20
Multi-level systems approaches
Throughout this book we have advocated the use of systems thinking in CQI: analysing how parts of a healthcare system work together to support PHC, and how parts of a system can be changed to produce better outcomes.1 Systems thinking helps in understanding how care systems interact to influence quality of care for clients. Systems thinking also encourages teams to consider the wider contexts in which PHC services operate: the resources available and the historical, social, economic and environmental circumstances that influence people’s health and wellbeing across the life course.2 Examples are the positive health effects of a secure food supply and employment opportunities, or the negative effects of discrimination on health and wellbeing. While these types of determinants of health may not be within the sphere of control of a PHC service or practice, they will be of concern, and the intersectoral action required to improve outcomes can be influenced and facilitated by PHC services.3
The intersectoral action required to improve outcomes can be influenced or facilitated by PHC services.
Healthcare equity has been advanced when system-strengthening efforts take account of various determinants of health (for example, social, economic, cultural, structural, political, environmental), and when these efforts are applied on a wide scale and at different levels of the system. In systems thinking, everyone’s actions count, and – while it requires societal and political commitment and collective effort to create change – the quality improvement efforts of PHC professionals and communities make important contributions. These contributions are strengthened when CQI efforts are sustained through policy and funding commitment at a higher system level. This chapter uses real-world examples to illustrate how multi-level and intersectoral systems approaches to CQI can be used to improve the quality of comprehensive PHC, as part of a broader systems approach to improving health and wellbeing.
A systems framework for CQI in PHC services
In Chapter 3, we introduced a systems framework that illustrates the potential for PHC services to support and extend CQI efforts in two dimensions: vertically across the health system and horizontally across sectors (Figure 3.1). The framework demonstrates these features:
- vertical integration, referring to the use of CQI across all levels of health systems from community engagement and client care (base of diagram) to jurisdiction/provincial and national levels (top of diagram)
- horizontal integration, referring to the incorporation of CQI into evidence-based clinical care (left of diagram) and linkages and advocacy for influencing the social and cultural determinants of health (right of diagram)
- within PHC services, the conditions that support an integrated systems approach to improvement are trained and supported staff, engaged and active service users, strong management systems and a culture of CQI, resourcing and cost-effectiveness.4
While the contexts in which PHC operates vary widely, the health of populations is always influenced by a range of determinants, which are in turn influenced by many factors including collective action. And while quality improvement strategies and tools differ, CQI is inherently participatory and requires partnering with other agencies and groups (or teams) to monitor and mobilise action on social, cultural, economic, political and environmental determinants.
The framework in action
In the following examples, people working in different sectors or at different levels of the health system came together in a systems approach to quality improvement. The supportive conditions identified in the framework can be identified to varying degrees within these examples.
Example: community engagement improves ear health
After a review of child ear health data, the child health team at Yadu Health Aboriginal Corporation identified the need to increase screening (otoscopy and tympanometry) rates to enable early identification and management of middle ear disease. The team worked with staff at local schools and childcare centres to set up outreach clinics and trained several colleagues in screening techniques. During consultations, a video otoscope was used to spark conversations about healthy ears with children and their parents or carers. Letters advising families of screening results and next steps were followed up with phone calls and home visits as needed, and the child health team worked with other PHC practitioners to provide children with ongoing ear care. A new referral process was put in place to increase families’ access to visiting specialist services at the regional hospital. Senior managers also negotiated for an ear specialist to deliver care at the PHC service twice a year, reducing the need for families to undertake the 1,600-kilometre return journey to the capital city for treatment.
Early outcomes included increased staff skills and confidence in ear health care, significant increases in ear health screening, multiple pathways for families to access ear health services, greater community interest in ear health and care, and stronger health service/community connections.5
Example: partnerships improve cancer care
A quality improvement initiative is supporting Aboriginal community controlled PHC services in Dharawal Country in New South Wales to deliver evidence-based holistic cancer prevention, support and care. Illawarra Aboriginal Medical Service partnered with health support organisations at the national and state level and with university researchers to evaluate the cancer care training needs of staff and to document case studies of best-practice cancer care reflecting Aboriginal practices and values. The information from this initiative was used to develop a manual and training materials to help teams to continually improve and monitor the quality of cancer prevention programs and cancer care, as well as palliative care, advanced care planning and grief support for families and carers.6
Example: access to data enhances improvement
In some large organisations, key performance indicator reports or data dashboards are prepared centrally and sent to health services to support their CQI programs. PHC teams can see the areas of care where they are doing well and not so well, data trends over time, and how their health centre’s indicators are benchmarked against regional averages. CQI facilitators generally aim to involve as many staff as possible in reviewing reports and interpreting data, including those who live in the local community. An inclusive approach brings contextual knowledge and a range of perspectives to data interpretation, goal setting and improvement planning.7
Example: clients’ priorities improve healthy ageing supports
Communities and PHC services in the Torres Strait are working with researchers to develop a framework to facilitate healthy ageing. Elderly residents join yarning circles to talk about what it means to them to age well and what their priorities are as they age. CQI methods are then used to audit existing community and health services to identify gaps in holistic care for older people and act on the priorities. Outcomes from the community engagement process include a quality framework of best-practice screening and assessment with a toolbox of resources to support healthy ageing. The resources are designed to be implemented in local communities and PHC services.8
Example: partnerships to combat environmental determinants of health
In parts of northern Australia, the convergence of excessive heat, poor housing, energy insecurity and chronic disease has reached critical levels. Uninsulated, poorly ventilated houses are becoming dangerously hot as climate change increases temperatures, and poor energy efficiency means that more electricity is needed to keep homes thermally safe. This increases financial stress on already disadvantaged communities; most households are disconnected from the electricity supply more than ten times a year. Extreme heat causes significant health problems and makes existing conditions worse, and, when the power goes off, people cannot safely store medications or use vital health equipment, such as machines to help them breathe or home dialysis equipment.
A multi-sectoral response is needed. Indigenous community leaders are involving health professionals, architects, engineers, researchers and others in advocating for climate-resilient, energy-efficient public housing that is co-designed with communities or retrofitted to reflect their cultural practices and accumulated knowledge of how to live in hot climates. Healthcare leaders are raising clinicians’ awareness of the need to be cognisant of the direct effects of heat on their clients’ health and health risks, care management and capacity for self-care, and are joining calls for legislative protections for safe housing and energy security in remote communities.9
The CQI tools described in Box 20.1 were developed to support a systems approach to improving social and environmental determinants of health in rural and remote Australian communities. They were created and piloted through multi-phase and iterative processes that involved a series of consultations with community members and relevant stakeholders. The tools can be used in conjunction with clinical audit tools to promote a holistic, systems-thinking approach to CQI.
A similar approach was used to develop the Good Food Systems Tool described in Chapter 5, which supports community-driven decision-making to tackle inequities in food supply and food access for remote Indigenous communities.10
Box 20.1 A cross-sector initiative to develop CQI tools
Some of the common factors underlying poor child health are crowded housing, and inadequate access to health hardware, health resources and services. A CQI initiative aimed to identify the factors underlying high rates of poor child health in remote Aboriginal communities and develop indicators and CQI tools. The project brought together people from different knowledge systems, backgrounds and disciplines, allowing for diverse perspectives to be reflected in the physical and social factors identified and in the two tools developed.
- The Healthy Community Assessment Tool11 assessed whether communities had the infrastructure and programs that enabled community members to make healthy lifestyle choices. Indicators such as water supply, food supply, waste disposal, sport and recreational facilities, early childhood education and childcare services were included.
- The Household Assessment Tool12 was initiated by a health service manager for use in an early intervention program aiming to prevent progression from growth faltering to failure to thrive among infants. Social and environmental indicators placing children at greater risk of poor health and development outcomes were included (for example, housing functionality, hygiene and child safety, crowding, food security, social environment, school attendance). Household-level indicators aimed to match the objectives and performance indicators in service agreements between government and community agencies.
Linking PHC staff and community members with people beyond the health sector had several benefits.
- Different perspectives were incorporated in addition to evidence-based indicators already in the public domain: scientific (for example, biological plausibility), lay perceptions and Aboriginal perspectives.
- The indicators were seen as meaningful and appropriate by community residents (and other key stakeholders).
- The tools were co-designed with community members and can be used by health practitioners, health promotion officers, community leaders, environmental health and housing officers, and other government officers.13
A multi-level, system-wide approach to improvement
CQI is particularly effective in improving the standard of care when applied system-wide.14 When Ferlie and Shortell examined quality strategies in the United States and the United Kingdom more than two decades ago, they found that efforts relying on narrow, single-level program changes were largely unsuccessful. The health systems researchers argued that system changes are needed concurrently at four levels to achieve and sustain quality improvement:
- individual level (for example, education, leadership development at all levels, guideline use)
- group or team level (for example, clinical audits, team development, guideline use)
- organisation level (for example, CQI, organisational learning, organisational culture)
- larger system or policy environment in which an organisation operates (for example, national improvement policies, accrediting agencies, legal systems, funding policies).15
It is now widely accepted that “for CQI to add value, have impact and realise its potential, it [needs] to be managed at multiple levels”.16 In Australia, for example, efforts to tackle entrenched health inequality for Aboriginal and Torres Strait Islander peoples have featured multi-level investment in CQI. While there are different CQI program approaches across jurisdictions, and different levels of maturity in the use of CQI across services, national level policy and funding agreements require that PHC services use CQI processes to monitor improvement efforts and enhance the quality of service delivery.17 This high-level policy and funding approach helps to sustain CQI processes at the PHC service and practice level. A comparative case study published in 2017 found that consistent and sustained policy and multi-level infrastructure support for CQI in the Northern Territory (as outlined in the following example) enabled wide-scale and ongoing improvement in quality of care, compared with jurisdictions where CQI efforts were generally smaller in scale and more fragmented.18 The authors concluded that it was not sufficient for improvement initiatives to rely on local service managers and clinicians, as their efforts are strongly mediated by higher system-level influences.
Example: sustained commitment to CQI at multiple levels
Larger system level
A five-year National Framework for Continuous Quality Improvement in Primary Health Care for Aboriginal and Torres Strait Islander People 2018–2319 was developed in Australia as a joint initiative of the National Aboriginal Community Controlled Health Organisation and affiliates, with support from the Commonwealth Department of Health. The framework is complemented by a Model of Aboriginal and Torres Strait Islander Community-Controlled Comprehensive Primary Health Care,20 which specifies the use of CQI in each of the four domains of core services: governance; community health promotion and empowerment; clinical services; policy direction and partnerships.
Organisation level
In the Northern Territory, a CQI strategy21 is governed by a steering committee representing key stakeholders. Community-controlled and government-managed health services participate in the strategy, which aims to ensure CQI is part of core business for every PHC service. There has been sustained investment in building CQI knowledge and skills and providing health services with tools and strategies for engaging in CQI. Processes to support the use of data for CQI were established through a data working group and collaboratives.
Group or team level
Two coordinators provide program management and leadership, CQI expertise and support to facilitators employed by health services, who provide practical support in planning and implementing CQI. All PHC teams have access to CQI training, a range of data sources and opportunities to participate in CQI processes.
Individual level
Feedback about quality of care to PHC staff, members of governing boards, clients and communities is tailored to identified needs. Managers and members of multidisciplinary PHC teams have access to CQI and cultural safety training, CQI collaboratives and other professional development. There is high workforce turnover, particularly in remote communities, however a core of CQI leaders and community champions endures.22
For CQI to add value, have effect and realise its potential, it needs to be managed at multiple levels.
Using CQI data for wide-scale improvement
Despite developments in CQI theory and practice, there is little evidence about how to engage stakeholders in wide-scale CQI processes to inform system strengthening. Yet bringing together CQI data from multiple PHC centres has scope to engage stakeholders in identifying common priorities for improving care, and interventions that target change at different health-system levels. To this end, our CQI research network conducted an interactive data dissemination process targeting people in diverse PHC roles at different levels of the health system. The CQI data had been collected over 10 years and represented more than 60,000 de-identified clinical audits of client records and 492 systems assessments from 175 PHC centres across five Australian jurisdictions.23
- Aggregated CQI data reports were distributed by email through the existing ABCD National Research Partnership network (described in Chapter 9) and a snowballing recruitment technique was used to invite wider participation.
- Stakeholders were invited to use aggregated CQI data reports to identify the evidence-to-practice gaps, barriers and enablers most critical to improving health outcomes in key areas of clinical care, and to suggesst improvement strategies.
- Feedback was obtained through online surveys. A phased reporting and feedback process was used, culminating in a final report and other outputs (for example, journal articles, summaries) (see Figure 20.1).
- The process was used to generate findings for child health, maternal health, preventive care, chronic illness, mental health, and acute rheumatic fever and rheumatic heart disease care. (Key findings are reported in Part III.24)
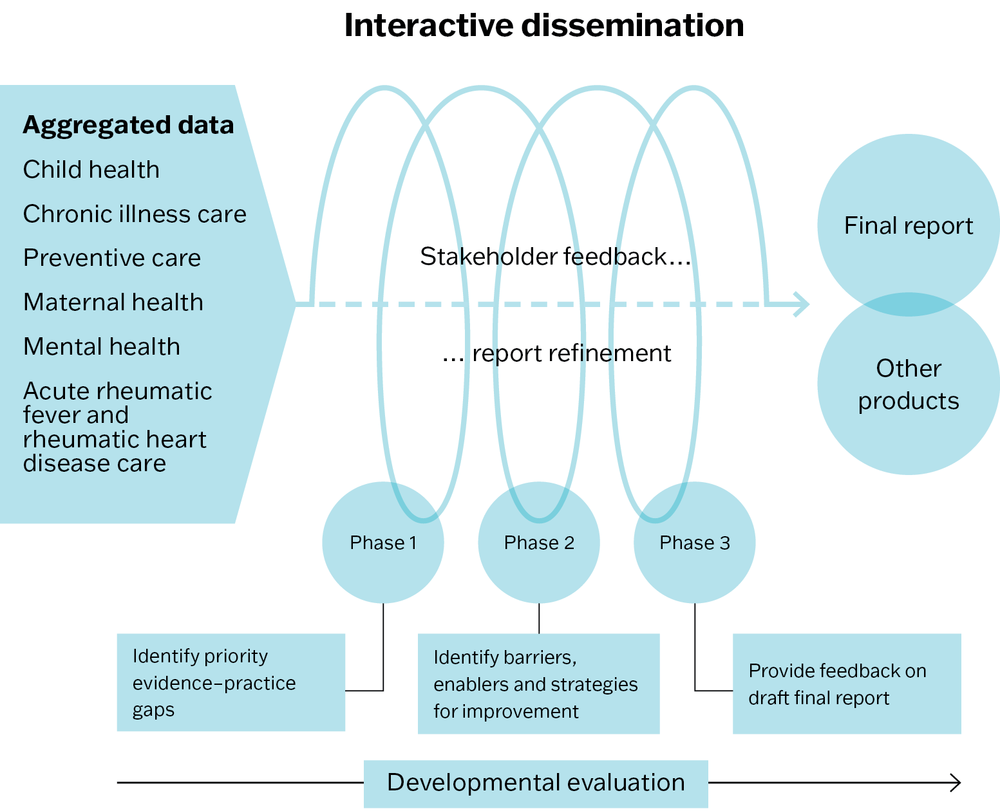
Figure 20.1 Engaging stakeholders in identifying priority evidence–practice gaps, barriers and strategies for improvement (ESP) project. Source: Laycock, Harvey
et al. 2018.
People who responded to the project surveys included Aboriginal and Torres Strait Islander health practitioners, nurses, doctors and other health practitioners, CQI facilitators, policymakers, PHC managers, governing board members and researchers.25
The commonly identified evidence-to-practice gaps across all the data could be grouped into five categories:
- follow-up of abnormal findings
- assessment and counselling for lifestyle risk factors
- emotional wellbeing screening and support
- treatment adherence (for example, taking medications) and self-management
- physical checks and investigations.
Synthesising the findings to identify messages for greater impact
When the priority evidence-to-practice gaps in each area of PHC (for example, child health, chronic illness care) were mapped according to these five categories, three improvement needs were common to all areas:
- follow-up of abnormal findings
- risk factor inquiry and provision of brief interventions
- social and emotional wellbeing support.
This finding suggested that improving these care processes would improve the quality of care for clients with a range of health conditions and care needs. Survey data about system barriers to improving the three gaps were analysed; these data reflected participants’ contextual and professional knowledge and their experience working in Aboriginal and Torres Strait Islander PHC. Pareto analysis was used to identify the “vital few” system barriers to improvement in each of the categories. (For an explanation of Pareto analysis, see Chapter 5). The findings are summarised in Figure 20.2.
As illustrated in Figure 20.2, the “vital few” barriers to improvement were identified as clinical information systems, workforce, staff skills and training, financial resources and community engagement. The findings suggested that focusing improvement efforts on these aspects of PHC would increase the effect for improving people’s health.
The analysis also reinforced the importance of multi-level action across the health system to improve PHC performance, and the need to bring communities, policymakers and practitioners together to plan system improvement. As project participants reflected:
“At the micro level [the process] can start conversations … on a macro level, it provides this large scale, very hard to argue with evidence for why action is needed, and support from the wider health system, government and funders.” – researcher
“I see the role of data as bringing strategic people closer to the frontline practitioners, and then saying, ‘We need to do something about this, help us and we will help you’.” – senior manager26
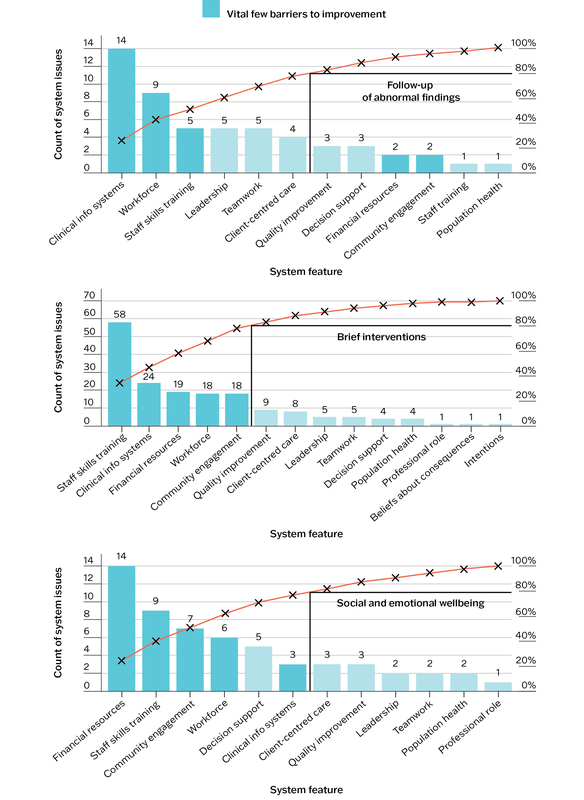
Figure 20.2 Using Pareto analysis to identify the “vital few” system barriers to wide-scale improvement: follow-up of abnormal findings, brief interventions, social and emotional wellbeing. Source: Matthews, J. Bailie et al. 2017.
Summary
This chapter has provided examples of a systems approach to CQI in PHC. The varied examples illustrate the benefit of people in complementary roles and at different system levels being involved in quality improvement. High-level policy support and action for CQI help to build sustainability of CQI processes at the health service and community level. Concurrent action at different system levels and across sectors has more potential to create synergy for change than efforts that are narrow in focus, due in large part to the interconnectedness of the systems that affect health. Strengthening systems in one area of health can reduce pressure on other systems; bridging a common evidence-to-practice gap can improve the quality of clinical care for clients with a range of health conditions.
A systems approach to CQI is situated within a broader systems approach to health services and health services research. It is important to acknowledge that not all system improvements are amenable to a classic CQI approach. Health systems research is a diverse and innovative field of research, and a range of mechanisms are required to improve health systems and other systems that affect health, such as legislation, justice, education, food production and social welfare. CQI is one key element in the coordinated and sustained action required to achieve improvement in population health outcomes and health equity.
References
Bailie, C., V. Matthews, J. Bailie, P. Burgess, K. Copley, C. Kennedy et al. (2016). Determinants and gaps in preventive care delivery for Indigenous Australians: a cross-sectional analysis. Frontiers in Public Health 4(34). DOI: 10.3389/fpubh.2016.00034.
Bailie, J., A. Laycock, V. Matthews and R. Bailie (2016). System-level action required for wide-scale improvement in quality of primary health care: synthesis of feedback from an interactive process to promote dissemination and use of aggregated quality of care data. Frontiers in Public Health 4(86). DOI: 10.3389/fpubh.2016.00086.
Bailie, J., V. Matthews, A. Laycock, R. Schultz, C. Burgess, D. Peiris et al. (2017). Improving preventive health care in Aboriginal and Torres Strait Islander primary care settings. Globalization and Health 13: 48. DOI: 10.1186/s12992-017-0267-z.
Bailie, R., V. Matthews, S. Larkins, S. Thompson, P. Burgess, T. Weeramanthri et al. (2017). Impact of policy support on uptake of evidence-based continuous quality improvement activities and the quality of care for Indigenous Australians: a comparative case study. BMJ Open 7(10). DOI: 10.1136/bmjopen-2017-016626.
Bainbridge, R., J. McCalman, M. Redman-MacLaren and M. Whiteside (2019). Grounded theory as systems science: working with Indigenous nations for social justice. In Antony Bryant and Kathy Charmaz, eds. The Sage handbook of current developments in grounded theory, 611–29. Thousand Oaks, CA: SAGE Publications.
Brimblecombe, J., C. van den Boogaard, B. Wood, S. Liberato, J. Brown, A. Barnes et al. (2015). Development of the good food planning tool: a food system approach to food security in Indigenous Australian remote communities. Health Place 34: 54–62. DOI: 10.1016/j.healthplace.2015.03.006.
Copley, K. and L. Patel (2021). The Northern Territory continuous quality improvement strategy. Darwin: Aboriginal Medical Service Alliance Northern Territory.
Ferlie, E.B. and S.M. Shortell (2001). Improving the quality of health care in the United Kingdom and the United States: a framework for change. Milbank Quarterly 79(2): 281–315.
Gibson-Helm, M., J. Bailie, V. Matthews, A. Laycock, J. Boyle and R. Bailie (2018). Identifying evidence–practice gaps and strategies for improvement in Aboriginal and Torres Strait Islander maternal health care. PLOS One 13(2): e0192262. DOI: 10.1371/journal.pone.0192262.
Heyeres, M., J. McCalman, K. Tsey and I. Kinchin (2016). The complexity of health service integration: a review of reviews. Frontiers in Public Health 4: 223. DOI: 10.3389/fpubh.2016.00223.
James Cook University (2019). Plan for healthy ageing in the Torres Strait. James Cook University. https://www.jcu.edu.au/news/releases/2019/july/plan-for-healthy-ageing-in-the-torres-strait.
Laycock, A., J. Bailie, V. Matthews, F. Cunningham, G. Harvey, N. Percival et al. (2017). A developmental evaluation to enhance stakeholder engagement in a wide-scale interactive project disseminating quality improvement data: study protocol for a mixed-methods study. BMJ Open 7: e016341. DOI: 10.1136/bmjopen-2017-016341.
Laycock, A., G. Harvey, N. Percival, F. Cunningham, J. Bailie, V. Matthews et al. (2018). Application of the i-PARIHS framework for enhancing understanding of interactive dissemination to achieve wide-scale improvement in Indigenous primary health care. Health Research Policy and Systems 16(117). DOI: 10.1186/s12961-018-0392-z.
Matthews, V., J. Bailie, A. Laycock, R. Bailie (2017). The vital few: key barriers to widescale improvement in Aboriginal & Torres Strait Islander primary health care. Presentation. 10th Health Services and Research Policy Conference, 1–3 November 2017, Gold Coast, Queensland.
McCalman, J., R. Bailie, R. Bainbridge, K. McPhail-Bell, N. Percival, D. Askew et al. (2018). Continuous quality improvement and comprehensive primary health care: a systems framework to improve service quality and health outcomes. Frontiers in Public Health 6: 76. DOI: 10.3389/fpubh.2018.00076.
McCalman, J., C. Jongen and R. Bainbridge (2017). Organisational systems’ approaches to improving cultural competence in health care: a systematic scoping review of the literature. International Journal for Equity in Health 16(78). DOI: 10.1186/s12939-017-0571-5.
McDonald, E., R. Bailie and T. Michel (2013). Development and trialling of a tool to support a systems approach to improve social determinants of health in rural and remote Australian communities: the healthy community assessment tool. International Journal for Equity in Health 12(15). DOI: 10.1186/1475-9276-12-15.
McDonald, E., R. Bailie and P. Morris (2014). Participatory systems approach to health improvement in Australian Aboriginal children. Health Promotion International 32: 62–72. DOI: 10.1093/heapro/dau003.
National Aboriginal Community Controlled Health Organisation (2021). Core Services and Outcomes Framework: the Model of Aboriginal and Torres Strait Islander Community-Controlled Comprehensive Primary Health Care. Canberra, ACT: NACCHO. https://csof.naccho.org.au.
National Aboriginal Community Controlled Health Organisation (2018). National Framework for continuous quality improvement in primary health care for Aboriginal and Torres Strait Islander people 2018–2023. Canberra: NACCHO.
Peters, D., N. Tran and T. Adam (2013). Implementation research in health: a practical guide. Geneva, Switzerland: World Health Organization.
Quilty, S., N. Frank Jupurrurla, R. Bailie and R. Gruen (2022). Climate, housing, energy and Indigenous health: a call to action. Medical Journal of Australia 217(1): 9–12. DOI10.5694/mja2.51610.
Quilty, S. and N. Jupurrurla (2022). How climate change is turning remote Indigenous houses into dangerous hot boxes. The Conversation, 17 June. https://theconversation.com/how-climate-change-is-turning-remote-indigenous-houses-into-dangerous-hot-boxes-184328.
Shortell, S., C. Bennett and G. Byck (1998). Assessing the impact of continuous quality improvement on clinical practice: what it will take to accelerate progress. Milbank Quarterly 7(4): 593–624.
Sollecito, W. and J. Johnson (2019). McLaughlin and Kaluzny’s continuous quality improvement in health care. Burlington, MA: Jones & Bartlett Learning.
Trees, J., T. Levett, K. Wynn and R. Ivers (2022). Ngununggula: the story of a cancer care team for Aboriginal people. International Journal of Whole Person Care 9(1): 50–1.
Tricco, A., N. Ivers, J. Grimshaw, D. Moher, L. Turner, J. Galipeau et al. (2012). Effectiveness of quality improvement strategies on the management of diabetes: a systematic review and meta-analysis. Lancet 379(9833): 2252–61. DOI: 10.1016/S01406736(12)60480-2.
1 McCalman, Jongen and Bainbridge 2017; Peters, Tran and Adam 2013.
2 Bainbridge, McCalman et al. 2019.
3 National Aboriginal Community Controlled Health Organisation 2021.
4 Heyeres, McCalman et al. 2016; McCalman, R. Bailie et al. 2018.
5 National Aboriginal Community Controlled Health Organisation 2018.
6 Trees, Levett et al. 2022.
7 National Aboriginal Community Controlled Health Organisation 2018.
8 James Cook University 2019.
9 Quilty, Frank Jupurrurla et al. 2022; Quilty and Jupurrurla 2022.
10 Brimblecombe, van den Boogaard et al. 2015.
11 McDonald, R. Bailie and Michel 2013.
12 McDonald, R. Bailie and Morris 2014.
13 McDonald, R. Bailie and Morris 2014.
14 J. Bailie, Matthews et al. 2017; Shortell, Bennett and Byck 1998; Tricco, Ivers et al. 2012.
15 Ferlie and Shortell 2001.
16 Sollecito and Johnson 2019, 314.
17 National Aboriginal Community Controlled Health Organisation 2018.
18 R. Bailie, Matthews et al. 2017.
19 National Aboriginal Community Controlled Health Organisation 2018.
20 National Aboriginal Community Controlled Health Organisation 2021.
21 Copley and Patel 2021.
22 Copley and Patel 2021.
23 Laycock, J. Bailie et al. 2017.
24 C. Bailie, Matthews et al. 2016; J. Bailie, Matthews et al. 2017; J. Bailie, Laycock et al. 2016; Gibson-Helm, J. Bailie et al. 2018.
25 For a breakdown of respondents’ roles and numbers see Laycock, Harvey et al. 2018.
26 Laycock, Harvey et al. 2018.