22
Learning from two decades of CQI research in Indigenous PHC
Aboriginal and Torres Strait Islander Australians have demonstrated extraordinary cultural strength, adaptability and resilience across time. Vital for the continuing improvement of health outcomes is research that produces the knowledge, processes, tools and resources to enable communities, health practitioners, other service providers and policymakers to improve health care, prevent disease and support wellbeing. Shifts in health research approaches, as described in the previous chapter, have been complemented by significant changes to Indigenous health policy.1
Our CQI research network has learnt from and contributed to these efforts. Early quality improvement research played an important role in testing the acceptability of CQI approaches and their effect on Indigenous PHC.2 Important gains have since been made. Quality improvement efforts in PHC have been accelerated and strengthened at multiple levels and contexts.3 Clinical performance assessment and improvements have been achieved across a range of services4 and structured health service and systems assessments have been facilitated to support best practice.5 Quality improvement has increasingly focused on the social, cultural, structural and environmental factors that influence health.6 As this work has progressed, research teams have adopted a broader agenda to embed Aboriginal and Torres Strait Islander leadership, participation and priorities in health and wellbeing research. Network members have created spaces to safely share their experiences from different viewpoints and learn from each other. These developments are essential for bringing about meaningful change and lasting benefits for communities.
This chapter shares lessons learnt by the research network, which brings together Aboriginal and Torres Strait Islander and non-Indigenous stakeholders to improve healthcare equity. Drawing on publications from network members, we describe some of the structures and mechanisms that are being used to foster culturally safe, strengths-based and transformative PHC and quality improvement research among Aboriginal and Torres Strait Islander communities in Australia. The lessons learnt have informed the principles of CQI implementation and research, and may offer insights for others seeking to improve equity and justice through research.
Building on strengths to transform research
Research networks provide a forum for experimentation and knowledge creation, information exchange and the spread of good ideas and practice. They can be useful in addressing complex issues or “wicked” problems when solutions go beyond the control and scope of any one agency.7
Research networks . . . can be useful in addressing complex issues or “wicked” problems when solutions go beyond the control and scope of any one agency.
Our CQI research network in Aboriginal and Torres Strait Islander PHC has had several iterations (see overview in Chapter 9). Since 2015, the network has used an “innovation platform” approach. Leaders of large-scale change have argued that innovation platforms create an opportunity for people working in different parts of the system to tackle challenging issues together,8 including entrenched systemic problems.
Centre for Research Excellence in Integrated Quality Improvement
The vision of the Centre for Research Excellence in Integrated Quality Improvement (CRE-IQI) innovation platform, which was funded from 2015 to 2019, was to accelerate and strengthen large-scale primary healthcare quality improvement efforts. To achieve this vision, stakeholders from multiple roles and organisations were brought together to work on shared goals, find solutions to common quality improvement problems, learn from each other, and take collective action. The elements of the CRE-IQI innovation platform are shown in Figure 22.1.
Members included Indigenous and non-indigenous clinicians, researchers, policy and project managers from health services (including community-controlled organisations), regional service support organisations, national support organisations, universities, research institutes and government. As an “open platform”, the CRE-IQI encouraged new partnerships and collaborations and provided a vehicle for integrated research and knowledge translation.9
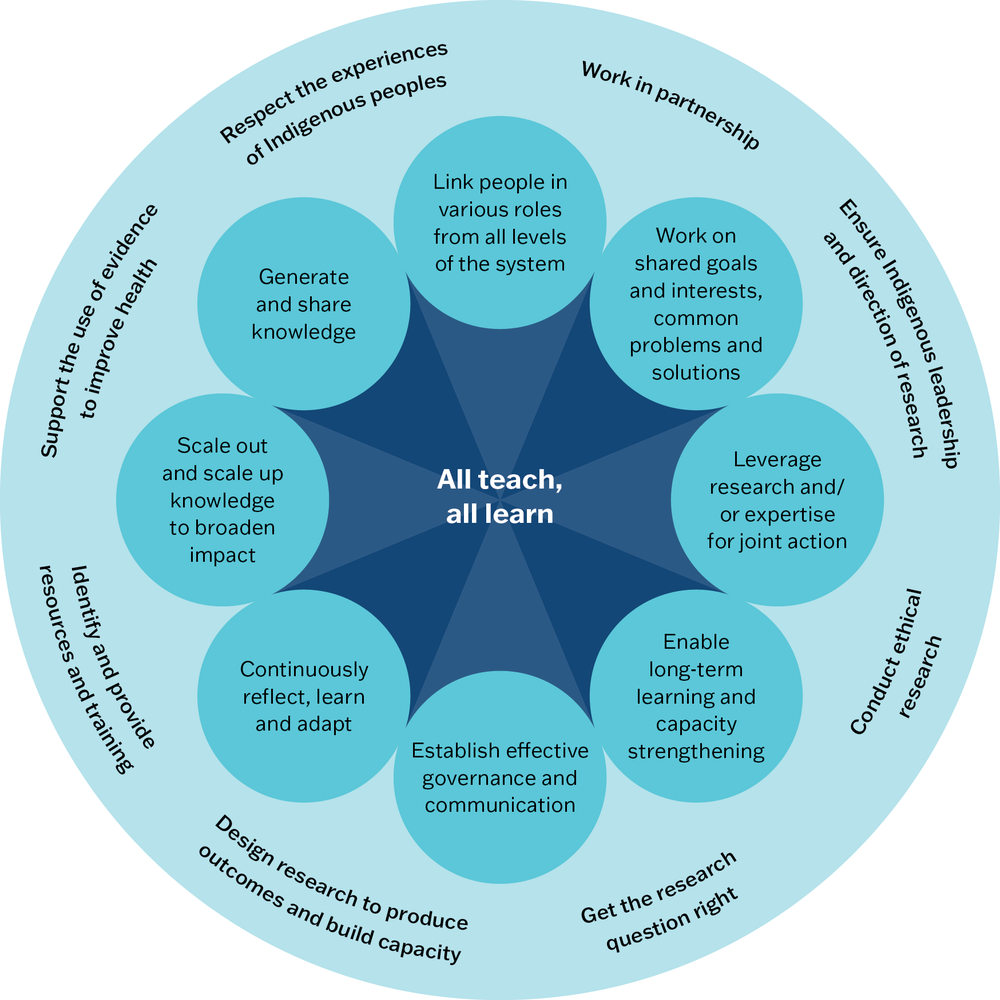
Figure 22.1 Elements of the CRE-IQI innovation platform. Source: A. Laycock, Conte et al. 2020.
“All teach, all learn” approach to research capacity strengthening
One of the goals of the CRE-IQI was to increase the capacity of members to participate in and lead CQI research. It was recognised that this involved capacities for building research skills and confidence, taking ownership and leadership, collaborating, forming research partnerships and working in a culturally safe way, translating research, and building structures and resources.10
The CRE-IQI developed a model that drew on capacity strengthening11 and evidence from capacity building for quality improvement12 to theorise strategies for strengthening CQI research capacity in Aboriginal and Torres Strait Islander PHC.13 Consistent with the way of working across the research network, an “all teach, all learn” maxim was adopted. “All teach, all learn” embodies the value placed upon mutual learning, where all involved – Aboriginal and Torres Strait Islander and non-Indigenous people, those involved in primary healthcare services, the communities they serve, early career and experienced researchers – are learners and teachers. The strengths-based process used for developing the model identified the need to tackle power imbalances, cultural contexts, relationships, systems requirements and the existing knowledge, skills and experience of all involved to strengthen research capacity.14
Four principles were identified for implementing an “all teach, all learn” approach to CQI research capacity strengthening across the network: mutual or two-way learning; Indigenous leadership as core; sharing power and facilitating relationships; resourcing and continuous improvement. The principles are expanded in Box 22.1.
Box 22.1 Principles of the “all teach, all learn” approach to strengthening capacity for CQI research
Mutual or two-way learning
At the core of the “all teach, all learn” motto is the valuing of Indigenous cultures, knowledge and expertise alongside Western research and knowledge, and recognition that different kinds of capacities are to be developed in different people, processes, organisations and systems. These capacities are influenced by worldview, knowledge, experience and relationships.15 In the Australian context, mutuality requires valuing Aboriginal and Torres Strait Islander voices, identities and knowledge, and recognising the power held by decision-makers, institutions and structures to improve or undermine Indigenous health.16
Indigenous leadership as core
“Indigenous-led research” refers to research that is led and driven by Indigenous researchers, practitioners, policymakers and communities in partnership with community organisations, or through collaborative approaches involving Indigenous community or communities at each stage of the research process.17 Co-leadership arrangements can bring diverse knowledges in the same way as traditional distributed leadership models. Co-leads are researchers, community members, service providers, and policymakers of varying seniority or position, who support mutual strengthening of research capacity. These co-lead arrangements require culturally safe spaces.
Sharing power and facilitating relationships
A commitment to Indigenous leadership brings considerations and tensions to negotiate collectively for mutually beneficial outcomes. Methodologies that seek to support and value Indigenous knowledge within CQI research, and involve Indigenous people and their interests, are necessary. For non-Indigenous people in leadership roles, this means leading in partnership with Indigenous people and organisations, relinquishing and sharing power over research ownership and associated decisions, processes, outcomes and benefits. Indigenous ownership and respectful relationships from the outset of research enhance the likelihood of research relevance and thus translation and benefit.18 Allowing sufficient time for building meaningful relationships is essential for quality research and is an activity itself within strengthening research capacity, as it enables respectful engagement with Indigenous knowledge and perspectives.19
Resourcing and continuous improvement
Resources (especially staffing) are required to enable the communication, relationships, engagement and training that facilitate the strengthening of capacity for CQI research. Likewise, resourcing and continuous learning are essential to enable co-leadership, which is generally an additional responsibility for busy Indigenous translators, leaders or researchers, or those who combine these roles. Implementation is the responsibility of all within the Centre. A continuous improvement approach is used to test application of the program logic for research capacity-strengthening across the research programs and activities, and to monitor progress against the CQI–research capacity-strengthening priorities.20
Guiding principles
When the CRE-IQI was funded in 2015, members agreed that the research network should have an agreed set of operating principles, to guide how Aboriginal and Torres Strait Islander research values21 would be put into practice in quality improvement research. The principles were adapted, with permission, from a cancer research collaboration in Aboriginal and Torres Strait Islander health, as follows:
- respect the past and present experiences of Indigenous people
- work in partnership
- ensure Indigenous leadership and direction of research – in all stages of the process
- conduct ethical research
- get the research question right
- design research that will be feasible, produce outcomes and build capacity
- identify and provide the right resources and training
- establish systems and practices to support the application of evidence to improve Indigenous primary health care and health outcomes.
Published literature offered little in the way of critical reflection to support the implementation of such principles. The CRE-IQI’s management group undertook to evaluate how the principles were implemented and the outcomes over the research network’s lifespan.
Evaluating the implementation of the Centre for Research Excellence in Integrated Quality Improvement
Four approaches were used to evaluate the implementation of the CRE-IQI: developmental evaluation; principles-focused evaluation; social network analysis; and framework analysis (Box 22.2).22 While the resources and expertise required to evaluate this network were considerable, data sources were leveraged for multiple purposes to create efficiency and avoid “evaluation fatigue” amongst participants.
Box 22.2 Approaches used to evaluate the implementation of the
innovation platform
Developmental evaluation
Developmental evaluation can inform the development and adaptation of innovative and emergent initiatives in complex social environments. The approach uses systems thinking to consider how multiple parts of complex and dynamic systems (such as healthcare systems) are interrelated, focusing on users and use of evaluation findings. In addition to the innovation niche, developmental purpose, systems thinking and utilisation focus, the features of developmental evaluation include a complexity perspective, evaluation rigour, co-creation and timely feedback.23
Principles-focused evaluation
Principles-focused evaluation, like developmental evaluation, is an approach rather than a methodology. It examines “(1) whether principles are clear, meaningful and actionable, and if so, (2) whether they are actually being followed and, if so, (3) whether they are leading to the desired results.”24
Network analysis
Social network analysis is a set of techniques to map, measure and analyse social relationships between people, teams and organisations.25 Survey methods and software tools are used to collect, visualise, document and analyse interaction data to understand a group’s social structure, relationships and interaction patterns.
Framework analysis
Framework analysis is a form of thematic analysis in which an organised structure of concepts or themes is used to analyse data. For example, a framework designed to guide the development or evaluation of quality improvement collaboratives may be used to map and analyse communication, social systems, time span and innovation within the research collaborative, thereby increasing understanding of how the collaborative works and of its strengths and weaknesses.26
Applying different methodologies enabled the network to respond promptly to the “emergent” nature of a research system that was complex and dynamic. Together, the four evaluation approaches provided a nuanced understanding of how the collaboration was formed, how it worked, what changes were needed as work progressed, and what it achieved. This would have been difficult to achieve with any single evaluation approach.27 Specific projects associated with the CRE-IQI were also evaluated using impact and economic evaluation methods28 and developmental evaluation.29 The learning that may be drawn from the evaluation of the CRE-IQI innovation platform is an example of how complex research collaborations in health may be evaluated, strengthened and reformed.
Developmental evaluation use and findings
Developmental evaluation was used to inform and support the formation, functioning and outcomes of the CRE-IQI. Innovation platforms have continuous reflection, learning and adaptation as a specific design principle. As developmental evaluation emphasises continuous learning and adaptation, it was well aligned. While rigorous in its use of multiple data sources and varied methods, the developmental evaluation provided scope to move away from a “what is planned needs to be achieved” mindset to one that could continually adapt based on what we were learning and how the collaboration was evolving.
We found the developmental evaluation approach suited to a research collaboration aimed at integrating quality improvement efforts at different levels of the health system in a complex PHC environment. Use of systems thinking (a key principle of developmental evaluation) and attending to relationships and interactions between CRE-IQI members provided insights into how CRE-IQI strategies and processes could be modified to work more effectively. Timely feedback (both opportunistic and at predetermined times) ensured that evaluation data was used to test modifications and make further improvements.30
Developmental evaluators need to become embedded within projects to build and maintain evaluator–team relationships, and to know and respond in real time to the evaluation context and innovators’ concerns.31 Having a member of the CRE-IQI staff team in the lead evaluator role met those needs.
Principles-focused evaluation use and findings
A principles-focused evaluation approach enabled critical reflection on how, to what end and whether the guiding principles of the CRE-IQI were being implemented. Interviews with collaboration members and review of documents generated themes that were iteratively discussed with the wider membership, refined and categorised into “strategies” – activities by which implementation of our guiding principles were recognised; “outcomes” – results seen from implementing the principles; and “conditions” – aspects of the context that facilitated and constrained implementation of the principles.32
Five strategies were identified as supporting implementation of the principles: honouring the principles, sharing and dispersing leadership across the collaborative, collaborating purposefully, adopting a culture of mutual learning, and being dynamic and adaptable.
“You have to operationalise [the principles] in some way . . . you’ve done that . . . reemphasising that these are not static . . . they have to be continually evolving as the work and people and new issues emerge.” – researcher, Indigenous, university/research institute33
Outcomes included increased Indigenous leadership and participation, the ability to attract principled and values-driven researchers and stakeholders, and the development of trusting and respectful relationships.
“I feel like I trust all those [long- standing researchers] that have been around. I trust their values – that you want to be involved with researchers who have similar values.” – health service manager, non-Indigenous, Aboriginal community controlled health service34
The conditions that facilitated the implementation of the principles were collaborating over time, an increasing number of Indigenous researchers participating in the network and taking an “innovation platform” approach. 35 The strategies, outcomes and conditions are brought together in Figure 22.2.
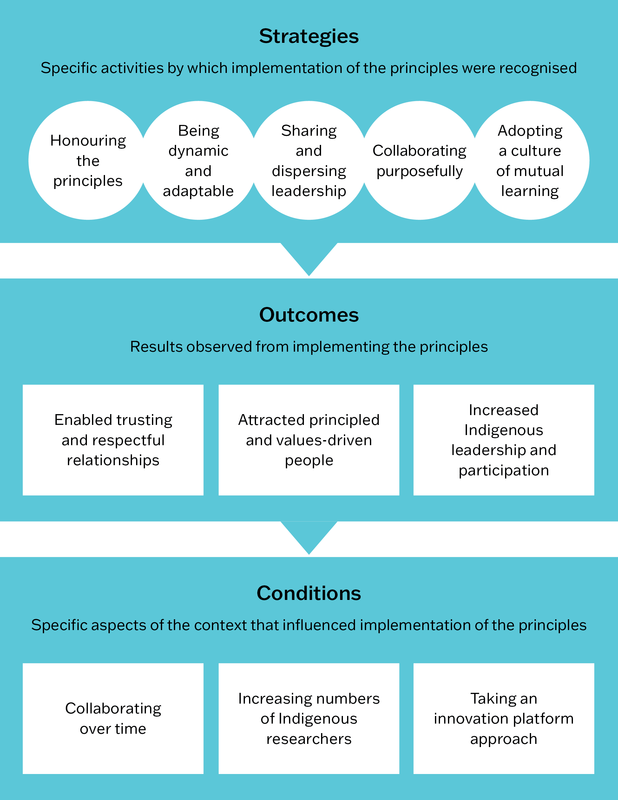
Figure 22.2 Strategies, outcomes and conditions related to how principles were implemented in the research collaboration. Source: J. Bailie, Laycock et al. 2021.
Having collaboratively developed principles held genuine meaning for members and was important for guiding the network: the principles acted as a compass for navigating complexity and conflict. Implementing the principles within a culture of continuous critical reflection, learning, adaptation and reinterpretation provided focus, direction and a way of working together.36
Having collaboratively developed principles held genuine meaning for members and was important for guiding the research network.
Network analysis use and findings
The CRE-IQI conducted two network analyses over its five-year span. Firstly, cross-sectional surveys of membership were used twice to collect network data. Survey questions captured member feedback on the perceived effect of the CRE-IQI and applied network metrics to examine the functioning of the CRE-IQI over its life cycle.37 A second network analysis examined collaboration and knowledge generation through the co-authorship of peer-reviewed articles.38 Findings are detailed in the cited papers. These were the key messages:
- there was a broadening of relationships and a sharing of knowledge not only with existing partners but also new ones; more than a third of sharing occurred outside immediate collaborative partnerships, indicating good network support39
- network analysis was useful for evaluating the functioning and collaboration of an innovation platform at individual, organisational and health system levels40
- collaboration in publications increased as the network consolidated and expanded
- a need to remedy inequities in female and Indigenous authorship was identified
- diverse authorship and decentralisation of the network appeared to build research impact and advance CQI knowledge and practice
- building long-term relationships facilitated participatory research in CQI.41
Building long-term relationships facilitated participatory research in CQI.
Framework analysis use and findings
The evaluation study team used a framework analysis approach to analyse project records, reports and publications, and interviews with stakeholders. Data were mapped retrospectively against the domains of the Agency for Healthcare Research and Quality learning collaboratives taxonomy42 to understand how and why the CRE-IQI generated innovations.
Findings were detailed by J. Bailie, Peiris and colleagues.43
These were the key messages:
- The long history of working together enabled trusting relationships, a collective identity and a foundation for new people to join. Time was a crucial element.
- Innovation was stimulated by bringing people together to learn, share ideas and solve problems, with Indigenous participation and leadership at the core of the research agenda-setting.44
Impact and economic evaluation of CRE-IQI projects
In addition, a few research projects of the CRE-IQI were evaluated using the “Framework to Assess the Impact from Translational health research” tool. The tool combines quantitative and qualitative measurement techniques to assess effectiveness. It uses a scorecard approach to report research outcomes and impact across five specific domains of benefit, the social return on investment, and case studies.45
The use of different evaluation approaches identified generalisable lessons for CQI research networks:
- trusting, respectful research relationships developed over time can support productivity and a collective identity, and provide a foundation for new members
- collectively agreed operating principles help in maintaining direction and navigating complexity
- bringing people together supports learning, sharing of ideas and problem-solving
- diverse participation can be important for advancing innovation, equity and the knowledge and practice of CQI in PHC
- the continuous learning and adaptation that generally characterise CQI can be used to improve the operation of a CQI research network.
Centre for Research Excellence: Strengthening Systems for Indigenous Health Care Equity
The Centre for Research Excellence: Strengthening Systems for Indigenous Health Care Equity (CRE-STRIDE, 2020–25) built on the work and evaluation of the CRE-IQI (2015–19) by strengthening Aboriginal and Torres Strait Islander research leadership, and changing from an advisory group model to one that distributed leadership at all levels, supported by an “all teach, all learn” philosophy between Indigenous and non-Indigenous collaborators. CRE-STRIDE was committed to embedding Indigenous research leadership and methodologies throughout its structures and research programs, which were brought together in the CRE-STRIDE Framework (Figure 22.3).46
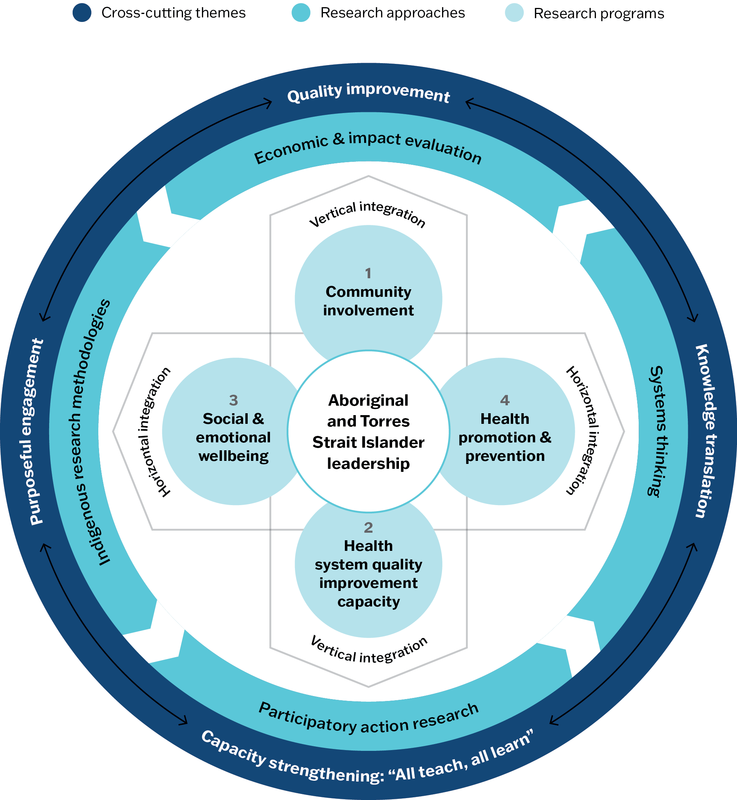
Figure 22.3 CRE-STRIDE Framework. Source: The Centre for Research Excellence: Strengthening Systems for Indigenous Health Care Equity (CRE-STRIDE n.d.a.).
The research approaches used in CRE-STRIDE were based on growing evidence of the importance of community-driven, culture-strengthening interventions in Indigenous primary healthcare settings. CRE-STRIDE’s way of working put the strengths, needs and aspirations of Aboriginal and Torres Strait Islander people at the centre of the research process, informed by methodologies that reflect Indigenous ways of knowing, being and doing.
CRE-STRIDE vision and guiding principles
CRE-STRIDE’s vision was equitable health care for Aboriginal and Torres Strait Islander peoples. Through CQI and collaborative implementation research, the network aimed to strengthen PHC and its interconnections to broader systems that affect health and wellbeing.
Specific strategies for achieving this vision were Aboriginal and Torres Strait Islander research leadership and reciprocal learning; strengthening quality improvement processes within primary healthcare systems and enhancing community engagement; and extending quality improvement processes and collaborations across sectors to promote holistic health outcomes recognising the importance of social and cultural determinants of health and wellbeing.
CRE-STRIDE’s guiding principles of practice were modified from the CRE-IQI to reflect active commitments:
- to respect – respect the past and present experiences of Aboriginal and Torres Strait Islander peoples
- to lead – Indigenous leadership or co-leadership on all projects
- to learn – “all teach, all learn” approach to collective capacity strengthening
- to relate – collaboration and partnership
- to share – sharing research and translation
- to change – work alongside community and other stakeholders to generate impactful research.47
These principles informed a way of thinking and doing that fosters culturally safe, strengths-based and transformative primary healthcare research with Aboriginal and Torres Strait Islander communities.
An Indigenous research framework for quality improvement research
CRE-STRIDE’s Indigenous Research Framework articulated these principles and provided guidance on how the collaboration could operationalise them. The framework brought together key themes from Indigenous research scholarship (as described in the previous chapter) that were important to CRE-STRIDE’s goals and work plan. Box 22.3 explains the components of CRE-STRIDE’s Indigenous Research Framework.
Box 22.3 CRE-STRIDE Indigenous Research Framework
Indigenous relationality
Our health and wellbeing encompasses Country, culture, spirituality, community and family. Land is central to our being, we understand and relate to each other by knowing where we come from and, from that, our kinship ties. Indigenous relationality, as described in Indigenous research paradigms, is around us every day. We see it in song, ceremony, throughout our daily lives. It has been intellectualised for academia, but we actually live and feel it. When we think about health and wellbeing, it is not compartmentalised into separate systems (for example, education, legal, health); rather it is a fluid and organic process that connects all elements (both human and non-human).
With this relationality comes responsibility, reciprocity and respect. We are obligated to look after Country and kin. In STRIDE, “thinking relationally” means factoring in these multiple elements into research processes and understanding that Western biomedical gold standards of research evidence alone may not necessarily provide solutions required to address health issues. To strengthen systems for healthcare equity, we must build relationships with community and work with multidisciplinary and intersectoral teams to tailor solutions to context.
Indigenous research leadership
Distributed leadership mirrors traditional forms of Aboriginal and Torres Strait Islander leadership, which is shared amongst people with differing responsibilities. Leaders are recognised based on their knowledge, reputation, personal qualities and ability to look after others (family, Country, systems of law).
Involving Aboriginal and Torres Strait Islander people in STRIDE research will empower and generate leadership at different levels. Communities provide leadership through setting research agendas and guiding methodological approaches. Aboriginal and Torres Strait Islander researchers provide leadership by sharing knowledge and understanding of Indigenous culture and contexts and facilitating relationships. Non-Indigenous researchers provide leadership by being allies, adopting new ways of thinking, critically reflecting on their own positionality and broadening their perspectives on the way knowledge can be generated and viewed. Shared leadership means working alongside each other, requiring respect, responsibility and reciprocity. STRIDE’s Indigenous research leadership is not about taking over or duplicating roles; rather it guides a changing narrative so that Indigenous methodologies, community needs, priorities and culture are at the centre of health research, designed to include and deliver benefit to Indigenous peoples.
Indigenous knowledge and sovereignty
Engaging communities in research and quality improvement processes is a foundational process in the work of STRIDE. It is also central to an Indigenous approach of locating research within community: respecting and listening to community; involving and learning from them throughout the research process; and two-way sharing of knowledge for the benefit of community health. It ensures relevance and accuracy of research; that we are working on what the community sees as priorities in a way that they understand and own.
In CRE-STRIDE, we are centring Indigenous knowledge in our research processes. As part of this, we have responsibility to ensure appropriate forms of data collection, use and reporting (Indigenous data sovereignty). This means acknowledging research data belongs to community; disrupting deficit discourses; giving data back in accessible forms (as advised by community); and strengthening the capacity of the community and their health services to act as data custodians. In this way, community is empowered to use their data for their own planning, implementation and monitoring of health and wellbeing issues and for setting research agendas (data self-determination).
“All teach, all learn” capacity strengthening
“Reciprocal learning” reflects the bringing together of different worldviews in a collaborative way, through knowledge sharing, mutual support and openness of hearts and minds to each other’s perspectives.
STRIDE’s “all teach, all learn” approach consists of mutual learning and valuing of different knowledge systems (Indigenous and non-Indigenous) and different perspectives (researcher, health service provider, community member); co-leadership, power sharing and facilitating relationships underpinned by trust and respect. Designed as a continual process of reflection and review, it requires an ability to consider self in relation to others and to engage in dialogue through constructive learning conversations. As relationality and connectedness are central to our way of life, a particular focus of STRIDE’s capacity-strengthening program is how we put inter-sectoral research into action to address social and cultural determinants of health.48
“Reciprocal learning” reflects the bringing together of different worldviews in a collaborative way, through knowledge sharing, mutual support and openness of hearts and minds to each other’s perspectives.
A matrix of strategies on how the collaboration can implement STRIDE’s principles of practice at an individual, project, collaboration and broader research system level was also developed, with the expectation that both the framework and the matrix would evolve over time. These documents formed the basis of regular reflection, evaluation and continuous improvement, with input from the broader collaboration.
Evaluating the Centre for Research Excellence: Strengthening Systems for Indigenous Health Care Equity (CRE-STRIDE)
A developmental evaluation approach was carried forward from CRE-IQI into CRE-STRIDE. The evaluation focused on newer aspects of the research network: increasing the application of Indigenous research methodologies and leadership; strengthening CQI processes within primary healthcare systems with a focus on community linkages; and extending CQI processes across sectors to promote health and wellbeing and to strengthen social and cultural determinants of health. The Ngaa-bi-nya Aboriginal and Torres Strait Islander program evaluation framework49 guided data collection and analysis in the evaluation. Ngaa-bi-nya takes a strengths-based approach, prompting evaluators to consider the historical, policy and social landscape surrounding Aboriginal and Torres Strait Islander peoples in contemporary settings.
Developmental evaluation findings (not finalised at the time of publication) indicate that the CRE-STRIDE network achieved its goals, despite the early challenges and ongoing effects of the Covid-19 pandemic and weather-related disasters that affected the host organisation and many network members.
- Indigenous leadership became strongly embedded across the network, with Indigenous people represented at all levels.
- The Indigenous Research Framework was accepted and used across many of the STRIDE projects; some members sought guidance for applying the framework in their research. Relationality was highly valued. A focus on Indigenous knowledge and sovereignty strengthened community participation and self-determination in research, broadened members’ thinking around data and inclusivity, and expanded the evidence base for Indigenous methodologies in CQI research.
- By integrating Indigenous leadership, knowledges and methodologies throughout the CRE-STRIDE, members were able to enhance community linkages and push the boundaries of CQI to incorporate social, cultural and environmental determinants of health.
- The foundational work of previous iterations of the research network allowed CRE-STRIDE to diversify its research focus and take a more holistic approach to PHC and equity for Indigenous communities. Areas of CQI research included clinical care, social determinants of health, social and emotional wellbeing, environmental and climate change effects.50
The next phase of the Indigenous-led CQI research network is STAUNCH – Stronger Together As Unified Nations for Community-led Health. STAUNCH aims to promote sovereign health and wellbeing by centring Indigenous Nation Building to assert local policy and program solutions for improving the quality of comprehensive primary health care. Research activities focus on strengthening First Nations’ self-governance, defining new quality and safety standards for care models that include the determinants of health, and guiding policymakers to look at health and wellbeing solutions that holistically consider social, political, economic and environmental issues.
Indigenous data sovereignty
CRE-STRIDE’s Indigenous Research Framework (Box 22.3) outlines actions the network took to advance Indigenous data sovereignty, a global movement concerned with the right of Indigenous peoples to govern the creation, collection, ownership and use of data about Indigenous peoples, lands and cultures.51 In support of these rights, the Global Indigenous Data Alliance has developed the CARE principles for Indigenous data governance, which are framed around collective benefit, authority to control, responsibility and ethics.52 Case studies, ecosystems and resources for advancing data sovereignty are becoming increasingly available.53 Indigenous data sovereignty holds messages for CQI research.
The Indigenous data sovereignty movement challenges how governments and institutions have historically captured and used data representing Indigenous peoples to develop policies and programs that do not protect and respect Indigenous interests or worldviews. It also draws attention to the way aggregated and decontextualised data can present people as problematic54 because they are unable to meaningfully reflect lived experiences, histories and cultural realities. These concerns reflect wider social and global movements calling for a shift from descriptive, problem-focused research about historically disempowered or socially excluded groups, to more action-oriented and solution-focused research that facilitates social inclusion, self-determination and health equity.55
The aggregation of data is, at times, necessary for population health approaches such as CQI and epidemic or pandemic management. Aggregated data provide information about the issues communities and populations are dealing with, enable changes in population health to be measured, improvement strategies to be designed and resources to be allocated. When using aggregated population health data to plan policies and improvement interventions, these aspects need to be considered:
- whether the data incorporates and reflects the strengths, values, knowledge systems and practices of the people to whom the policies relate, appropriately as determined by those groups56
- how to ensure communities have control over the distribution of resources based on local priorities, existing resources, knowledge, and governance processes57
- how data management systems can be used as a resource to serve communities.58
Summary
This chapter has described how a CQI and health systems research network in Aboriginal and Torres Strait Islander PHC has actioned key principles and built on learning to transform a CQI research program in Australia. The journey began with a participatory action research project testing the feasibility of CQI in 12 primary healthcare services59 and evolved into a collaboration involving diverse partners committed to primary healthcare quality improvement. We have shared lessons learnt through two decades of CQI research and evaluation, describing mechanisms and features developed to support innovation and to foster Indigenous-led, strengths-based quality improvement research with Aboriginal and Torres Strait Islander communities.
Equitable, collaborative research relationships have positive relational features that include trust, respect for knowledge and each other, a sense of belonging, and open lines of communication. Positive structural features are also necessary to improve equity in research, including opportunities for capacity building, inclusive decision-making, recognition of contribution (for example, through authorship and distributed leadership), and governance structures that empower participating organisations and communities.60 These features are important for progressing the network’s ongoing research agenda and meeting future research challenges. The capacity to respond and adapt to changing contexts is essential for an equity-focused quality improvement research network and for the effective implementation of CQI.
References
Bailie, J., F. Cunningham, S. Abimbola, A. Laycock, R. Bainbridge, R. Bailie et al. (2022). Methodological pluralism for better evaluations of complex interventions: lessons from evaluating an innovation platform in Australia. Health Research Policy and Systems 20(1): 14. DOI: 10.1186/s12961-022-00814-5.
Bailie, J., F. Cunningham, R. Bainbridge, M. Passey, A. Laycock, R. Bailie et al. (2018). Comparing and contrasting “innovation platforms” with other forms of professional networks for strengthening primary healthcare systems for Indigenous Australians. BMJ Global Health 3: e000683. DOI: 10.1136/bmjgh-2017-000683.
Bailie, J., A. Laycock, K. Conte, V. Matthews, D. Peiris, R. Bailie et al. (2021). Principles guiding ethical research in a collaboration to strengthen Indigenous primary healthcare in Australia: learning from experience. BMJ Global Health 6(1): e003852. DOI: 10.1136/bmjgh-2020-003852.
Bailie, J., A. Laycock, V. Matthews and R. Bailie (2016) System-level action required for wide-scale improvement in quality of primary health care: synthesis of feedback from an interactive process to promote dissemination and use of aggregated quality of care data. Frontiers in Public Health
4: 86. DOI: 10.3389/fpubh.2016.00086.
Bailie, J., A. Laycock, D. Peiris, R. Bainbridge, V. Matthews, F. Cunningham et al. (2020). Using developmental evaluation to enhance continuous reflection, learning and adaptation of an innovation platform in Australian Indigenous primary healthcare. Health Research Policy and Systems
18(1): 45. DOI: 10.1186/s12961-020-00562-4.
Bailie, J., D. Peiris, F. Cunningham, A. Laycock, R. Bailie, V. Matthews et al. (2021). Utility of the AHRQ learning collaboratives taxonomy for analyzing innovations from an Australian collaborative. Joint Commission Journal on Quality and Patient Safety 47: 711–22. DOI: 10.1016/j.jcjq.2021.08.008.
Bailie, J., B. Potts, A. Laycock, S. Abimbola, R. Bailie, F. Cunningham et al. (2021). Collaboration and knowledge generation in an 18-year quality improvement research programme in Australian Indigenous primary healthcare: a coauthorship network analysis. BMJ Open 11(5): e045101. DOI: 10.1136/bmjopen-2020-045101.
Bailie, R., J. Bailie, S. Larkins and E. Broughton (2017). Editorial: Continuous quality improvement (CQI)—advancing understanding of design, application, impact, and evaluation of CQI approaches. Frontiers in Public Health 5: 306. DOI: 10.3389/fpubh.2017.00306.
Bailie, R., D. Si, L. O’Donoghue and M. Dowden (2007). Indigenous health: effective and sustainable health services through continuous quality improvement. Medical Journal of Australia 186(10): 525–7. DOI: 10.5694/j.1326-5377.2007.tb01028.x.
Benveniste, T., A. Laycock, R. Bailie, J. Bailie, K. Vine, K. Clancy et al. (2023). Finding our “STRIDE”: draft developmental evaluation interim report, vol. 1. Centre for Research Excellence: Strengthening Systems for Indigenous Health Equity. Lismore, NSW: University Centre for Rural Health, University of Sydney.
Blanchet, K. and P. James (2012). How to do (or not to do) . . . a social network analysis in health systems research. Health Policy and Planning 27(5): 438–46. DOI: 10.1093/heapol/czr055.
Bond, C. (2009). Starting at strengths . . . an Indigenous early years intervention. Medical Journal of Australia 191(3): 175–7. DOI: 10.5694/j.1326-5377.2009.tb02733.x.
Bond, C., W. Foley and D. Askew (2016). “It puts a human face on the researched” – a qualitative evaluation of an Indigenous health research governance model. Australian and New Zealand Journal of Public Health 40(S1): S89–S95. DOI: 10.1111/1753-6405.12422.
Brimblecombe, J., C. van den Boogaard, B. Wood, S. Liberato, J. Brown, A. Barnes et al. (2015). Development of the good food planning tool: a food system approach to food security in indigenous Australian remote communities. Health Place 34: 54–62. DOI: 10.1016/j.healthplace.2015.03.006.
Centre for Research Excellence: Strengthening Systems for Indigenous Health Care Equity (CRE-STRIDE) (n.d.a.). Background. https://cre-stride.org/background/.
Centre for Research Excellence: Strengthening Systems for Indigenous Health Care Equity (CRE-STRIDE) (n.d.b.). Guiding principles. https://cre-stride.org/guiding-principles/.
Clapham, K. (2011). Indigenous-led intervention research: the benefits, challenges and opportunities. International Journal of Critical Indigenous Studies. 4(2): 40–8. DOI: 10.5204/ijcis.v4i2.63
Coalition of Aboriginal and Torres Strait Islander Peak Organisations and Australian Governments (2020). National Agreement on Closing the Gap. Department of the Prime Minister and Cabinet. Canberra: Commonwealth of Australia.
Cunningham, F., S. Ferguson-Hill, V. Matthews and R. Bailie (2016). Leveraging quality improvement through use of the Systems Assessment Tool in Indigenous primary health care services: a mixed methods study. BMC Health Services Research 16(1): 583. DOI: 10.1186/s12913-016-1810-y.
Cunningham, F., B. Potts, S. Ramanathan, J. Bailie, R. Bainbridge, A. Searles et al. (2022). Network evaluation of an innovation platform in continuous quality improvement in Australian Indigenous primary healthcare. Health Research Policy and Systems 20(1): 119. DOI: 10.1186/s12961-022-00909-z.
Elston, J., V. Saunders, B. Hayes, R. Bainbridge and B. McCoy (2013). Building Indigenous Australian research capacity. Contemporary Nurse: A Journal for the Australian Nursing Profession 46(1): 6–12. DOI: 10.5172/conu.2013.46.1.6.
Evans, M., A. Miller, P. Hutchinson and C. Dingwall (2014). Decolonizing research practice: indigenous methodologies, Aboriginal methods, and knowledge/knowing. In P. Leavy, ed. The Oxford Handbook of Qualitative Research, 179–91. Oxford: Oxford University Press.
Faure, M., N. Munung, N. Ntusi, B. Pratt and J. de Vries (2021). Considering equity in global health collaborations: a qualitative study on experiences of equity. PLOS One 16(10). DOI: 10.1371/journal.pone.0258286.
Gibson-Helm, M., A. Rumbold, H. Teede, S. Ranasinha, R. Bailie and J. Boyle (2016). Improving the provision of pregnancy care for Aboriginal and Torres Strait Islander women: a continuous quality improvement initiative. BMC Pregnancy and Childbirth 16: 118. DOI: 10.1186/s12884-016-0892-1.
Global Indigenous Data Alliance (n.d.). CARE Principles for Indigenous Data Governance. https://www.gida-global.org/care.
Indigenous Reference Committee CRE-STRIDE (2020). Indigenous Research Framework. Lismore, NSW: Centre for Research Excellence: Strengthening Systems for Indigenous Health Care Equity.
Iyamu, I., M. Berger, S. Fernando, M. Snow and A. Salmon (2022). Developmental evaluation during the COVID-19 pandemic: practice-based learnings from projects in British Columbia, Canada. Evaluation Journal of Australasia: 1035719. DOI: 10.1177/1035719X221119841.
Kukutai, T. and J. Taylor, eds (2016). Indigenous data sovereignty: toward an agenda. Canberra: ANU Press.
Laycock, A., J. Bailie, V. Matthews and R. Bailie (2019). Using developmental evaluation to support knowledge translation: reflections from a large-scale quality improvement project in Indigenous primary healthcare. Health Research Policy and Systems 17(1): 70. DOI: 10.1186/s12961-019-0474-6.
Laycock, A., K. Conte, K. Harkin, J. Bailie, V. Matthews, F. Cunningham et al. (2020). Improving the quality of primary health care for Aboriginal and Torres Strait Islander Australians 2015–2019: Messages for Action, Impact and Research. Centre for Research Excellence in Integrated Quality Improvement Lismore NSW: University Centre for Rural Health, University of Sydney.
Laycock, A., D. Walker, N. Harrison and J. Brands (2011). Researching Indigenous health: a practical guide for researchers. Melbourne: Lowitja Institute.
Lovett, R. (2016). Aboriginal and Torres Strait Islander community wellbeing: identified needs for statistical capacity. In T. Kukutai and J. Taylor, eds. Indigenous data sovereignty: toward an agenda, 213–31. Canberra: ANU Press.
Maiam nayri Wingara Indigenous Data Sovereignty Collective (2019). Indigenous data sovereignty principles. https://mkstudy.com.au/indigenousdatasovereigntyprinciples/.
McPhail-Bell, K., V. Matthews, R. Bainbridge, M. Redman-MacLaren, D. Askew, S. Ramanathan et al. (2018). An “all teach, all learn” approach to research capacity strengthening in Indigenous primary health care continuous quality improvement. Frontiers in Public Health 6: 107. DOI: 10.3389/fpubh.2018.00107.
Mery, G., M. Dobrow, G. Baker, J. Im and A. Brown (2017). Evaluating investment in quality improvement capacity building: a systematic review. BMJ Open 7(2): e012431–e31. DOI: 10.1136/bmjopen-2016-012431.
National Health and Medical Research Council (2018a). Ethical conduct in research with Aboriginal and Torres Strait Islander peoples and communities: guidelines for researchers and stakeholders. Canberra: Commonwealth of Australia.
National Health and Medical Research Council (2018b). Keeping research on track II: a companion document to Ethical conduct in research with Aboriginal and Torres Strait Islander peoples and communities: guidelines for researchers and stakeholders. Canberra: Commonwealth of Australia. https://www.nhmrc.gov.au/about-us/resources/keeping-research-track-ii.
Nicholls, R. (2009). Research and Indigenous participation: critical reflexive methods. International Journal of Social Research Methodology 12(2): 117–26. DOI: 10.1080/ 13645570902727698.
Nix, M., P. McNamara, J. Genevro, N. Vargas, K. Mistry, A. Fournier et al. (2018). Learning collaboratives: insights and a new taxonomy from AHRQ’s two decades of experience. Health Affairs (Millwood) 37(2): 205–12. DOI: 10.1377/hlthaff.2017.1144.
Otoo, S., N. Agapitova and B. Joy (2009). The Capacity Development Results Framework: a strategic and results-oriented approach to learning for capacity development. Washington, DC: World Bank.
Patton, M. (2018). Principles-focused evaluation – the guide. New York, NY: Guilford Press.
Patton, M. (2016). What is essential in developmental evaluation? On integrity, fidelity, adultery, abstinence, impotence, long-term commitment, integrity, and sensitivity in implementing evaluation models. American Journal of Evaluation 37(2): 250–65. DOI: 10.1177/1098214015626295.
Patton, M. (2011). Developmental evaluation: applying complexity concepts to enhance innovation and use. New York, NY: The Guilford Press.
Phelan, A. (2020). “We need to be seen” – why data is vital in the fight against Covid-19. University of New South Wales, 25 March. https://newsroom.unsw.edu.au/news/health/we-need-be-seen-%E2%80%93-why-data-vital-fight-against-covid-19.
Ramanathan, S., S. Larkins, K. Carlisle, N. Turner, R. Bailie, S. Thompson et al. (2021). What was the impact of a participatory research project in Australian Indigenous primary healthcare services? Applying a comprehensive framework for assessing translational health research to Lessons for the Best. BMJ Open 11(2): e040749. DOI: 10.1136/bmjopen-2020-040749.
Redman-MacLaren, M., D. MacLaren, H. Harrington, R. Asugeni, R. Timothy-Harrington, E. Kekeubata et al. (2012). Mutual research capacity strengthening: a qualitative study of two-way partnerships in public health research. International Journal for Equity in Health 11(1): 79. DOI: 10.1186/1475-9276-11-79.
Searles, A., C. Doran, J. Attia, D. Knight, J. Wiggers, S. Deeming et al. (2016). An approach to measuring and encouraging research translation and research impact. Health Research Policy and Systems 14(1). DOI: 10.1186/s12961-016-0131-2.
Si, D., R. Bailie, C. Connors, M. Dowden, A. Stewart, G. Robinson et al. (2005). Assessing health centre systems for guiding improvement in diabetes care. BMC Health Services Research 5: 56. DOI: 10.1186/1472-6963-5-56.
Smylie, J., A. Lofters, M. Firestone and P. O’Campo (2012). Population-based data and community empowerment. In Patricia O’Campo and James R. Dunn, eds. Rethinking social epidemiology: towards a science of change, 67–92. Dordrecht, the Netherlands: Springer.
Standen, J., G. Morgan, T. Sowerbutts, K. Blazek, J. Gugusheff, O. Puntsag et al. (2020). Prioritising housing maintenance to improve health in Indigenous communities in NSW over 20 years. International Journal of Environmental Research and Public Health 17(16). DOI: 10.3390/ijerph17165946.
Sustainable Improvement Team and the Horizons Team (2018). Leading large scale change: a practical guide. England: National Health Service.
Tsey, K., K. Lawson, I. Kinchin, R. Bainbridge, J. McCalman, F. Watkin et al. (2016). Evaluating research impact: the development of a research for impact tool. Frontiers in Public Health 4: 160. DOI: 10.3389/fpubh.2016.00160.
Tuhiwai Smith, L. (1999). Decolonizing methodologies: research and indigenous peoples. London: Zed Books.
United Nations (2007). United Nations Declaration on the Rights of Indigenous Peoples. https://www.ohchr.org/en/indigenous-peoples/un-declaration-rights-indigenous-peoples.
Walter, M. (2016). Data politics and Indigenous representation in Australian statistics. In T. Kukutai and J. Taylor, eds. Indigenous data sovereignty: toward an agenda, 79–98. Canberra: ANU Press.
Walter, M., T. Kukutai, S. Russo Carroll and D. Rodriguez-Lonebear, eds (2021). Indigenous data sovereignty and policy. London: Routledge.
Williams, M. (2018). Ngaa-bi-nya Aboriginal and Torres Strait Islander program evaluation framework. Evaluation Journal of Australasia 18(1): 6–20. DOI: 10.1177/1035719X18760141.
1 Coalition of Aboriginal and Torres Strait Islander Peak Organisations and Australian Governments 2020.
2 R. Bailie, Si et al. 2007; Si, R. Bailie et al. 2005.
3 R. Bailie, J. Bailie et al. 2017.
4 J. Bailie, Laycock et al. 2016; Gibson-Helm, Rumbold et al. 2016.
5 Cunningham, Ferguson-Hill et al. 2016.
6 Brimblecombe, van den Boogaard et al. 2015; CRE-STRIDE n.d.a.; Standen, Morgan et al. 2020.
7 J. Bailie, Cunningham et al. 2018.
8 Sustainable Improvement Team and the Horizons Team 2018.
9 J. Bailie, Cunningham et al. 2018.
10 McPhail-Bell, Matthews et al. 2018.
11 Otoo, Agapitova and Joy 2009.
12 Mery, Dobrow et al. 2017.
13 McPhail-Bell, Matthews et al. 2018.
14 McPhail-Bell, Matthews et al. 2018.
15 Redman-MacLaren, MacLaren et al. 2012; Elston, Saunders et al. 2013.
16 Bond 2009; Evans, Miller et al. 2014; Laycock, Walker et al. 2011; McPhail-Bell, Matthews et al. 2018; Nicholls 2009.
17 Clapham 2011.
18 Tsey, Lawson et al. 2016.
19 Bond, Foley and Askew 2016; Elston, Saunders et al. 2013; McPhail-Bell, Matthews et al. 2018; Tuhiwai Smith 1999.
20 McPhail-Bell, Matthews et al. 2018.
21 National Health and Medical Research Council 2018a, b.
22 J. Bailie, Cunningham et al. 2022.
23 Patton 2011, 2016.
24 Patton 2018, 3.
25 Blanchet and James 2012.
26 Nix, McNamara et al. 2018.
27 J. Bailie, Cunningham et al. 2022.
28 Ramanathan, Larkins et al. 2021.
29 Laycock, J. Bailie et al. 2019.
30 J. Bailie, Laycock et al. 2020.
31 Iyamu, Berger et al. 2022.
32 J. Bailie, Laycock et al. 2021.
33 J. Bailie, Laycock et al. 2021, 5.
34 J. Bailie, Laycock et al. 2021, 8.
35 J. Bailie, Laycock et al. 2021.
36 J. Bailie, Laycock et al. 2021.
37 Cunningham, Potts et al. 2022.
38 J. Bailie, Potts et al. 2021.
39 J. Bailie, Cunningham et al. 2022; Cunningham, Potts et al. 2022.
40 Cunningham, Potts et al. 2022.
41 J. Bailie, Potts et al. 2021.
42 Nix, McNamara et al. 2018.
43 J. Bailie, Peiris et al. 2021.
44 J. Bailie, Peiris et al. 2021.
45 Ramanathan, Larkins et al. 2021; Searles, Doran et al. 2016.
46 The Centre for Research Excellence: Strengthening Systems for Indigenous Health Care Equity (CRE-STRIDE) n.d.a.
47 The Centre for Research Excellence: Strengthening Systems for Indigenous Health Care Equity (CRE-STRIDE) n.d.b.
48 Indigenous Reference Committee (CRE-STRIDE) 2020.
49 Williams 2018.
50 Benveniste, Laycock et al. 2023.
51 Maiam nayri Wingara Indigenous Data Sovereignty Collective 2019; United Nations 2007, Article 13.
52 Global Indigenous Data Alliance n.d.
53 Kukutai and Taylor 2016; Walter, Kukutai et al. 2021.
54 Walter 2016.
55 Smylie, Lofters et al. 2012.
56 Smylie, Lofters et al. 2012.
57 Lovett 2016.
58 Kalinda Griffiths in Phelan 2020.
59 Smylie, Lofters et al. 2012.
60 R. Bailie, Si et al. 2007.
61 Faure, Munung et al. 2021; Indigenous Reference Committee (CRE-STRIDE) 2020.