Chapter 19
Competency-based curriculum: Permanent transition in dentistry
Faculty of Dentistry
The learning environment of the clinic
Dentistry is a field of human health care where education principally trains students for the independent and proficient care of patients with oral and dental diseases and disorders. The learning environment is the dental clinic which is often housed within a tertiary medical hospital. Much learning, of course, is completed in traditional lecture theatres and seminars rooms, online and face-to-face but the clear understanding of student and educator is the goal of clinical performance. It has been suggested that ‘the clinic is the learning environment to which all our students aspire’ requiring the assiduous ‘transfer of knowledge from the basic sciences to the clinic by tuning and restructuring of knowledge’ (Rumelhart & Norman, 1978; Mullins, Wetherill & Robbe, 2003). How teaching best occurs in this environment, for the preparation of students to advance to independently provide patient clinical care, is an important and central field of enquiry for educators and clinicians alike.
Students, as trainee clinicians, are introduced to the learning environment of the clinic early in their careers. This aims to provide authentic, contextual learning and facilitate integration of knowledge from basic to clinical sciences uniquely afforded by the environment (Mullins, et al., 2003). In providing strong contextual learning, the environment is an example of a ‘community of practice’ featuring ‘mutual engagement’ of a number of participants (Lave & Wenger, 1991). Other important participants are regional Health Care Systems supporting the vast majority of patient care in accommodating the clinical environment and statutory national bodies, such as the Australian Dental Council, who are tasked with standard maintenance and recurrent accreditation of dental programs. Other participants are the professional associations, such as the Australian Dental Association representing a unified community of practitioners. In this setting, students are expected to simultaneously demonstrate diverse competencies, including a range of skills, broad knowledge-base, professionalism and empathic, ethical behaviour, supervised by clinical educators.
In many professions, clinical educators are themselves practicing clinicians, and share responsibility for patient care provided by student clinicians, with those students. The clinical educator often employs a range of teaching modes and their supervision, at its best, may be defined as the ‘provision of monitoring, guidance and feedback on matters of personal, professional and educational development in the context of patient care’ (Hirons & Velleman, 1993; Irby, 1995; Kilminister, Jolly & van der Vleuten, 2002). The student/clinical educator relationship has also been suggested to mirror the therapeutic alliance that exists between patient and physician, in representing an educational alliance (Tiberius, Sinai & Flak, 2002). Whilst the relationship can benefit both student and educator, Fallon and co-workers found that effective clinical teaching in medicine also has an impact on patient outcome which can improve when direct supervision of the student clinician is combined with focused feedback. (Fallon, Wears & Tepas, 1993). 210
Clinical teaching in a dental education context has been less extensively examined and is different from that of medical clinical teaching. (Romberg, 1984; Chambers, Geissberger & Leknius; 2004). Technical competence in the fine motor skills required in dental procedures is an important characteristic of dental education. Unlike clinical teaching in undergraduate medicine, undergraduate dental clinical teaching must facilitate the development of competence that enables a student to autonomously engage in the privilege of patient care at graduation guided by reflective practice (Greenwood, Lewis & Burgess, 1998). Reflective practice is a way for beginners in a discipline to recognise consonance between their own individual practices and those of successful practitioners. (Schön, 1996).
Whilst in business and industry the competence-model is reported to benefit a broad and large range of stakeholders in, for example, articulating workforce needs, focusing training, activating development efforts and planning future trajectories, it is not clear if this is also so in dental education. There is little organised research that can point to the long-term value and impact of competency-based curricula on student development of clinical competence and patient outcome. (Hager & Gonzi, 1991; Gonzi, 1993). Similarly, there is little organised research that clarifies how students learn clinical competence. Chambers has argued, however, that competency-based education has raised these matters to conscious discussion. (Chambers, 2001). This attests to the sense of a curriculum in transition.
Drivers of change: The move to competency-based curricula in dentistry
The need to consider the merits of a competency-based curricula has been faced by many professions. Probably the earliest driver of this for the Faculty of Dentistry was the issue of a report by the Institute of Medicine (IOM) in 1995; Dental Education at the Crossroads: Challenges and Change (Field, 1995). This report recommended significant curricular reforms relative to educational contact and presentation in dentistry. In 1998, the Commission on Dental Accreditation of the American Dental Association adopted predoctoral dental program accreditation standards requiring competency-based assessment. This was then placed in the light of the first ever US Surgeon General’s report on oral health published in 2000: Oral Health in America: A Report of the Surgeon General (Satcher, 2000). This report detailed the most common oral health problems while highlighting the need to increase access and care for a range of underserved populations in the US. Implications of the reports gave rise to curriculum reforms which included ‘redesigning curriculum to incorporate competence-based learning principles, decompression of the curriculum by eliminating irrelevant or duplicated material and revitalising underlying sciences via evidence-based approaches’ (Hendricson & Cohen, 2001). The American Dental Education Association in a report, the Competencies for the New Dentist (2004) equated graduation (that is, with a first dental professional degree) with the attainment of professional competency through a continuous process of professional improvement divided into five stages: novice, beginner, competent, proficient and expert as described by Dreyfus and others (Dreyfus & Dreyfus, 1986; Bruer, 1993).
Political unifying changes in Europe also impacted on educational processes. With the signing of the Bologna Declaration in 1999 by the Ministers of Education of 29 European countries, an aim to establish a European Higher Education Area by 2010 achieved strong significance in advancing the importance of competency-based dental education. The groups tasked with facilitating convergence in the dental education area, 211the Association of Dental Education in Europe (ADEE) moved to organise competencies for the graduate dentist into a professional profile that would have applicability amongst all the nation members of the European Union. (Plasschaert, Holbrook, Delap, Martinez & Walmsley, 2005). This, together with similar initiatives in North America and the United Kingdom, provides an overview of competency-based curricular design available in dental education. (Boyd, Gerrow & Chambers 1996; American Association of Dental Schools, 1997; General Dental Council, 2002).
These reports caused strong resonance in the Australian dental educational community. In 1999 to 2000, the Faculty of Dentistry at the University of Sydney sought to respond to some of these strong external issues but also had pressing internal issues with which to contend. The internal imperative was the implications of an advanced curriculum reform already completed by a faculty with which dentistry had strong integration both educationally and professionally. The Faculty of Medicine had by now already implemented its new graduate-entry, four-year problem-based learning (PBL) curriculum, the Graduate Medical Program, which had immediate logistical and philosophical implications for the provision of basic science teaching for the Faculty of Dentistry. In 2001, the Faculty of Dentistry therefore, introduced the BDent program, replacing the former five-year, undergraduate-entry and largely didactic Bachelor of Dental Surgery (BDS). The BDent PBL-based curriculum was designed to align with best practice in dental education identified in international standards in literature and by University of Sydney Academic Board policies whilst contributing to the objectives of the University Strategic Plan in the creation of a strong evidence-based scholarly environment. (Klineberg, Massey, Thomas & Cockrell, 2002). The reform had begun and it was soon recognised that a new curriculum required new and evidence-based educational modalities to be developed to support its objectives. Meeting these challenges became the driving energy of a number of faculty research projects in both scholarship of learning and research paradigms and these are described below.
Scholarship of learning and teaching projects
The faculty curriculum committee was tasked with the development and implementation of a competency-based curriculum. This was considered in terms of three broad phases: planning, implementation and evaluation. Each phase was characterised by a series of integrated projects in both the scholarship of learning and teaching, and in educational research. The results of these projects were presented throughout the timeline of the curriculum development, at dental and medical educational conferences, nationally and internationally, and published in refereed journals, to seek the benefit of critical review and reinvest that benefit into the phases. The curriculum committee had final oversight of developments providing broader comment. An added challenge to the committee was the need to maintain the integrity of the exiting BDS degree program whilst simultaneously developing and implementing the BDent program.
Planning the curriculum
Development of the dental clinical competencies. An aim was defined as the design of the competency-based structure of the new dental program. The method featured aspects of project management often used in business: organising the team, defining the project, planning the stages and activities, activating goals, reporting the results, reviewing the process. The team consisted of a cross-section of discipline experts and 212educators led by a senior academic with strong educational experience. Firstly, a literature search was completed on competency-based education. This yielded a working definition of competency as a broadly stated general description of an essential patient care skill or professional role that an entry-level general practitioner must be able to perform unassisted and unsupervised. In addition, it was considered that maintenance of competence required reflective practice and was a professional and ethical responsibility (Willis & Dubin, 1990). Secondly, a search and critical review of online competency statements and resources published by dental schools and dental educational associations nationally and internationally was completed. Thirdly, the various lists were reviewed by the project group by determining the behavioural objectives comprising the competency, the direct applicability to dental practice and the relevance of the competency to the program mission. A example for the competencies was that adopted by the Association for Canadian Faculties of Dentistry. The competencies for the BDent program was rationalised to a final list of 50 items set out in one of a series of five curriculum planning papers. The team reiteratively reviewed the competencies in terms of discipline emphasis and balance in order to safeguard overall integrity and to facilitate the networking of new knowledge patterns. This networking was preliminarily completed by grouping competencies into multi-disciplinary domains of knowledge. The final stage of the project was the determination of the following components for each competency: educational outcome, specific knowledge, pre-clinical skills and clinical skills. Outcomes of this published project were the identification of the competencies and their operational components, acceptance by consensus in the faculty of the competency-based structure and a recognition of the imperative of review of the competencies in the future (Klineberg et al., 2002).
Development of a new dental competency-based unit of study. An aim for this project was the operationalising of the competencies into units of study, the basic packets of academic programs. Utilising a similar method already establish above, the curriculum team critically adapted units of study from the Faculty of Medicine Graduate Medical Program in the three themes of Life Sciences, Personal and Professional Development and Dentist and the Community. These three themes provide the framework for the goals of the program, for the development of the curriculum and for assessment. Uniquely dental units of study where developed to integrate those competencies encompassing the necessary communication, reasoning and clinical skills required to provide accurate oral health diagnosis as well as the clinical understanding and technical skills needed to treat dental patients. This occurred by the consolidation of about sixteen individual dental disciplines into two new dental themes, Total Patient Care, for senior years, and Foundations of Total Patient Care, for junior years, of the BDent program. Each of these new themes required the scholarly development of a number of new learning strategies and modalities which were addressed in the implementation phase (Daly, Groenlund & Moran, 2002).
The BDent website for the dental program at the University of Sydney. An aim in this project was to develop a program website that supported learning by providing staff and students with access to curriculum in a timed, controlled way. The curriculum team employed an information technology specialist to develop the website. Technical advice suggested that the website needed to be password protected, feature a bulletin board to announce news, feature customised online lecture timetables, allow timed 213release of resources, enable users to submit feedback through a forum, allow ‘staff only’ access to certain resources and provide multimedia ‘triggers’ to enhance learning. Student response to the website has been monitored consistently with unsolicited and solicited student and teacher feedback and focus group sessions. Outcomes have been excellent utility by students and educators but ongoing maintenance of the website has been imperfect. This project and the website were presented in 2002 at the American Dental Education Association Annual Conference in San Diego, USA and the presentation was rewarded with an international award (Gerzina, Lester & Sefton, 2002; Reynolds & Gerzina, 2002)
Establishing benchmarking in the Faculty of Dentistry. This funded research project aimed to develop a method for benchmarking teaching and learning in response to an institutional need to validate the new BDent program. A qualitative method was used. A collaborative institutional partner, University of Adelaide, was identified, and the partners negotiated on the areas of teaching and learning to be benchmarked. Problem-based-learning approach and assessment were nominated as those areas. A list of quality indicators for these aspects of teaching and learning were first developed conceptually and then validated by the literature. Then, using a quality enhancement framework, levels of achievement for each indicator were developed (Kember, 2000). The project yielded a strong, evidence-based charting of performance indicators which were mutually developed with the benchmarking partner and which represented an agreed model for a benchmarking project to progress to the next stages of implementation and evaluation. It was perceived that the model could be readily adapted for any benchmarking project in all levels of education; primary, secondary, tertiary and continuing. Another significant outcome of the project has been the commendation by accreditation bodies of the dental program in Sydney for the benchmarking initiative and the expansion of the project to include another partner, the Faculty of Dentistry at the University of Toronto, Canada (Henderson-Smart, Winning, Gerzina, King & Hyde, 2006). This project has been presented in several forums including national and international conferences (Dempster, Grad & Gerzina, 2005a).
Implementing the curriculum
Development of dental clinical competency logbook. An aim was to develop, and evaluate effectiveness of, a learning resource to organise and track the completion of competencies by students, promote self-reflective practice and enable criterion-referenced assessment. The curriculum team used a method including a database literature search for clinical log books in the professions of dentistry, nursing and surgery. Desired characteristics for learning and assessment in the logbook were defined and enabled a stepwise development of the logbook. Student evaluation of the logbook was completed by questionnaire using a six-point Likert scale and using 20 items. These items were drawn from statements articulated by students during informal focus group sessions about the logbook. An open-ended comment section was included. Several results and outcomes have occurred. Student evaluation (response rate 73%) of the logbook has been favourable with strong support, particularly, for the self-assessment section. The Clinical Competency Logbook has now been in place for junior years in the BDent program for the last seven years (with annual refinement). The logbook has been viewed favourably by accreditation teams (Australian Dental Council Accreditation Report, 2005). Currently, a new Scholarly Project is advancing 214the modality into an electronic version, the eLogbook, and extending its use into all years of the program. (Moran & Gerzina, 2001).
Assessing the development of clinical competence. This project aimed to assess student development of specific clinical competencies which are considered essential for independent high quality provision of dental care for patients in a dental surgery. To achieve this aim, the working group utilised a qualitative method. Data derived from websites of dental schools throughout the North America, Europe and UK were systematically searched for detail on assessment tools and an extensive literature search through ERIC and MEDLINE were presented to the working group for discussion and critical review. In addition, current faculty assessment practices and University of Sydney Academic Board Policy on assessment completed a data set for elaborate discussion. Methods included consolidation in the working group, of the understanding of sound assessment practice. Practically, the competencies were arranged in interdependent groups enabling the competencies to be directly linked to areas of the curriculum. There were several outcomes. A scheme of integrated clinical assessments was developed that could measure the acquisition and mastering of the dental clinical competencies. The new assessment tools were criterion-referenced, authentic, fair, realistic and meaningful, recognising the development of student clinical competence as proceeding from the cognitive to the behavioural with increasing dependence on the provision of dental care as the assessment focus. Sessional assessment and self-assessment are used in all years of the program, embodied in the clinical competency log-book. In the largely pre-clinical early years, further formal clinical assessment also includes both integrated and discipline specific clinical assessments. In the predominately clinical years 3 and 4, competency assessment is founded on sessional clinical assessment, completion of clinical thresholds, case presentations and in clinical mentor reports. Assessment of student completion of clinical competencies is now completed in several ways in the program, aiming to authentically present an accurate overview of a student’s clinical development.
Evaluating the curriculum
Effectiveness of assessment in integrated clinical competencies. This research project aimed to qualitatively assess the effectiveness of the newly formulated clinical assessment in the junior years of the program (BDent 1 and 2). In this project methodology, a questionnaire was designed that explored the value of the assessment format in accurately reflecting student performance, enabling valuable feedback and enhancing student self-evaluation. Both students and assessors were provided with the opportunity to provide feedback. The questionnaires were constructed based on responses to a six-point Likert scale with responses ranging from 1 (strongly agree) to 6 (strongly disagree). Data were entered into SPSS (Statistical Package for Social Sciences) and analysed. Open-ended questions were also included. Results from the questionnaires were valuable. Differences in perceptions of the value of the assessment grades varied between the student groups and between the assessors. Tentativeness in the use of the full range of the grades characterised students and assessors with less familiarity with assessment goals. Criteria for the grades and guidelines were found to be meaningful by all groups and simplification of logistical issues was seen as a requirement for compliance by students and assessors. The current study highlighted the value of a robust and sensitive grading scale in clinical and pre-clinical assessment 215in dentistry. Some data from this project are shown in Figure 19.1. An outcome of the project has been that clinical sessional grading using non-numerical grade descriptors is now completed by both the student (in a reflective self-assessment) and by the clinical educator for every clinical session. The grades are able to be summatively processed supporting progression decision but remain the primary source of feedback to students on their development of clinical proficiency. (Hyde & Gerzina, 2002; Russell, Reynolds, Fairley, Hyde, McInerney & Gerzina, 2005)
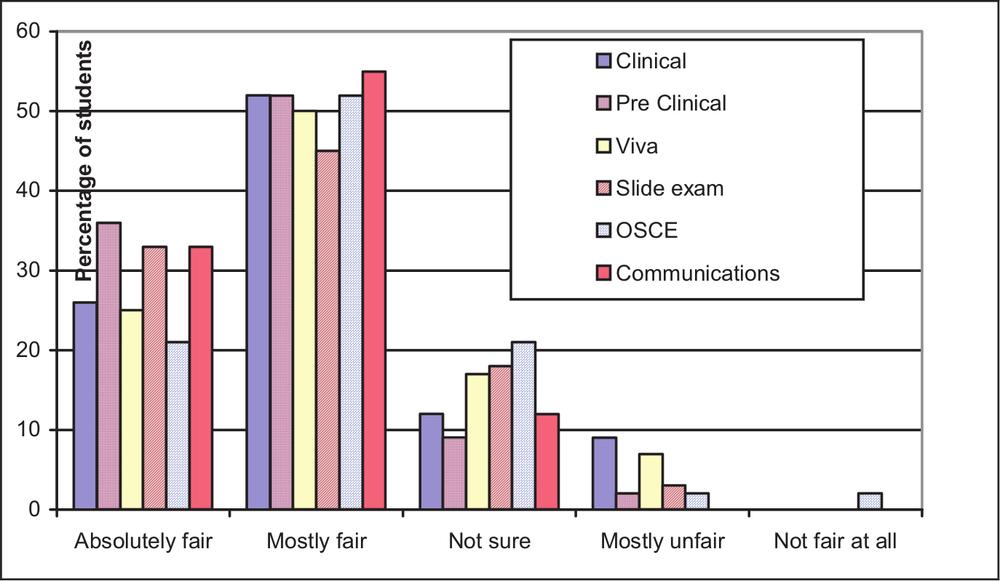
Figure 19.1. Students’ ratings of the perceived fairness of each component of the Clinical Assessment (n=44, RR 65%)
Student use and perceptions of different learning aids in relation to formative assessment, and to becoming a clinician. This research project aimed to determine student perceptions of a recent written formative assessment in terms of the usefulness of various learning aids both in preparing for the assessment and in preparing to be a dental clinician. The project also aimed to establish correlations between approach to learning and perceptions of assessment and learning aids. The Study Process Questionnaire (SPQ) (Biggs, 1987) and two specifically designed questionnaires were used featuring a six-point Likert scale. Correlations between student approach to learning as assessed by the SPQ and perceptions of assessment and learning aids were evaluated. The SPQ yields three factor scores ‘deep’, ‘surface’ and ‘achievement’. Relationships between approach to learning and perception of the written formative assessment were examined in the first instance. Correlations between approach to learning and student perception of the usefulness of learning aids in preparing for assessment and preparing to be a clinician were examined in the second instance using Spearman correlation coefficient and a significance level of p<0.05. Theoretically expected associations were seen, in that surface learning was associated with students’ concerns regarding whether assessment items reflected curriculum content, a valuing of lectures as a learning aid and low scores for group seminars, called theme sessions. 216
Table 19.1. Significant (and trend to significant) correlations between approach to learning and perceptions of assessment and learning aids
| Approach | Question | Correlation |
|---|---|---|
| Surface | The MEQ questions were representative of | r = -.307 |
| the curriculum content* | p = .07 | |
| I find theme sessions a useful learning aid in | r = -.512; r = -.387 | |
| preparing for assessment/clinical wo | p = .002; p = .024 | |
| I find lectures a useful learning aid in preparing | r = .415 | |
| to be a clinician | p =.015 | |
| Deep | The MEQ paper tested clinical application of | r = .374 |
| basic and clinical sciences | p = .03 | |
| I don’t find independent study groups a useful | r = -.296; r = -.275 | |
| learning aid in preparing for assessment/ to be a clinician ** | p = .08, p = .11 | |
| I find clinical days a useful learning aid in | r = .303 | |
| preparing to be a clinician | p = .08 | |
| I don’t find learning topics a useful learning aid in | r = - . 277; r =-.330 | |
| preparing for assessment/ to be a clinician ** | p = .09, p = .06 | |
| Achievement | Written formative assessment helped to clarify the | r = .392 |
| level of knowledge and understanding required | p = .02 | |
| I will change my approach to study as a result of | r = .323 | |
| my experience with the first formative assessment | p = .06 | |
| Formative assessment failed to give me a clearer | r = -.287 | |
| understanding of my strengths and weaknesses ** | p = .10 | |
| I don’t find learning topics a useful learning aid | r = -.390; r = -.317 | |
| in preparing for assessment/to be a clinician** | p = .02; p = .07 | |
| I don’t find independent study groups a useful | r = -.346 | |
| learning aid in preparing for assessment** | p = .04 | |
| I don’t find on-line assessments a useful learning | r = -.332 | |
| aid in preparing for assessment ** | p = .05 | |
| I don’t find written formative assessments a | r = -.424 | |
| useful learning aid in preparing for subsequent assessments ** | p = .01 |
* negative correlation, positively framed item; ** negative correlation, negatively framed item r = correlation coefficient comparing paired responses; the first r value refers to correlations with assessment while the second refers to correlations with preparing to be a clinician
p < 0.05 considered significant; p < 0.1 considered to be a trend to significance; where two values are given, the first r and p values refer to correlations with assessment while the second refers to correlations with preparing to be a clinician
(Source: Gerzina, Worthington, Byrne & McMahon, 2003)
Deep learning was associated with a perception that the assessment tested application of basic and clinical sciences and a valuing of both independent study groups and learning topics as learning aids. An achievement orientation to learning was associated with a valuing of formative assessment as a learning aid and an intention to modify study habits as a result of participating in formative assessment. Some data from this project are shown in Table 19.1. The findings provided insight into student learning in a PBL context which will meaningfully inform both educators and curriculum developers (Gerzina, Worthington, Byrne & McMahon, 2003). 217
Competency-based dental clinical teaching: perceptions of students and educators. This research project aimed to explore perceptions of dental student clinicians and clinical educators about dental clinical teaching to provide primary data for dental researchers and educators. Student focus group data provided background for development of a questionnaire which explored three themes related to clinical teaching. Twenty-one educators and 45 student respondents completed the 25-item questionnaire. In the theme of the educator/student relationship no statistically significant differences were seen between educator and student group perceptions. In the theme of educational theory applied in dental clinical teaching, a statistically significant difference was seen between educator and student groups in perceptions of the value of pre-clinical instruction in senior clinical years and in perceptions of the value of a clinical log book. In the theme of skills required for clinical dental practice, a statistically significant difference was seen between educator and student groups in the perceived value of a critical appreciation of evidence-based practice as one of the skills. Some data from this project are shown in Table 19.2. The study overall indicated that the dental clinical learning environment supports close perceptual conformity between students and clinical educators in regard to what each group considers to be ‘good practice’ in clinical teaching. The findings of this study indicate that some techniques that have been advocated to enhance clinical learning, such as evidence-based teaching methods, require further investigation (Dempster, Grad & Gerzina, 2005b).
Table 19.2. Comparison of educator and student perceptions in regard to the application of educational theory in dental clinical teaching
| Questionnaire Statement | Educators | Students | |||||
| Median | Mean | S.D. | Median | Mean | S.D. | S | |
| The PBL form of teaching has supported the development of the ability to provide dental clinical care of patients | 3 | 3.4 | 0.5 | 4 | 4.2 | 0.5 | NS |
| Small group teaching, such as tutorials, are valuable to the development of dental clinical skills. | 2 | 2.2 | 0.6 | 2 | 2.5 | 0.4 | NS |
| There is a clear link between the theory and the clinical practice of dentistry in the dental program. | 3 | 3.3 | 0.3 | 2 | 2.3 | 0.2 | S P<0.003 |
| Formal lectures are valuable to the development of dental clinical skills. | 3 | 2.6 | 0.9 | 2 | 2.3 | 0.5 | NS |
| Grading student performance in clinical sessions should use a ‘pass’, ‘credit’ etc system to best support student development as dental practitioners | 3 | 3.2 | 0.7 | 3 | 3.4 | 1.5 | NS |
| A student record of their completed patient care, such as a clinical log book, assists student preparation for independent practice. | 3 | 2.9 | 0.3 | 4 | 3.7 | 0.2 | S P<0.004 |
Rating scale: 1=always agree, 2=agree, 5=disagree, 6=strongly disagree.
(Source: Gerzina, McLean, Fairley, 2005)
218Preparedness of dental clinical educators to supervise student clinical competence. The aim of this research project was to provide data on the clinical educators’ perceptions of clinical teaching and their degree of confidence to clinically supervise student clinicians during student care of patients. A mixed qualitative/quantitative method was used. A questionnaire was developed for all clinical educators containing both open- and closed-structured items reflecting all the Clinical Competencies of the program. The closed-items section used a 5-point Likert scale to ascertain educator perceptions of, firstly, their degree of confidence to supervise students completing each of the clinical competencies and secondly, their perception of their own teaching characteristics compared with a list of characteristics associated with effective educators in the literature. An open item section queried educator ideas about aspects of educator development in dental clinical teaching. Chi square (p<0.05) was used to compare results between participant educators (general dentists, specialist dentists) and Pearsons product-moment coefficient was used to determine correlations between years of teaching or gender and perceptions reported. Results were as follows. A response rate of 67% to the questionnaire was seen amongst the educator participants (63% male, 30% specialist or possessing a higher degree) and these participants had an average of 9 years clinical teaching experience. A majority of educators (greater than 70%) felt well prepared to supervise student clinicians completing 60% of the listed clinical competencies, such as ‘conducting a dental clinical examination’. Educators reported feeling unprepared to supervise students in 17% of listed competencies, such as ‘performing periodontal surgery’. They reported being uncertain about their confidence in supervising students completing another 17% of the competencies such as ‘managing needs of physically challenged patients’. Educators rated themselves as possessing a large number of the characteristics of effective educators but were unsure about some characteristics, such as ‘gauging a student’s need for independence’ and ‘linking theory to practice’. Specialist dental educators considered themselves confident to supervise in a significantly larger number (p<0.05) of the clinical competencies than general dental specialists; no significant differences were seen in comparing educators of more or less than 10 years teaching experience; some significant gender differences were seen in educators confidence supervising specialist-level competencies (Gerzina & Down, 2006).
Conclusions
The competencies present, in a comprehensive and convenient list, the ingredient skills and capabilities that the entry-level clinical practitioner needs in order to conduct independent practice. Typically, curriculum designers attempt to realise the vision of curriculum planners in choosing an educational approach that serves the educational mission. Curriculum development and implementation is most usefully approached in a structured strategic way, aiming to take value from the benefits of faculty positioning in a research-intensive learning environment of a university. A ‘traditional’ way to design a curriculum is a linear process starting with a needs assessment, goal development, design of the objectives, teaching strategies and finally evaluation methods (Harden, 1986). However, the challenging issues emerging for professional educators and curriculum designers relate to the translation and adaptation of these skills and capabilities into learning interactions and events that are simultaneously authentic, 219stimulating, valid and practical and align to the expectation of the health care setting in which most clinical training programs are conducted.
The current chapter has aimed to present the perspective and a sample of the endeavours of a clinical faculty in a large research-focused university as it engages with the enormous challenge and promise of competency-based curricula and the slow turning of the faculty ship onto that course. Competence of the graduate and then of the graduate clinician were discussed in the light of the clinical learning environment and the issues of multiple stakeholders in clinician training. Our own faculty has made some tentative but exciting inroads into understanding the educational power of a competency-based approach to curriculum design, development and implementation through a broad and growing number of projects in the scholarship of learning and teaching and in research enquiries. Presentations on the endeavours and findings have been shared in the educational community nationally and internationally and critically reviewed. Current new initiatives in the faculty have commenced in patient care teams, utilising interprofessional learning in elaborating the dental team with other oral health practitioners and with other practitioners. An abiding reality remains in the sustainability of the curriculum in transition.
The growing educational emphasis on competence at graduation will continue to affect educational business. International consideration of the value and costs of competency-based curricula as applied in higher education continues to be elaborated by discussion and publication. Growing evidence and research analysing the effects of the approach almost guarantee an ongoing exciting future. But perhaps, the final analysis of the value and effectiveness of the approach may lie in the ability of the students and the educators alike to recognise a curriculum in transition and acknowledge the keen sensitivity of that curriculum to emergent evidence. 220