look for that reported side effects in the placebo arms of drug trials often reflect the type of symptoms associated with active treatment. The powerful influence of such expectations has been nicely demonstrated in experimental pain studies using neuroimaging techniques. In one study, the effect of positive and negative expectations on experimentally induced visceral pain was investigated using functional magnetic resonance imaging (fMRI).45 Participants received an inert substance intravenously, accompanied by either positive instructions that they should expect to experience pain relief, or negative instructions that their pain would increase. The participants’ reported experience and their neural processing of visceral pain as measured by fMRI were both consistent with the instructions they had been given, confirming that their reports were not the result of ‘response bias’ (the tendency to give an expected or socially desirable answer) but reflected their authentic experiences.
Nocebo effects may arise as an adverse effect of placebo therapy, but they have also been shown to occur more widely. There are numerous examples of people reporting symptoms that are unrelated to any biological or pathogenic cause but which are triggered by expectations of adverse health effects.46 This has been seen throughout history; as Francis Bacon (1561–1626) famously noted, ‘infections … if you fear them, you call them upon you’.47 The common expression that someone is ‘worried sick’ goes to the heart of this phenomenon. When people mistakenly believe they have been exposed to an ongoing environmental health threat, negative expectations and symptomatic experiences may persist for years, particularly if the concern has been amplified by media attention.48 In one example, residents of a small Memphis town exhibited a dramatic escalation in symptom reporting following a health scare fuelled by media reports that they were living near an old toxic waste dump.49 Residents were not reassured by soil toxicity tests which showed that no hazard existed, and increased symptom reporting continued. It was only when it came to light that authorities had been mistaken as to the location of the dump site, which had in fact been situated many miles from the town, that symptom reporting began to subside. However, even this information was not convincing to some residents, who continued to believe they were experiencing adverse health effects from the phantom dump site.
Nocebo responses have also been implicated in health scares involving other modern technologies. As we saw in the Introduction, the advent of new technologies has consistently been associated with complaints involving a constellation of symptoms akin to those attributed to windfarms.50 In recent years a number of people have expressed health concerns about technologies that emit weak electromagnetic fields, such as mobile phones, and have attributed a range of symptoms to exposure to these technologies.51 However, evidence from a number of double blind provocation studies suggests that negative health effects are caused not by exposure to electromagnetic fields, but rather by worry about such exposure.52 In a double-blind provocation study, participants are exposed both to the stimulus to which they attribute symptoms (such as low-level electromagnetic fields) and to a neutral control stimulus (such as sham or fake electromagnetic fields). During the experiment both participants and the experimenter are unaware whether the exposure is to the real or the sham stimulus. Such studies have consistently shown that sham exposure to electromagnetic fields can activate symptoms in individuals who believe that they suffer from electromagnetic hyper-sensitivity.53
It is important to reiterate that while the exposure itself might be benign, the symptoms reported are not imaginary. As noted above, neuroimaging has confirmed this. In one study, for subjects who self-identified as sensitive to electromagnetic fields, exposure to sham mobile phone radiation was accompanied by activation of brain areas involved in pain perception and the elicitation and control of sympathetic autonomic arousal.54 When we suggest that nocebo responses may be responsible for health effects, we are not dismissing these symptoms as imaginary or ‘all in the mind’. What the evidence demonstrates, however, is that, to responsibly alleviate suffering, treatment options should target sufferers’ expectations, rather than having sufferers simply avoid the technologies they believe are causing their problems.
In the case of windfarms, the type of health complaints attributed to wind turbines, as well as the timing and location of these complaints and who is making them, all suggest that negative expectations may explain the appearance of symptoms in windfarm communities.
The symptoms attributed to windfarms
Many of the symptoms said to arise from exposure to windfarms, such as headaches, tinnitus, fatigue, concentration difficulties, insomnia, gastrointestinal problems, and musculoskeletal pain, are commonly experienced by healthy individuals living in all communities, regardless of whether they are near a windfarm or not. Further, some health complaints attributed to windfarms, such as vestibular symptoms of dizziness and nausea, are symptoms commonly experienced when a person is anxious or distressed.55 As previously discussed, such symptoms are easily misinterpreted as being directly caused by an environmental agent, rather than a result of stress exacerbated by ongoing concern about perceived toxic exposure.
It is true that symptoms such as tinnitus and sleep disturbance can also be indicative of harmful sound exposure. However, the idea that people living in the vicinity of windfarms can expect to experience these symptoms has been widely promoted in the media, and by windfarm opponents increasingly using the portentous-sounding diagnosis of ‘wind turbine syndrome’. As we saw from the evidence from drug trials, such negative expectations are powerful: they will guide people to notice these symptoms and to attribute them to windfarms. An analysis of symptom reporting by people living near wind turbines in Canada found that the reported symptoms were no more prevalent in windfarm communities than in the general population, suggesting that people were misattributing their common symptoms to wind turbines, rather than becoming more symptomatic.56
It is interesting that in households where health complaints are reported, adverse effects often extend to every family member in residence, although the effects may take different forms.57 In one family, exposure to windfarm sound was said to have caused allergies in a child, social withdrawal in a teenager, symptoms of tinnitus in the mother, and a constant discomforting sensation in the chest of the father.58 This suggests a process whereby all health complaints are attributed to the household’s proximity to windfarms, rather than to other, more likely, causes.
Retrospective symptom reporting: subjectivity and recall bias
Windfarm opponents sometimes counter the suggestion that symptoms could arise from negative expectations by arguing that this ‘cannot account for those who were pro-turbine prior to commissioning only to experience adverse health effects post-commissioning’.59 However, there are a number of reasons why a person’s expectations may change. Social context can play a role, such as exposure to intra-community conflict about windfarms. Negative expectations may develop because of exposure to anti-windfarm rhetoric and warnings about the purported health effects of turbine sound. Being told that there is a health risk associated with something you previously supported can be enough to elevate concern and create negative expectations. Once these expectations are formed it is easy to retrospectively misattribute the ordinary experience of symptoms or illness to wind turbines.
Retrospective reports of symptoms are also likely to suffer from recall bias, where there is a tendency to overestimate the incidence and intensity of past symptoms.60 Research consistently shows that when people are remembering past symptoms they are likely to rate the symptoms as being more frequent and more severe than at the time they were actually experienced. Interestingly, this bias may occur immediately after the symptom episode.61 In the case of windfarms we see this in research comparing objective and subjective measures of sleep disturbance, discussed in Chapter 4.62 In this instance, participants were studied before and after the installation of wind turbines in their community. Objective data collected using polysomnography to measure physiologic signals showed that there were no significant changes in the sleep of participants when they were exposed to wind turbine sound. However, subjective data collected using sleep diaries revealed a deterioration in reported sleep quality over time. The issue was apparently one of biased recall. Without the benefit of objective measurement it would have erroneously appeared as though wind turbines had adversely affected residents’ sleep.
It is notable that diseases such as diabetes, duodenal ulcers, skin cancer, herpes and stroke, have been ascribed to exposure to windfarm sound.63 This strongly suggests the involvement of negative expectations, given there is no evidence that windfarms could be responsible for any of these diseases. Over recent decades people have become more inclined to believe that ill health is a by-product of exposure to a toxic environment, and to look for environmental explanations for illness.64 This is illustrated by research indicating a tendency among survivors of the ten most common cancers to believe that environmental factors play a much more significant role in carcinogenesis than is indicated by the scientific evidence.65 Negative expectations arising from health concerns about environmental agents can lead sufferers to misattribute their illness to environmental exposure, rather than to more likely influences such as aging, genetic predisposition or lifestyle.66
The social transmission of symptoms
As we have seen, while windfarms have been operating in many countries for over 25 years, health concerns about them are much more recent. The vast majority of health complaints arose after the self-publication of Pierpont’s Wind turbine syndrome in 2009 (see Chapter 2). There is also evidence of a clustering effect, whereby symptoms tend to arise in geographical locations where there has been targeted negative publicity about wind turbines, or where people are accessing negative health information about windfarms. Thus, there are clear indications that exposure to information about purported health risks might be playing a determinative role.
There is consistent evidence from both experimental and field research that media warnings and information circulated via social discourse may create negative expectations and prompt complaints of symptoms, even when the environmental exposure is completely benign.67 Merely watching a television report promoting a link between exposure to wi-fi and adverse health effects has been shown to increase the likelihood of experiencing symptoms following exposure to a sham wi-fi signal, and to increase the risk of developing an apparent sensitivity to electromagnetic fields.68 In the Netherlands, exposure to media reports about a fireworks explosion was associated with increased reporting of medically unexplained symptoms, not only by victims directly impacted by the disaster but also by people not directly affected.69
The social contagion effect
As already noted, of the small proportion of people worldwide who have reported symptoms ascribed to windfarms, many live in households where multiple occupants report adverse health effects. This suggests a process of social transmission whereby negative expectations and symptoms are discussed within the family, or through wider social networks. Research shows that simply hearing someone talking about their symptoms or observing someone exhibit symptomatic behaviour, such as wincing in pain, can result in the observer manifesting the same symptom.70 Symptoms such as dizziness, nausea and headaches have been shown to be particularly susceptible to social transmission in both experimental and real-world settings.71
In one innovative study, the experience of headache was elicited in a subset of a group of students visiting a research facility at an altitude of 3500 metres.72 All the students who experienced headaches had heard rumours about the risk of headaches at high altitude from a single study participant. This participant, known as the ‘trigger’, had been randomly chosen by the experimenters to receive information, prior to the trip, about the possible occurrence of severe headache at high altitudes. Results showed a significant increase in headaches in those who were vicariously exposed to this information through the naïve trigger, but not in the remaining students who remained unaware of the rumour. Further, the headaches were not a result of reporting bias. Tests indicated that the headaches were accompanied by biochemical changes – increased salivary prostaglandins and thromboxane – that caused the pain to worsen. Administration of a placebo ‘analgesic’ was shown to reduce this effect, by inhibiting the nocebo component of pain and prostaglandins synthesis. This study highlights that socially transmitted expectations can influence both symptom reporting and biochemical pain pathways.
The power of observation and modelling has also been investigated in experimental studies considering factors involved in mass psychogenic illness – that is, the collective manifestation of physical symptoms in the absence of an identifiable pathogenic cause.73 In one study participants were asked to inhale a suspected environmental toxin (actually plain ambient air). They were told the agent was known to provoke headache, nausea, itchy skin and drowsiness.74 The researchers had also enlisted actors (known in psychology as ‘confederates’) to pretend to be study participants. The genuine participants reported significantly more symptoms if they saw a confederate inhale the suspected toxin and feign the expected symptoms. Observing someone else modelling the expected ill effects amplified their own symptoms.
Evidence also indicates that medically unexplained pain and health complaints in children can sometimes be influenced by a parent modelling similar symptoms, which could explain why some children in windfarm communities have reported symptoms.75 Both experimental and clinical evidence therefore supports the likely role of social contagion in the transmission of symptoms attributed to windfarms.
Individual differences
Of course, not everyone who is exposed to negative health misinformation about windfarms will experience a nocebo response. This will depend on whether individuals are likely to accept, and be worried by, the narrative that windfarms cause health effects. The evidence from field research shows us that there are personality and attitudinal differences between those who do and do not report symptoms, and that these differences support the thesis that symptoms are triggered by negative expectations.
Most of us have experienced ‘negative’ people in our families, friendship networks and workplaces. Negative people cause discreet eye-rolling in others when they launch into their predictable whinging about all manner of things. Psychologists have studied this phenomenon and have developed various measurement scales and questionnaires to evaluate where people fall on the negative–positive personality spectrum. There are a number of negative-oriented personality traits. Neuroticism is a stable tendency to respond to threat, frustration or loss with negative emotions such as anxiety, worry, hostility or sadness.76 Negative affectivity reflects a propensity to experience elevated levels of distress over time and in diverse circumstances.77 Frustration intolerance is a tendency to be unable to cope with negative emotions, thoughts and events.78
People who report symptoms and attribute them to windfarms are more likely to view life through a negative lens and to experience more negative emotions over time. This was highlighted when an English research group investigated whether having a generally negative mindset was associated with negative feelings about ten small and micro wind turbines near two English cities.79 A relationship between perceived wind turbine noise and medically unexplained non-specific symptoms was only found in people who scored highly when assessed for negative-orientated personality traits (neuroticism, negative affectivity and frustration intolerance).
Effectively, the people attributing symptoms to windfarms are the same people who are likely to complain in other situations. There is consistent evidence that people who exhibit negative-oriented personality traits are more inclined to believe negative narratives about health, to notice and report symptoms consistent with perceived health threats, and to be more susceptible to illness by suggestion.80 Importantly, increased symptom reporting in this group is generally unrelated to objective markers of ill health.81
Negative attitudes to wind turbines and noise annoyance
Negative attitudes to wind turbines are associated with increased symptom reporting. In a recent study, residents living in the vicinity of wind turbines reported poorer sleep quality if they had a negative attitude to wind turbines, if they had concerns about property devaluation, and if they could see wind turbines from their property.82
As discussed in Chapter 4, there are also inter-relationships between reported annoyance with the noise produced by windfarms, psychological distress, and reports of stress-related symptoms such as dizziness.83 While noise annoyance is not closely related to any neurophysiological sensitivity to noise, it is consistently related to perceived noise sensitivity, which is a personality trait reflecting a predisposition to attend to and negatively evaluate noise.84 If annoyance were purely a reflection of the character of windfarm sound, or of the noise sensitivity of residents, we would not expect to see substantial variations in the proportion of people reporting noise annoyance across geographical locations. However, there is considerable variability in noise annoyance reported in field studies. An investigation conducted by Health Canada in relation to two Canadian provinces with equivalent residential noise exposure showed that 6.3 percent of Prince Edward Island respondents were highly annoyed by wind turbine noise, compared with 16.5 percent of respondents from Ontario.85 This indicates that situational and contextual variables are influencing annoyance reactions.
There is also evidence that noise annoyance is more strongly related to negative attitudes about wind turbines than to the actual level of noise exposure.86 Noise annoyance is associated with concerns about the health effects of windfarms, aesthetic objections to wind turbines, and simply knowing that the sound is caused by turbines.87 Increased noise annoyance is also associated with negative publicity about windfarm health effects, indicating that negative expectations play a role.88 The provincial differences seen between Prince Edward Island and Ontario may, at least in part, be explained by a propensity for media in Ontario to favour negative health stories about windfarms.89

Figure 5.1 Subject being contemporaneously exposed to infrasound and audible windfarm sound in the Acoustic Research Centre listening room.

Figure 5.2 Subject undergoing hearing screening test in the listening room with view into the sound control room.
Positive context
Finally, residents who have received economic benefit from a windfarm are likely to have more positive attitudes about windfarms and, correspondingly, are unlikely to be noise annoyed or to report symptoms, even at relatively high sound exposure. In fact in the recent large scale Health Canada study participants who did not receive personal benefits had 12 times higher odds of being annoyed by wind turbine noise.90 As we noted in Chapter 3, evidence suggests payment may be one protective factor against anti-windfarm rhetoric, and so an effective antidote to wind turbine syndrome.
A series of experimental studies
To test the broad hypothesis that increased annoyance and health complaints can be explained by negative expectations, we conducted a number of experimental studies. The experiments were performed at the Acoustic Research Centre at the University of Auckland, in a listening room built to international standards for experiments assessing subjective responses to sound (IEC268-13). Over the course of the studies, 246 people, ranging in age between 17 and 70 years old, took part in experimental procedures. We recruited healthy volunteers on the basis that when describing the onset of symptoms, complainants generally self-identify as previously healthy members of the community. Take for example the acute health effects described below:
Within twenty minutes … we each experienced unpleasant symptoms of motion sickness, including ear pressure, headache, nausea, dizziness, vertigo, especially when moving about …91
Over the course of the experiments participants were exposed to infrasound, or to infrasound overlaid with audible windfarm sound, and were asked to report on their current symptoms, mood, and annoyance reactions during two exposure sessions. During the sessions where infrasound was combined with audible windfarm sound, the infrasound at 9 Hz was transmitted at 50.4 dB, to replicate as closely as possible the pressure level at 9 Hz measured in field studies at a distance of 350 metres from wind turbines.92 Audible windfarm sound was transmitted at 43 dB, a level comparable to the maximum noise exposure level in New Zealand, as set by the windfarm noise standard NZS 6808:2010. The sound recording was taken from a location on a small road approximately one kilometre from the nearest turbine of a windfarm that consisted of 134 turbines (103 turbines of 660 KW and 31 turbines of 3 MW).
Sham controlled study
In the initial sham controlled double blind provocation study, 54 participants were exposed to ten minutes of infrasound and ten minutes of sham infrasound (actually silence), in counter-balanced order – that is, half the participants were exposed to genuine infrasound in their first listening session and sham infrasound in their second, and the remaining participants in the opposite order.93 However, participants were led to believe that they would be exposed to infrasound during both listening sessions. Participants were asked to evaluate the extent to which they experienced 24 physical symptoms, such as headache, nausea, and dizziness, on a scale from 0 (not at all) to 6 (extreme), both before and during listening sessions. The participants’ level of concern about the health effects of windfarm sound exposure was also assessed over the course of the experiment.
Prior to exposure, 27 participants viewed audio-visual material integrating information from the internet suggesting that people were experiencing symptoms when exposed to infrasound generated by windfarms (we will refer to this as the high expectancy group). The remaining 27 participants viewed material in which experts explained that infrasound exposure is an everyday experience and that infrasound produced by windfarms would not cause symptoms (the low expectancy group).
The high expectancy participants reported significant increases in the number and intensity of symptoms experienced during exposure to both real and sham infrasound, relative to the baseline level of symptoms they had reported before the listening sessions. This demonstrated that their symptom reports were provoked by expectations rather than as a result of infrasound exposure. Participants in the high expectancy group tended to report symptoms that had been suggested to them as typical symptoms of infrasound exposure, indicating that their symptom expectations were very specific. As predicted, this increased symptom reporting was associated with increased concern about the health effects of windfarms which developed in the high expectancy group over the course of the study. Importantly, participants in the low expectancy group exhibited no increase in symptom reporting during either listening session, further suggesting that symptom reporting in the high expectation group was a result of a nocebo response.
Building on these findings, our next experimental studies involved simultaneous exposure to sub-audible infrasound and audible windfarm sound during two discrete listening sessions.94 In keeping with the sham study, expectations were manipulated prior to the listening sessions by exposing participants to media sourced from the internet. As we found in the initial sham study that negative expectations formed from accessing information on the internet triggered symptoms during exposure to windfarm infrasound, our first follow-up study was designed to assess whether positive expectations could produce the opposite effect, in terms of a reduction in symptoms and improvements in reported health (Crichton, Dodd, Schmid, Gamble, Cundy et al., 2014). In this study 60 participants were randomly assigned to receive either positive or negative expectations prior to listening sessions. Negative expectation participants watched audio-visual material incorporating television footage about health effects said to be caused by infrasound produced by wind turbines. In contrast, positive expectation participants viewed material that explained infrasound exposure was a normal, natural experience, and also outlined the possible therapeutic effects of infrasound (there are infrasound producing devices promoted on the internet as alleviating the very symptoms windfarm infrasound is said to trigger).
We discovered that, during simultaneous exposure to audible windfarm sound and infrasound, symptoms and mood were strongly influenced by the type of expectations received. Negative expectation participants experienced a significant increase in symptoms and a significant deterioration in mood, while positive expectation participants reported a significant decrease in symptoms and a significant improvement in mood (Figure 5.3). At the conclusion of the experiment 90 percent of positive expectation participants reported that, during listening sessions, they had experienced an improvement in symptoms, while 77 percent of negative expectation participants reported a worsening of symptoms.
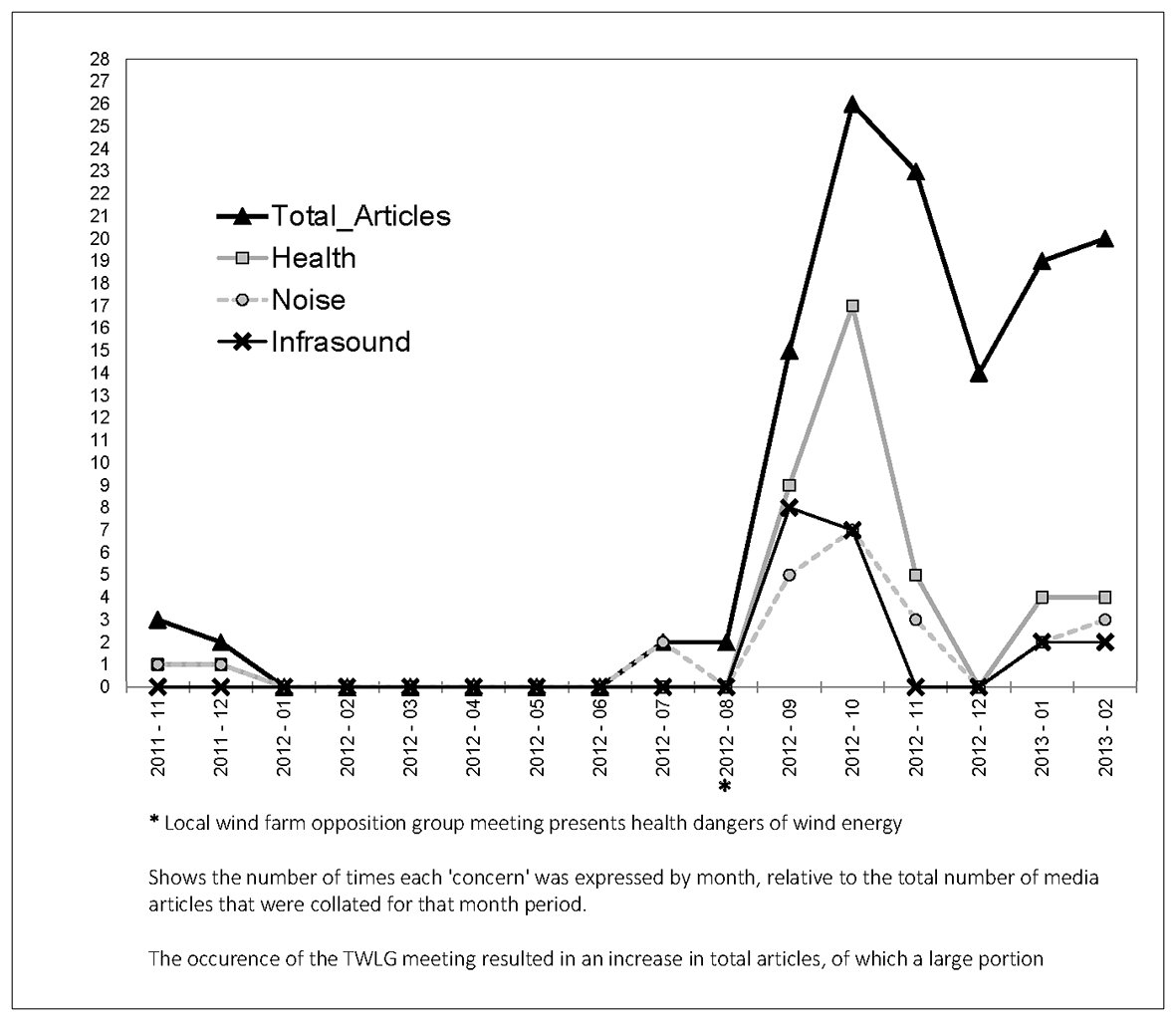
Figure 5.3 Incidence of negative news media mentions of health, noise and infrasound about the proposed Cherry Tree windfarm, Nov 2011–Feb 2013.
In further experiments we found that, once formed, negative expectations could be positively changed and symptom reporting reversed. This was achieved in one experiment by providing negative expectations before the first listening session, during which participants experienced a nocebo response, and by then delivering an alternative positive narrative before the second listening session.95 This positive narrative emphasised that infrasound was found throughout nature, had alleged health benefits, and exposure was actually a normal experience. We also found that creating positive expectations about infrasound had a buffering effect on the later delivery of negative health information about windfarms; so that, although nocebo responses in response to negative information occurred, they were blunted and less severe. Importantly, we also discovered that, after the initial delivery of negative expectations and consequent symptom reporting during the first listening session, we could reverse symptom reports by providing, before the second session, an explanation of the nocebo effect and its likely role in the participant’s symptomatic experiences.96 These findings provide preliminary indications that disseminating a more positive narrative about windfarms may protect against and improve symptom reporting in community settings.
Overall, across all the experiments, participants who were exposed to warnings about the purported health risks posed by windfarms consistently reported an increase in their symptoms and a deterioration in mood when exposed to windfarm sound. In fact, when participants were given only negative information about windfarm sound, without any counter-narrative, their symptom reporting increased over time, suggesting that their experiences were reinforcing their negative expectations, leading to further anxiety and heightened symptomatic responses. Importantly, however, their symptoms were reduced and their mood improved when infrasound was framed as simply sub-audible sound created by natural phenomena such as waves crashing on the shore or wind blowing through trees, with purported health benefits.
In light of evidence showing interrelationships between noise annoyance, distress, and stress related symptom reporting, reducing noise annoyance is an important strategy to optimise overall health benefits associated with windfarms.97 To this end we also examined whether negative expectations could be exacerbating annoyance reactions, and whether creating more positive expectations could help to reduce noise annoyance during exposure to wind turbine sound. Given that, as previously discussed, perceived noise sensitivity is said to constitute an underlying vulnerability to annoyance reactions, we also assessed the relationship between perceived noise sensitivity and noise annoyance, and whether expectations influenced that relationship. In keeping with studies of noise annoyance in windfarm communities98 participants evaluated their own noise sensitivity on a scale from not at all sensitive to extremely noise sensitive, before experimental procedures began. Again, positive and negative expectations were delivered prior to listening sessions using audio-visual presentations incorporating existing internet material.
We found that participants exposed to negative expectations were significantly more annoyed by windfarm sound than participants exposed to positive expectations, illustrating the potential for media and social narratives to influence noise annoyance in windfarm communities. Somewhat surprisingly, while perceived noise sensitivity predicted annoyance, this was only true for the negative expectation group. In other words, individuals in the negative expectation group experienced higher levels of noise annoyance if they were noise sensitive – while positive expectation participants were not annoyed by the sound, even if they were noise sensitive.
Tellingly, in each group, noise sensitivity was related to the participants’ experience of negative mood during sound exposure, but the influence ran in opposite directions. In the negative expectations group, participants who considered themselves more sensitive to noise experienced a more negative mood, including more worry, anxiety and distress. However, in the positive expectation group, noise-sensitive participants reported lower levels of worry, anxiety and distress. This suggested that these participants experienced significant relief from an underlying tendency to be anxious about the negative effects of sound exposure. This supports the view that perceived noise sensitivity reflects attitudinal and evaluative responses to sound, rather than sensory aspects of auditory processing.99 These findings are in keeping with other evidence that the context of environmental sound exposure can determine whether perceived noise sensitivity predicts annoyance reactions.100
Implications for windfarms
These results have important implications, as anti-windfarm campaigners often cite noise sensitivity as an intractable vulnerability to the negative effects of windfarm sound, and argue that this requires precautionary changes to the regulations governing the location of windfarms. Instead, our research suggests that the answer does not lie in regulatory change, as the vulnerability is not to the acoustic characteristics of windfarm sound. Rather, noise-sensitive individuals are more susceptible to negative suggestions about sound exposure, and, as a result, are more at risk of negative reactions triggered by the dissemination of misinformation about the health risk posed by windfarms. Importantly, our results suggest that creating more positive expectations about windfarm sound exposure should reduce annoyance reactions, even in noise-sensitive residents. This is also indicated by field evidence revealing that where people adopt positive attitudes to windfarms, this operates as a protective factor against annoyance, even if residents are noise-sensitive.101
Critically, we discovered that it is possible to reverse negative expectations after they are formed, and thereby alleviate annoyance and symptom complaints during exposure to windfarm sound. This is important if we are to address health complaints in the community. Results showed that nocebo responses were reversed when participants were provided with an alternative, positive narrative about the health effects of windfarm sound, whereby infrasound was depicted as a normal component of environmental sound and reference was made to the use of infrasound in therapeutic contexts.102
We also found that nocebo responses could be reversed by explaining to participants that their symptomatic experiences were prompted by negative expectations formed from viewing internet material suggesting that windfarms posed health risks.103 The way in which the nocebo effect was explained to participants was designed to normalise the nocebo response, eliminate blame, and ensure that their experience of symptoms was validated. Evidence demonstrates that if people feel they are not being believed or not taken seriously, they may become resistant to psychological explanations for their symptoms, and will therefore be more likely to persist with the belief that their symptoms have a biological cause.104
As we have previously discussed, brain imaging studies reveal that symptoms experienced as a result of nocebo responses are authentic experiences. Therefore, reversing negative expectations about windfarms is likely to be a vital strategy to address genuine suffering in windfarm communities. This highlights the need for responsible and careful framing of messages about windfarms: the aim should be to minimise anxiety and avoid creating unfounded negative expectations. Importantly, our experimental findings suggest that creating more positive expectations about windfarm sound may ameliorate health complaints and reduce annoyance in affected communities.
The first report of Australia’s National Wind Farm Commission,105 released in 2017 and discussed in Chapter 6, revealed that, in its first year of operation, all of the 46 complaints the commission received about operational windfarms related to just nine of the 76 existing farms in Australia. Further, there were only 42 complaints regarding 19 proposed windfarms. These are very small numbers relative to the numbers of residents living near windfarms across Australia. Field evidence indicates that generally, over time, residents develop more positive attitudes to windfarms in their community.106 However, in communities where anti-windfarm advocates are actively attempting to provoke anticipatory anxiety, there is a real risk that negative expectations will produce annoyance and symptoms.
Case study in fomenting anxiety
To understand how anti-windfarm advocates foment anxiety in communities, it is useful to consider a case study from rural Victoria.107 In 2011, Infigen Energy applied to construct and operate a 16-turbine windfarm known as Cherry Tree, near the top of a 550-metre ridge. Australian census data show that the three settlements nearest to the proposed windfarm had the following populations: Trawool (376 dwellings with 789 people), Whitehead’s Creek (9.5 kilometres away from the site, with 159 private dwellings and 373 people) and Seymour (12.7 kilometres away; 2923 dwellings with 6370 people).108
On 28 August 2012, a newly proclaimed local anti-windfarm group, the Trawool Valley Landscape Guardians (TWLG), organised a public meeting at Trawool, the small settlement nearest the proposed site. There was an estimated attendance of 100. The meeting was addressed by two residents (Donald Thomas and Noel Dean) who have property near the already operational Waubra windfarm, 230 kilometres by road from Trawool; Max Rheese, a member of the Australian Environment Foundation, an activist group sceptical about global warming and opposed to wind energy; and Steve Campbell, then chief of staff to Senator John Madigan, who at the time was minor party politician outspoken in his opposition to windfarms. A video produced by the Waubra Foundation was shown at the meeting, and a then-director of the foundation, Kathy Russell, was in attendance. Notes taken at the public meeting by an attendee were provided to us, and two news reports highlighted points made by speakers.
In 2013, the Victorian Civil and Administrative Tribunal (VCAT) conducted a hearing to consider objections to the proposed windfarm. In the months prior to this hearing, we documented examples of negative information disseminated through the news media, online, and through other channels.
We obtained all media coverage of the proposed windfarm from a commercial media monitoring company (iSentia) for the period between 9 November 2011 and 28 February 2013. This covered the period from the public announcement of the proposal until soon after the commencement of the VCAT hearings. We also searched Google News for the same period, using combinations of the search terms ‘Cherry Tree’, Cherry Tree, Infigen (the wind company), and ‘windfarm’. The records retrieved included news, letters and editorials from local, state and national newspapers, but not local radio or state-wide television. We examined this material for any negative content about noise and/or health issues, which we then grouped into free broad categories, namely expressions of concern or direct assertions that:
- the windfarm would have a direct impact on human health (‘Health’)
- the windfarm would generate audible noise that would cause annoyance or affect residents’ quality of life (‘Noise’)
- the windfarm would have a direct impact on human health through inaudible noise in the infrasonic range (‘Infrasound’).
As we have discussed, the internet provides ready access to an abundance of claims about diseases and symptoms said to occur in humans and animals exposed to wind turbines (see Appendix 1). On 21 August 2014, we conducted a Google search using five different search strings likely to be used by anyone seeking broad information about windfarms and health. Jessica Lee has analysed search engine data and shown, among other things, that the first page of Google results account for 33 percent of all reader click-throughs. We weighted the results of our searches using Lee’s click-through data,109 and calculated the probabilistic click-through rankings of the top ten sites returned by each of the five searches. (For more details, see our open-access paper.110)
We also searched submissions made to VCAT, which are public documents. We examined 75 opposing submissions for any mention of health concerns, and recorded other concerns. Multiple concerns were recorded separately and the postcodes of the writers were recorded. We provide illustrative examples of these concerns in Table 5.2 below.
| Quote | Source |
|---|---|
| ‘After attending the urgent community meeting regarding the Cherry Tree windfarm proposal, we are now more than ever gravely concerned members of the community’ | Letter from four residents. Seymour Telegraph, 12 September 2012. |
| ‘The major concern of the audience was health including sleep deprivation, increased blood pressure, heart racing, nosebleeds and constant headaches derived from the noise, vibration and infrasound produced from the 160m turbines’ | Seymour Nagambie Advertiser, 4 September 2012. |
| ‘Headaches, wanting to vomit all the time, pains in the chest, blood pressure, can’t sleep, sleeping tablets do nothing for you’ | Resident featured in a Waubra Foundation video screened at the Trawool meeting. |
| ‘Really bad chest pains in the night, and a lot of blood noses, I’d be asleep and then wake up, and my nose would be bleeding. It’s just pretty scary stuff’ | Resident featured in a Waubra Foundation video screened at the Trawool meeting. |
| ‘Symptoms have been consistently reported in Australia, up to 10 kilometres from homes. Most symptoms disappear when people leave the area, or when the turbines are switched off | Waubra Foundation video screened at the Trawool meeting. |
| ‘[There’s] not a single credible research paper in the peer reviewed literature stating that chronic wind turbine noise is harmless to human health but there is now over a dozen peer reviewed papers that say the opposite’ | Max Rheese, climate change sceptic and windfarm opponent, at the Trawool meeting. |
| ‘It’s the most bizarre thing. It just sounds so weird but you lay down and you can hear the turbines in your pillow’ | Waubra resident Donald Thomas at the Trawool meeting |
Table 5.2 Illustrative examples of negative statements about windfarms and health from news media and public meeting convened by opponents.
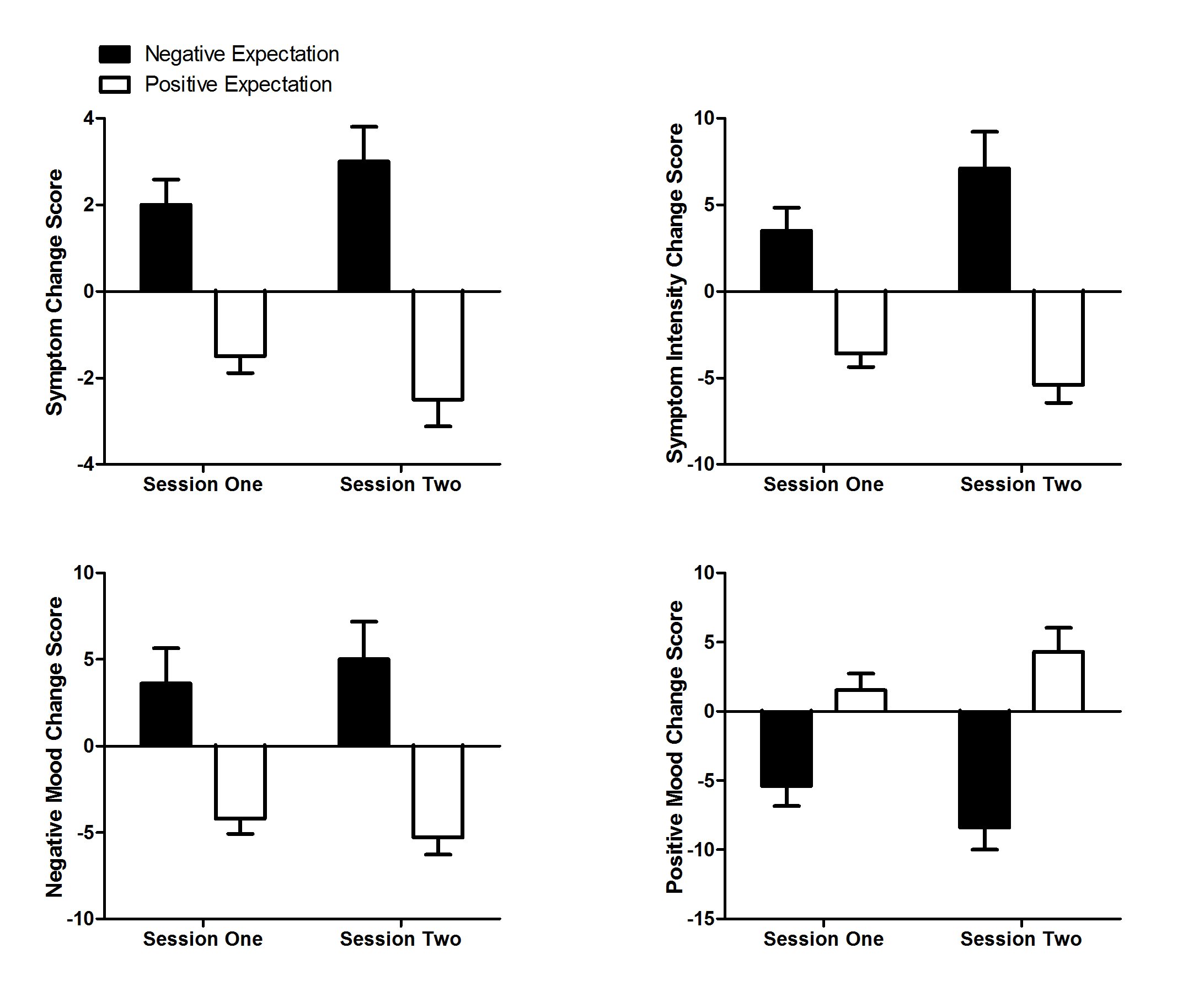
Figure 5.4 Changes from baseline in symptom number, symptom intensity, and mood scores. Source: Crichton, Dodd et al. 2014.
Dissemination of negative information in the local community
Of 126 media articles retrieved, 41 (33 percent) contained concerns about the health impacts of the proposed windfarm. Ninety-five percent of these were published after the anti-windfarm meeting organised by TWLG in August 2012. Figure 5.4 shows the number of times each concern was expressed in the collated media content, along with the total number of articles, and a marker showing the timing of the TWLG meeting.
Negative information from the internet
Using our five different search strings, 27 different sites were retrieved in the top ten hits thus returned. Of these, eight (30 percent) were stories or pages that described the alleged negative health impacts of windfarms, and two were ranked in the top ten weighted click-ranked sites.
Submissions to VCAT
There were 75 submissions made to VCAT from 53 households (several households sent separate submissions by different family members). Of these 53 households, 14 were in Trawool households (representing 3.7 percent of Trawool residences), 16 from Whitehead’s Creek (10.1 percent of residences) and 13 from Seymour (0.4 percent of residences). Three were sent from Melbourne addresses (110 kilometres away) and two from known anti-windfarm activists in other states. The remaining five were from hamlets at direct distances ranging from 4.6 to 26.4 kilometres from the proposed site.
All but one submission mentioned health concerns, with reduced visual amenity and bird deaths also being commonly mentioned. Thirty-three (44 percent) of submissions together named 28 different symptoms or health concerns, with the most common being sleep problems (17 mentions), headache/migraine (11), anxiety (9), stress (8), tinnitus (6), and memory loss, nausea and hypertension (5 each). (Table 5.3)
| Concerns expressed | N (% of submissions) |
|---|---|
| Health related | |
| General concern about health impacts | 74 (99) |
| Concern that sound or noise will cause health impacts | 58 (77) |
| Specific symptoms, illnesses named | 33 (44) |
| Anticipated abandonment of home | 17 (23) |
| More research needed on health impacts | 17 (23) |
| Blade glint/ shadow flicker | 14 (19) |
| Concerns pre-existing illness will worsen | 11 (15) |
| Electromagnetic interference | 10 (13) |
| Comparisons with tobacco, asbestos or lead as previously benign re health | 4 (5) |
| Economic impact | |
| Visual amenity marred | 57 (76) |
| Fire risk | 47 (63) |
| Traffic and access problems | 37 (49) |
| Loss of tourism | 21 (28) |
| Decline in local business | 15 (20) |
| Other | |
| Fauna deaths (esp. birds) | 64 (85) |
| Flora destruction | 37 (49) |
| Community divisiveness | 16 (21) |
| Concern over wind company’s multi-national status | 15 (20) |
| Belief windfarms are uneconomic | 12 (16) |
Table 5.3 Concerns expressed in 75 submissions opposing the windfarm development.
Across the 75 submissions, there were many examples of people expressing concern after having been exposed to alarming, negative claims and testimonies from victims, scientists and doctors. These were often sourced from the anti-windfarm movement, particularly the Waubra Foundation, and from the TVLG public meeting.
For example, from a chiropractor:
After reading and hearing many accounts of anecdotal evidence given by people living within the vicinity of the wind turbines we are concerned that the turbines may impact on our health. Although we were unable to find any published research on the health problems associated with wind turbines we feel that it better not to take the risk until appropriate research is carried out. Innumerable letters and reports have been written by general practitioners who have witnessed first-hand the negative effects of wind turbines on the health of patients in their community. The results are alarming to say the least.
Many submission writers mentioned that they had met people who claimed to have been made ill by turbines: ‘seeing how sick people have become horrifies us’. Many also referred to ‘research conducted by the Waubra Foundation’, despite the organisation having recently declared that they do not conduct medical research:
From research from the conducted Waubra Foundation [sic] and international acoustic technicians, we know that the following medical conditions have been identified in people living, working or visiting within 10km of operating wind turbines.
No submissions showed awareness that nobody involved with the Waubra Foundation has conducted any research authorised by a human ethics review committee, nor published any research on the area in an indexed peer-reviewed journal.
As we saw in Chapter 3, windfarm opponents have circulated the factoid that ‘over 40’ Australian families have abandoned their homes.111 ‘Walking off farms’ was mentioned in 17 submissions (23 percent): ‘This is evidenced by the fact people are walking off their farms and leaving their houses as a result of the health effects’ and ‘I believe at this stage that there is too much evidence of people becoming sick and even having to walk off of their land in other areas because of the negative effects of the turbines’. Those leaving were said to include turbines hosts: ‘People who have permitted to have put wind turbines on their property, have had to leave their homes because of illness, problems sleeping and noise.’ One submission threatened abandonment before any adverse effects were experienced: ‘I won’t wait to become sick, I would leave’.
The spectre of a distant and venal transnational corporation putting profits over local residents’ health was raised in 20 percent of submissions. The company concerned, Infigen, operates windfarms in Australia and the USA.
One must ask the question of what is more important – that a multi-national corporation generates higher profits or that the mental and potentially physical health of the local community is compromised by allowing the wind farm to operate in this location.
(Significantly, Australia’s only community-owned windfarm at Leonards Hill, also in Victoria, was not spared opposition despite its ownership structure.)
Three quarters of submissions expressed concern that existing health problems would be exacerbated:
My eldest son and mother-in-law suffer from severe migraine headaches, often brought on by changes in air pressure, always exacerbated by any loud or ongoing noise. The noise from the wind turbines would make their condition unbearable.
One submission referred directly to claims made by the two Waubra residents who had addressed the meeting: ‘One man got sick and he sold his farm because the wind turbines made him sick. The other man could hear the wind turbine noise in his pillow’.
Our results described the dramatic increase in expressed concerns about health and other issues published in local news media immediately following a public meeting organised and addressed by dedicated opponents of windfarms from outside the area. The meeting exposed the small proportion of local residents in attendance to a powerful mixture of sometimes emotional testimony from two complainants from another community, and to contributions from the Waubra Foundation presumably intended to provoke health concerns in those attending and their social networks. Our data also show that anyone searching the internet in Australia for information on health and windfarms will readily find negative material published by opponents.
Confirmation bias is a well-documented cognitive heuristic whereby people search for, interpret, and prioritise information in ways that confirm their beliefs.112 If individuals have been primed by exposure to events like the Trawool meeting to understand that windfarms threaten health, subsequent searches for information may see confirmation bias operate and lead them to select information that is consonant with their existing negative beliefs.
Victim testimony can be a powerful ingredient in fomenting anxiety in those exposed to their claims. As was noted in a study of Dutch media coverage, ‘Scientists, technicians and experts get significantly less space, than laypeople, government, industry and interest groups, in media coverage of EMF health impacts’. In reporting on the proposed windfarm, local news media highlighted the testimony of purported victims:
Mr Dean said he suffered balance-related problems which he believed were caused by low frequency sound waves generated turbulence created by wind coming into the turbines. He had suffered head pains, tinnitus and muscle spasms. He had sold most of his land ‘and got the hell out of there’ telling the audience ‘I hope other people don’t have to go through what we’ve gone through.’113
During the meeting, an audience member thanked the speakers and said, ‘I think it’s been extremely informative. A lot of the health issues have come out that we probably weren’t aware of.’ The meeting provided attendees no exposure to the many who live near windfarms who have no noise or health complaints. A selection of such people from the Waubra area can be seen in a video produced by Vic Wind,114 featuring landowners talking about their experiences of hosting turbines. Instead, the Trawool public meeting provided a concentrated and memorable set of highly negative claims. This was followed by a surge in local media reporting, although only one third of this raised concerns about noise or health. In total, only 53 of the 3458 residences (or 1.5 percent) in Trawool, Whitehead’s Creek and Seymour submitted objections to VCAT.
In the submissions that were submitted, there was considerable evidence of shared or identical wording. Six contained an identical paragraph disputing the wind company’s statement that the noise of wind turbines would be comparable to background noise at a beach. These similarities suggested there had been networking between opponents.
VCAT allowed the windfarm to proceed. Of the health considerations raised by opponents, VCAT rejected the hypotheses that wind turbines directly cause adverse health outcomes, implying instead that psychogenic factors were relevant to understanding such experiences:
The Tribunal has no doubt that some people who live close to a wind turbine experience adverse health effects, including sleep disturbance. The current state of scientific opinion is that there is no causal link of a physiological nature between these effects and the turbine … The totality of material before the Tribunal suggests, but does not conclusively prove, that these effects are suffered by only a small proportion of the population surrounding a wind farm … The position now, as then, stated by the NHMRC in summary, is that there is no evidence that wind turbines cause adverse health effects.115
Every Australian planning case to date considering the issue of ‘wind turbine syndrome’ has found the evidence offered by proponents of the disease to be insufficient.116
Finally, it is interesting to compare the Cherry Tree windfarm development with the Coonooer Bridge windfarm, developed and approved at approximately the same time in Victoria. The latter utilised a community sharing model to distribute income equitably among neighbours. A scientist from the CSIRO noted of the difference between the two projects: ‘When we dug a little deeper, we often found their opposition was based more on concerns about process’.117 Although our research shows the clear impact of the activities of anti-windfarm groups on the expression of health concerns, further research may shed light on what inspires both acceptance rather than resentment.
1Knopper and Ollson 2011.
2Leslie 2000.
3Covello and Sandman 2001.
4Sandman 1989.
5Sandman 1991.
6I applied these to a case study of mobile phone tower complaints in the 1990s. See Chapman and Wutzke 1997.
7McCluskey, Kalaitzandonakes and Swinnen 2016.
8Eldridge-Thomas and Rubin 2013; Leslie 2000.
9Leventhall 2006; Leventhall 2007; Leventhall 2013.
10Leventhall 2006.
11Leventhall 2007.
12Leventhall 2006.
13Leventhall 2013.
14Leventhall 2013.
15Evans, Cooper and Lenchine 2013.
16Leventhall 2013; Munk 2014.
17Dechene, Stahl, Hansen and Wanke 2010.
18Leventhall 2017.
19Johnston 2009.
20Abrams 2013.
21Bastasch 2014.
22Murray 2014.
23MacGregor and Fleming 1996.
24Boykoff and Boykoff 2015.
25Knapton 2015.
26Devlin 2014.
27Deignan, Harvey and Hoffman-Goetz 2013.
28Deignan and Hoffman-Goetz 2015.
29Australian Broadcasting Corporation 2015.
30Baxter, Morzaria and Hirsch 2013; Mroczek, Banas, Machowska-Szewczyk and Kurpas 2015.
31Moore 2013.
32Danker-Hopfe, Dorn, Bornkessel and Sauter 2010.
33Petrie et al. 2005.
34Pennebaker and Skelton 1981.
35Petrie, Faasse, Crichton and Grey 2014.
36Pennebaker 1994.
37Moss-Morris and Petrie 1999.
38Hahn 1997.
39Benedetti, Durando and Vighetti 2014.
40Benedetti, Lanotte, Lopiano and Colloca 2007. A useful and entertaining explanation of the nocebo effect is available on YouTube, and had nearly 5.7 million views as of May 2017: http://bit.ly/2ciSTSc.
41Enck, Bingel, Schedlowski and Rief 2013.
42Rosenzweig, Brohier and Zipfel 1993
43Rief, Avorn and Barsky 2006.
44Wells and Kaptchuk 2012.
45Schmid et al. 2013.
46Maugh 1982.
47Page et al. 2006.
48Bacon [1597] 2005.
49David and Wessely 1995.
50Petrie and Wessely 2002; Spurgeon 2002.
51Rubin, Cleare and Wessely 2008.
52Rubin, Nieto-Hernandez and Wessely 2010.
53Rubin et al. 2010.
54Landgrebe et al. 2008.
55Moss-Morris and Petrie 1999.
56Hamilton 2014.
57Thorne 2011.
58Phillips 2011.
59Commonwealth of Australia 2015c.
60Houtveen and Oei 2007.
61Walentynowicz, Bogaerts, Van Diest, Raes and Van den Bergh 2015.
62Jalali et al. 2016.
63Chapman 2014b.
64Page et al. 2006.
65Ferrucci et al. 2011.
66Petrie and Wessely 2002.
67Winters et al. 2003.
68Witthoft and Rubin 2013.
69ten Veen, Morren and Yzermans 2009.
70Faasse, Grey, Jordan, Garland and Petrie 2015.
71Broderick, Kaplan-Liss and Bass 2011.
72Benedetti et al. 2014.
73Lorber, Mazzoni and Kirsch 2007.
74Mazzoni, Foan, Hyland and Kirsch 2010.
75Osborne, Hatcher and Richtsmeier 1989; Wolff et al. 2010.
76Goldberg et al. 2006; Taylor et al. 2013.
77Watson and Pennebaker 1989.
78Harrington 2005.
79Taylor et al. 2013.
80Petrie, Moss-Morris, Grey and Shaw 2004; Put et al. 2004.
81Pennebaker 1994.
82Jalali et al. 2016.
83Michaud et al. 2016b.
84Schutte, Marks, Wenning and Griefahn 2007.
85Michaud 2015.
86Pedersen and Waye 2004.
87Magari, Smith, Schiff and Rohr 2014; Pedersen, van den Berg, Bakker and Bouma 2009; Van Renterghem, Bockstael, De Weirt and Botteldooren 2013.
88Crichton, Chapman, Cundy and Petrie 2014.
89Deignan and Hoffman-Goetz 2015.
90Health Canada 2015.
91Ambrose, Rand and Krogh 2012.
92Turnbull et al. 2012.
93Crichton, Dodd, Schmid, Gamble, Cundy and Petrie 2014.
94Crichton, Dodd, Schmid, Gamble and Petrie 2014; Crichton, Dodd, Schmid and Petrie 2015; Crichton a Petrie 2015a, 2015b.
95Crichton and Petrie 2015a.
96Crichton and Petrie 2015b.
97Michaud et al. 2016b.
98Pedersen and Persson Waye 2007.
99Ellermeier, Eigenstetter and Zimmer 2001.
100Oiamo, Baxter, Grgicak-Mannion, Xu and Luginaah 2015.
101Pedersen et al. 2009.
102Crichton and Petrie 2015a.
103Crichton and Petrie 2015b.
104Liden, Bjork-Bramberg and Svensson 2015.
105Office of the National Wind Commissioner 2017.
106Wilson and Dyke 2009.
107This account is based on a paper first published in 2014 and co-authored with my colleagues Ketan Joshi and Luke Fry: Chapman et al. 2014.
108This short video shows views from the planned site for the 16-turbine, 50 megawatt windfarm: http://youtu.be/JpxNcTCWXIQ
109Lee 2013.
110Chapman et al. 2014.
111Chapman 2014b.
112Klayman 1995.
113Sonti 2012.
114See http://www.windalliance.org.au/waubra-videos.
115Bergin 2014.
116Barnard 2014.
117Green 2013.