3
Adapting continuous quality improvement for primary health care
Why is adaption needed?
The CQI approach to health care has been dominated by the hospital sector, where a relatively controlled environment and relatively routine models of care have some similarities with the industrial sector from which CQI evolved. The standard characteristics of CQI, as described in McLaughlin and Kaluzny’s seminal text1 and cited by Sollecito,2 reflect these features: links to the organisation’s strategic plan; a quality council made up of the organisation’s top leadership; staff training; mechanisms for selecting improvement opportunities; and the formation of process improvement teams. Staff support for process analysis and redesign, policies that motivate and support staff participation in process improvement, and application of the most rigorous techniques of the scientific method and statistical process control are also specified. Lacking in the list of features is client or consumer involvement in CQI, an aspect of quality receiving increased attention. While the CQI structures and processes identified are feasible in medium-size or large hospitals, or for managing networks of community-based health services through centralised organisational structures, they do not reflect the way most PHC is delivered. CQI needs to be modified for application in PHC.
PHC delivery models
As highlighted earlier, PHC services tend to have these characteristics:
- are widely dispersed across diverse contexts
- are of varied size – some delivery models include multiple sites and clinicians (for example, nurses, doctors, health workers), some have only a few clinicians (in some cases one) and administration staff
- are of varied composition (for example, a medical practice, a group of medical and allied professionals or a community-based organisation)
- are governed through a variety of small business, corporate or government structures
- are relatively independent or autonomous, and reliant on professionalism for ensuring quality.
Compared with hospitals and corporate networks, individual PHC services and practices are less likely to have a shared (or any) strategic plan that local staff can identify with, or a quality council to which most staff feel accountable. Where efforts to establish the types of structures and processes described by McLaughlin and Kaluzny have been made in PHC, the participation or engagement by individual PHC services and practices has varied greatly, with limited effect across the PHC service system or at a population level. Despite these challenges, strategic and systemic approaches to improvement are necessary for dealing with the complexity of PHC delivery and for improving care quality.
Strategic and systemic approaches to improvement are necessary for dealing with the complexity of PHC.
Traditions in healthcare delivery also challenge systemic approaches to PHC and CQI. Up to the 1970s, PHC was largely perceived as a cottage industry, in which “healthcare was seen as a craft or art delivered by individual professionals who had learned by apprenticeship and who worked independently in a decentralised system”.3 Practitioners generally developed their own systems for recording the care they provided and were individually accountable, with no mechanisms for linking records with other providers and limited opportunities to share learning. While some policy debate continues to focus on the weaknesses of the professional system for improving quality (due to excessive professional autonomy and protectionist practices by “guilds” of practitioners), this historical reliance on the professionalism of health practitioners for self-regulation and quality of care is changing. The development of clinical guidelines and of more standardised clinical information systems are examples. A systems approach to CQI is one way of sharing ownership for quality improvement and mobilising change.
Timing and scope of care
In PHC, items of service need to be delivered to members of the service population at relatively infrequent intervals, when people present for care. For example, blood pressure checks for generally healthy adults may be recommended once a year, or once every two years, as a preventive health strategy. Glycated haemoglobin (HbA1c) tests are recommended once every three or six months for people with diabetes. Care delivery for these service items relies on people accessing care for checks (or for acute care that may or may not be related) or being accessible through outreach services. The measurements need to be taken over a sufficiently long period (sometimes years) for changes in the level of care delivery to be observed.
Measurements need to be taken over a sufficiently long period for changes in the level of care delivery to be observed.
In addition, a very broad scope of care is delivered through PHC maternal, child and preventive health care, care and management of chronic conditions, mental health, sexual health and so on. Within each of these areas of PHC, there are essential items of care to be delivered in order to meet expected standards of care.
Quality improvement challenges and responses
For the reasons we have identified, the gains made in the hospital sector during the 1980s and 1990s (re-engineering care delivery, improving care processes and adopting CQI techniques) have been slower and more challenging to implement in the PHC sector. The effects of poor-quality PHC may not be as immediate and dramatic as safety incidents in hospital care, where patients are generally sicker and treatments more intensive. But poor access to care, unacceptable (for example, disrespectful) care, missed opportunities, missed diagnoses, inappropriate investigations or treatment, and adverse events related to poor quality of PHC can all contribute to unnecessary human suffering and waste on a massive scale at the population level.
PHC teams and practices have the challenge of identifying which areas and which items of care should be the focus of their improvement efforts. This requires knowledge of what is being done relatively well and not so well by the service or practice, which in turn requires complete client records that accurately reflect the care delivered. Individual practitioners and teams also require knowledge about what is a reasonable level of care delivery in a population group: clear standards and measures of care quality established through quality assurance processes. While striving for 100 per cent delivery of “essential” care items is the ideal, it is rarely achievable, and is often much less than 100 per cent for a range of reasons. Teams need to prioritise improvements that are achievable and that offer the most benefit to clients.
PHC teams need to prioritise improvements that are achievable and that offer the most benefit to clients.
In addition, CQI requires comparable data from other PHC services and practices, to help benchmark quality of care. Local and regional variability in health care has long been known to exist, but there is a lack of evidence of this variability across PHC services on a wide scale and across the broad scope of clinical PHC. This is largely for reasons related to the diverse and dispersed nature of PHC services, and associated challenges in coordination, planning, delivery, monitoring and evaluation of PHC systems.
Substantial progress has been made in important areas, including the development, implementation and increased acceptability of clinical best-practice guidelines,4 the development of data systems that can support CQI and the use of “collaboratives” as a means of improving quality5 (see Chapter 7). Health practitioners and services have also embraced the concept of “client-centredness” to address the care needs and values of individual clients. Designing services that are appropriate and responsive to clients’ needs and the local context is especially important in PHC, to ensure easy and timely access to preventive care and treatment of health conditions throughout the life course. These PHC principles are strong motivators for staff to engage in CQI. PHC and CQI also have core concepts in common: both emphasise the importance of teamwork, and both PHC and CQI advocate systems approaches and systems thinking as a way of achieving better client outcomes.
PHC and CQI have core concepts in common.
The integrated nature of PHC can extend the benefits of improvement interventions, because system changes targeting one group of clients frequently flow on to benefit other groups. For example, changes made to a clinical information system to generate automated reminders when child health checks are due can be used to schedule other items of care for other groups; skills developed to provide brief interventions for smoking have application for other behavioural health risk factors.
Applying CQI
Consistent with the features of PHC delivery, CQI approaches need to allow practitioners and managers a high degree of autonomy to respond to local circumstances and population needs, and time to observe improvement.
Effective CQI in PHC has these characteristics:
- use of adaptable tools and processes
- use of clinical practice guidelines
- preparedness to begin in at least some areas
- use of local data and benchmarking
- active management
- “no blame” culture
- leadership by primary healthcare teams and communities
- participatory interpretation of data
- design of interventions to suit local conditions
- sharing of learning across teams
- investment by the health service and region
- improvement initiatives in four categories.
We will look at each of these in more detail.
Use of adaptable tools and processes
One size does not fit all: CQI tools and processes need to be readily adaptable to suit the context and capacity of each local PHC team or practice.
Use of clinical practice guidelines
Regardless of the tools used, CQI in a clinical context is guided by locally relevant clinical practice guidelines.
Preparedness to begin in at least some areas
It is important to start CQI from where the service is at. PHC services and practices have different levels of readiness for CQI. Where accurate data on care processes are not consistently available, this is often due to poor or fragmented clinical information systems. It is important not to wait for perfect data, but to focus efforts on where the biggest gains can be made – such as improving systems for accessible and reliable clinical records. Staff use of data in CQI cycles can act as a catalyst for improving data quality.6
Use of local data and benchmarking
Access to local data enables PHC teams to target improvement efforts where they will most benefit their service population. It is useful and important to have data from other PHC services for comparison, with the greatest value of benchmarking being in how data are used to gain deeper understanding of the influence of local contexts and service systems.
Active management
CQI needs to be actively managed and facilitated as part of core business. Active management can take various forms, and may involve dedicated CQI facilitators or coaches, regular progress reviews, the identification of CQI leaders who are not necessarily in management roles, and regional support structures.7
“No blame” culture
As in other healthcare settings, a “no blame” culture is essential for PHC staff to embrace CQI. To establish and sustain this culture within an organisation, managers at all levels need to understand and be committed to CQI, and have a relationship of trust with practitioners.8 Clear distinction needs to be made between collecting data for reporting purposes and using data to drive improvement.9
Leadership by PHC teams and communities
PHC teams need to be able to selectively monitor items of care (or indicators) in locally identified priority areas for improvement (for example, diabetes management, childhood anaemia). Priorities are typically selected based on comparing performance between areas of care within the local health service or practice, as well as comparing performance with other services (for benchmarking). Priorities may also be informed by client groups. Local ownership of CQI contrasts with top-down quality improvement programs that focus on a small number of indicators that are prescribed by senior policymakers. Such top-down approaches tend to rely on data systems of questionable quality and insufficient detail, and the top-down approach creates perverse incentives for accuracy in reporting of data.
Local ownership of CQI contrasts with top-down quality improvement programs.
Related to ownership, staff members need to value the use of data for improvement purposes and believe they can influence change.10 This comes from demonstrated improvements in care and clinical outcomes for clients, and increased confidence and skills as teams implement CQI.
Participatory interpretation of data
The meaningful interpretation of CQI data and the development of improvement strategies requires insight into the complex interactions between practitioners and clients, cultural and contextual factors, the nuanced decision-making that occurs, clinical system design and how all of these factors interact.11 Depending on the service context and structure, CQI may involve input from people in a range of PHC delivery roles: for example, clinicians, administration staff, cleaners, drivers, managers, visiting staff who provide specialised services, clients, families or carers and communities.12
Design of improvement interventions to suit local conditions
There is strong evidence that improving the quality of care requires a good match between the conditions or context for care delivery, and the strategies used to achieve improvement.13 Often, cultural and social influences need to be considered, emphasising the importance of local knowledge for ensuring that improvement strategies have practical relevance and address systemic problems.14
Improvement interventions should be designed or adapted to suit local conditions.
Sharing of learning across teams
Sharing knowledge about CQI and learning practical information from others about what works is particularly valuable for PHC teams, because of the dispersed location and relatively small scale of many PHC services.15
Investment by the health service and region
CQI requires clinical leadership and administrative support. It also requires specific investment to support the development of staff capability and systems, and the ongoing use of quality improvement tools and techniques to enhance health services for communities and individual clients. Regional CQI support systems can be important for supporting and coordinating these functions, due to the limited resources of PHC practices and smaller services. Such systems reflect supportive CQI policies at regional or national levels of the healthcare system.16 CQI approaches are most effective when the external environment is supportive.17
Improvement initiatives in four categories
Most CQI initiatives in PHC aim to improve the delivery of recommended care processes, as specified in practice guidelines. CQI approaches and activities are likely to involve localised improvement efforts; organisational learning; process re-engineering; or evidence-based practice and management.18
- Localised improvement efforts: CQI processes are used by PHC teams to identify and address improvement needs or opportunities (for example, the use of audit and feedback processes as a basis for planning improvement interventions).
- Organisational learning: this occurs when improvement processes result in changes to policies and procedures, such as changes to clinical protocols, client follow-up and recall procedures, adjustment in staff roles or community engagement strategies.
- Process re-engineering: this category covers changes or investments that affect organisational processes. These may be initiated within a PHC practice or service, or result from external or partnered investment (for example, the upgrade of a client information system or the introduction of a system-wide electronic health record).
- Evidence-based practice and management: improvements are classified in this category when approaches and practices are adjusted to reflect up-to-date health, management and systems research, clinical guidelines and the real-world knowledge and experience of staff, clients and communities.
An Indigenous context
Key features of CQI approaches make them well suited to Indigenous healthcare settings. The participatory approach and client focus of CQI, and the combination of scientific and humanistic professional values,19 align with the principles and values expressed in ethics guidelines for Aboriginal and Torres Strait Islander and other health research with First Nations peoples.20 Ethics guidelines emphasise the need for Indigenous health research to tackle underlying causes of poor health (for example, social and economic conditions), to build capacity (including community capacity to use data), and to improve outcomes. These concepts are central to CQI. Strengths-based approaches and a culture of self-evaluation that affirm the capabilities within Indigenous communities are also central. In addition, CQI provides a structure to refine and reinvigorate programs to promote sustainability.21
Strengths-based approaches that affirm the capabilities within Indigenous communities are central.
Factors that lead to the successful use of CQI in Aboriginal and Torres Strait Islander settings reflect those in other settings, but high-improving Aboriginal and Torres Strait Islander health services also have unique features. A multi-site study found services that showed a high level of improvement were embedded in the cultural and historical context of their communities. Staff in these health services understood how history (for example, cultural knowledge, colonisation) had shaped ways of seeing, being and doing, and how to act and communicate in culturally appropriate and respectful ways. Trusting, respectful and caring relationships were established between the clients and health service staff, who had a deep knowledge of their communities and PHC. There was cross-cultural learning for CQI, and improvement strategies tended to be driven by the community.22 Our CQI research in Aboriginal and Torres Strait Islander PHC has also shown that Indigenous staff in these contexts are crucial to improving the delivery of evidence-based care,23 including access to culturally safe and continuous care and informing and implementing CQI initiatives.24
Health equity
Health equity is a key principle of PHC. Inequalities in health and life expectancy between countries, and between population groups within countries and communities (for example, ethnic groups, socio-economic groups), draw attention to the need to improve PHC for groups with poorer health outcomes. Recent health frameworks targeting low- and middle-income countries have focused on improving processes of PHC delivery and strengthening the systems that provide client- and community-centred care.25 This is the core business of CQI.
The links between CQI and equitable health care are indisputable.
Quality improvement leaders have claimed that for care to be considered high quality, it must be equitable, and conversely, there cannot be health equity without high-quality care.26 The links between CQI and equitable health care are indisputable. The natural fit between CQI and efforts to improve health equity is evident in several ways:
- Equity is one of the seven domains of quality in health care (effective, safe, people-centred, timely, equitable, integrated and efficient).
- Health disparities are a marker of poor health system performance – CQI aims to strengthen care systems and processes to reduce variation in care delivery and improve the overall quality of care.
- The type of data collected for CQI (for example, demographic, service delivery and clinical indicators) is suitable for measuring health disparities. Data can show which groups are missing out on services or experiencing poorer health outcomes within a service population.
- CQI processes enable PHC services and teams to identify evidence-based priorities for improvement, and to design strategies targeting groups with greater needs.
- Use of CQI tools over consecutive CQI cycles can show progress in achieving equitable service delivery or health outcomes over time.
A system-wide approach to CQI enables system improvements to target issues associated with inequity, such as access to services by under-served populations (for example, people living in rural and remote areas), diseases of poverty (for example, tuberculosis and rheumatic heart disease) and improving the health of particular groups within populations (for example, refugees, Indigenous peoples, people living with disabilities). There is evidence that a system-wide approach to CQI can lead to large-scale improvements in care.27 In Australia, sustained use of CQI in Indigenous community settings has improved the delivery of PHC in many Aboriginal and Torres Strait Islander communities, as later chapters detail. There is a long way to go to close the gap in health equity for Aboriginal and Torres Strait Islander Australians, but CQI is an important part of the process.
CQI data can show variation in standards of care.
CQI data can show variation in standards of care. Variation is a measure of equity in care delivery: it shows the range in the quality of care delivered to clients. When CQI data from more than 270 PHC centres serving Aboriginal and Torres Strait Islander Australians were aggregated at a national level, it was evident that delivery of important items of care (for example, follow-up of clients with abnormal pathology results) varied widely between health centres. Trend data showed that the variation between health centre performance persisted over several audit cycles, and also that repeated CQI cycles decreased variation over time. Such evidence can help policymakers and managers to improve systems and allocate resources for more equitable service delivery.
Comprehensive PHC
As highlighted earlier, adapting conventional CQI approaches to PHC can be challenging. The comprehensive nature of high-quality PHC is a significant part of the challenge: the broad scope and complexity of care, the need to take account of the many influences on people’s health across the life course and to respond to individual, family and community health needs. Comprehensive care needs a comprehensive approach to identify and solve problems of quality across the scope of best practice.
Comprehensive care needs a comprehensive approach to identify and solve problems of quality across the scope of best practice.
Despite the use of systems thinking in quality improvement, CQI processes used do not intrinsically take a big-picture approach. CQI processes generally aim to improve performance in specific areas of clinical care (for example, cardiovascular health) and may focus on improving specific indicators for a client cohort (for example, blood pressure control). These areas of focus are likely to be defined by data reporting requirements, such as clinical and service delivery data collected for reporting against key performance indicators. There is a risk that implementing CQI processes in this way can reinforce “siloed” care, missing opportunities for synergy when making changes to care systems or missing opportunities to develop new indicators that are important to clients.
Evidence also shows that improvement of healthcare performance alone is not enough to improve health outcomes. The relative contribution of health care to health outcomes is estimated to account for only between 10 and 20 per cent of gain,28 which illustrates the importance of considering social, cultural and environmental circumstances when planning improvement interventions.
A comprehensive systems approach to CQI can enable PHC services to make evidence-based, locally responsive improvement decisions. To work in this way, CQI processes need to link with, and integrate, various stakeholders, influences and processes. McCalman, Bailie and colleagues have developed a framework to guide this approach.29 The framework depicts the integration of CQI efforts in two dimensions: vertically across the health system and horizontally across sectors (Figure 3.1). Vertical integration applies CQI processes across all levels of health systems, from community engagement and client care through to various levels of policy. Horizontal integration extends CQI from clinical guideline adherence at PHC service sites through to linkages and advocacy for the social and cultural determinants of health. In the context of Aboriginal and Torres Strait islander PHC, these determinants might include connections to land and spirituality, family and culture, housing, education, employment, criminal justice, and other sectors that affect health. Equally central to a service’s CQI approach are engaged service users, trained and supportive staff, strong management structures, systems and a culture of CQI, and resourcing and cost-effectiveness. Examples of the framework in action are provided in Chapter 20.
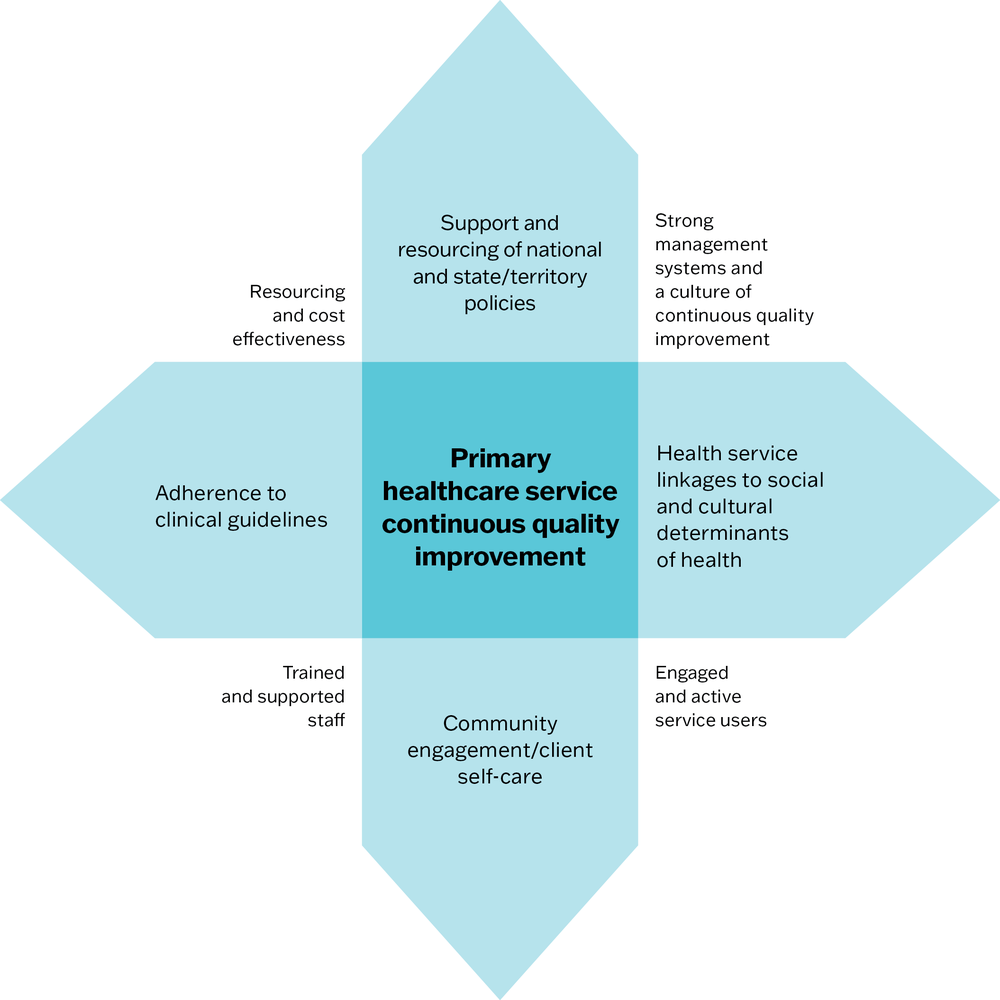
Figure 3.1 The vertical and horizontal enhancement of continuous quality improvement. Source: McCalman, Bailie et al. 2018.
Evidence of impact of CQI in comprehensive PHC
There is evidence that CQI works to improve the quality of PHC. Our research network has completed many studies investigating the effect of CQI and found that sustained use of CQI has improved the delivery of recommended care across complex and diverse PHC settings. Improvements in clinical care have resulted in improvements in maternal and women’s health,30 children’s health,31 preventive health,32 social and emotional wellbeing,33 diabetes,34 sexual health35 and rheumatic heart disease care.36 CQI interventions have also had positive effects on the delivery of health promotion programs.37 Research shows that a CQI approach is feasible and promising for improving programs that focus on the social determinants of health, including food security,38 family wellbeing empowerment programs,39 manager development programs in PHC services,40 student wellbeing in school settings41 and child protection processes.42 While the effects of implementing CQI in clinical PHC appear to be relatively under-researched internationally, examples of research in other settings include improvement in diabetes care,43 reduced hospital admissions among people with chronic conditions and among older clients44 and improved PHC team functioning.45
There is evidence that CQI works to improve the quality of PHC.
Audit and Best Practice for Chronic Disease program
The Audit and Best Practice for Chronic Disease (ABCD) research program developed and supported quality improvement tools and processes in PHC centres across Australia, with a focus on comprehensive PHC and services that serve predominantly Aboriginal and Torres Strait Islander populations. The tools are described in Part II. In Part III of this book, we summarise the history of the program and how PHC teams have used the clinical CQI tools and processes developed through this research. The approach described is supported by a strong evidence base of over 180 studies to date (several are cited above). The evidence is stronger than for any other approach to CQI in PHC as far as we are aware.
The knowledge gained from this work in Australia has wider relevance for implementing CQI in PHC. Internationally accepted principles for the effective implementation of CQI underpin the ABCD approach and, while PHC settings, characteristics and resources differ, similar improvement challenges prevail across countries. Part IV describes the ongoing system strengthening work of the quality improvement research network to help meet these challenges.
Summary
This chapter has identified characteristics of PHC that influence the implementation of CQI and discussed how conventional approaches to CQI can be adapted for practical application in PHC. We referred to CQI research in Australian Indigenous PHC settings to argue that a comprehensive systems approach to CQI can have a positive impact on health care and health equity.
References
Allen and Clarke Consulting (2013). Evaluation of the Northern Territory Continuous Quality Improvement Investment Strategy: Final report. Canberra: Department of Health.
Bailie, J., A. Laycock, V. Matthews, D. Peiris and R. Bailie (2019). Emerging evidence of the value of health assessments for Aboriginal and Torres Strait Islander people in the primary healthcare setting. Australian Journal of Primary Health 25(1): 1–5. DOI: 10.1071/PY18088.
Bailie, R., V. Matthews, S. Larkins, S. Thompson, P. Burgess, T. Weeramanthri et al. (2017). Impact of policy support on uptake of evidence-based continuous quality improvement activities and the quality of care for Indigenous Australians: a comparative case study. BMJ Open 7. DOI: 10.1136/bmjopen-2017-016626.
Bailie, R.S., D. Si, L. O’Donoghue and M. Dowden (2007). Indigenous health: effective and sustainable health services through continuous quality improvement. Medical Journal of Australia 186(10): 525–7.
Best, A., T. Greenhalgh, S. Lewis, J. Saul, S. Carroll and J. Bitz (2012). Large-system transformation in health care: a realist review. Milbank Quarterly 90(3): 421–56. DOI: 10.1111/j.1468-0009.2012.00670.x.
Booske, B., J. Athens, D. Kindig, H. Park and P. Remington (2010). Different perspectives for assigning weights to determinants of health. County Health Rankings Working Paper. Madison, WI: University of Wisconsin, Population Health Institute.
Brimblecombe, J., R. Bailie, C. van Den Boogaard, B. Wood, S. Liberato, M. Ferguson et al. (2017). Feasibility of a novel participatory multi-sector continuous improvement approach to enhance food security in remote Indigenous Australian communities. SSM – Population Health 3(C): 566–76. DOI: 10.1016/j.ssmph.2017.06.002.
de Silva, D. (2014). Improvement collaboratives in health care. Evidence scan No. 21. London: Health Foundation.
de Witt, A., F. Cunningham, R. Bailie, N. Percival, J. Adams and P. Valery (2018). “It’s just presence”, the contributions of Aboriginal and Torres Strait Islander health professionals in cancer care in Queensland. Frontiers in Public Health 6: 344. DOI: 10.3389/fpubh.2018.00344.
Diaz, A., B. Vo, P.D. Baade, V. Matthews, B. Nattabi, J. Bailie et al. (2019). Service level factors associated with cervical screening in Aboriginal and Torres Strait Islander primary health care centres in Australia. International Journal of Environmental Research and Public Health 16(19): 3630. DOI: 10.3390/ijerph16193630.
Dzau, V.J., K. Mate and M. O’Kane (2022). Equity and quality—improving health care delivery requires both. JAMA 327(6): 519–20. DOI: 10.1001/jama.2022.0283. DOI: 10.1001/jama.2022.0283
Edmond, K., S. Tung, K. McAuley, N. Strobel and D. McAullay (2018). Improving developmental care in primary practice for disadvantaged children. Archives of Disease in Childhood 104: 372–80. DOI: 10.1136/archdischild-2018-315164.
Gachupin, F.C., B. Lameman and F. Molina (2019). Guideline for researchers: a guide to establishing effective mutually-beneficial research partnerships with American Indian tribes, families and individuals. Tucson, AZ: University of Arizona, Department of Family and Community Medicine, College of Medicine.
Gardner, K.L., M. Dowden, S. Togni and R. Bailie (2010). Understanding uptake of continuous quality improvement in Indigenous primary health care: lessons from a multi-site case study of the Audit and Best Practice for Chronic Disease project. Implementation Science 5: 21. DOI: 10.1186/1748-5908-5-21.
Gibson-Helm, M., A. Rumbold, H. Teede, S. Ranasinha, R. Bailie and J. Boyle (2016). Improving the provision of pregnancy care for Aboriginal and Torres Strait Islander women: a continuous quality improvement initiative. BMC Pregnancy and Childbirth 16: 118. DOI: 10.1186/s12884-016-0892-1.
Gibson-Helm, M., H. Teede, A. Rumbold, S. Ranasinha, R. Bailie and J. Boyle (2015). Continuous quality improvement and metabolic screening during pregnancy at primary health centres attended by Aboriginal and Torres Strait Islander women. Medical Journal of Australia 203(9): e1–7. DOI: 10.5694/mja14.01660.
Greenhalgh, T., G. Robert, F. Macfarlane, P. Bate and O. Kyriakidou (2004). Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Quarterly 82(4): 581–629. DOI: 10.1111/j.0887-378X.2004.00325.x.
Guidelines International Network (2024). GIN international guideline library. https://g-i-n.net/international-guidelines-library.
Gunaratnam, P., G. Schierhout, J. Brands, L. Maher, R. Bailie, J. Ward et al. (2019). Qualitative perspectives on the sustainability of sexual health continuous quality improvement in clinics serving remote Aboriginal communities in Australia. BMJ Open 9(5): e026679. DOI: 10.1136/bmjopen-2018-026679.
Harris, S., M. Green, J. Brown, S. Roberts, G. Russell, M. Fournie et al. (2015). Impact of a quality improvement program on primary healthcare in Canada: a mixed-method evaluation. Health Policy 119(4): 405–16. DOI: 10.1016/j.healthpol.2014.10.019.
Kaplan, H., L. Provost, C. Froehle and P. Margolis (2012). The model for understanding success in quality (MUSIQ): building a theory of context in healthcare quality improvement. BMJ Quality and Safety 21: 13–20. DOI: 10.1136/bmjqs-2011-000010.
Langham, E., J. McCalman, V. Matthews, R.G. Bainbridge, B. Nattabi, I. Kinchin et al. (2017). Social and emotional wellbeing screening for Aboriginal and Torres Strait Islanders within primary health care: a series of missed opportunities? Frontiers in Public Health 5: 159. DOI: 10.3389/fpubh.2017.00159.
Larkins, S., K. Carlisle, N. Turner, J. Taylor, K. Copley, S. Cooney et al. (2019). “At the grass roots level it’s about sitting down and talking”: exploring quality improvement through case studies with high-improving Aboriginal and Torres Strait Islander primary healthcare services. BMJ Open 9(5): e027568DOI: 10.1136/bmjopen-2018-027568.
Lindenauer, P.K. (2008). Effects of quality improvement collaboratives. BMJ 336(7659): 1448–9. DOI: 10.1136/bmj.a216.
MacIsaac, M.B., M. Tam, K. McLean, M. Morgan, F. Jones and M. Saito (2019). We need to talk about quality in general practice. Medical Journal of Australia(28), Insight+ 28, 22 July 2019. https://insightplus.mja.com.au/2019/28/.
Matthews, V., G. Schierhout, J. McBroom, C. Connors, C. Kennedy, R. Kwedza et al. (2014). Duration of participation in continuous quality improvement: a key factor explaining improved delivery of type 2 diabetes services. BMC Health Services Research 14(1): 578. DOI: 10.1186/s12913-014-0578-1.
McAullay, D., K. McAuley, R. Bailie, V. Mathews, P. Jacoby, K. Gardner et al. (2018). Sustained participation in annual continuous quality improvement activities improves quality of care for Aboriginal and Torres Strait Islander children. Journal of Paediatrics and Child Health 54(2): 132–40. DOI: 10.1111/jpc.13673.
McCalman, J., R. Bailie, R. Bainbridge, K. McPhail-Bell, N. Percival, D. Askew et al. (2018). Continuous quality improvement and comprehensive primary health care: a systems framework to improve service quality and health outcomes. Frontiers in Public Health 6: 76. DOI: 10.3389/fpubh.2018.00076.
McCalman, J., R. Bainbridge, C. Brown, K. Tsey and A. Clarke (2018). The Aboriginal Australian Family Wellbeing Program: a historical analysis of the conditions that enabled its spread. Frontiers in Public Health 6. DOI: 10.3389/fpubh.2018.00026.
McCalman, J., R. Bainbridge, S. Russo, K. Rutherford, K. Tsey, M. Wenitong et al. (2016). Psycho-social resilience, vulnerability and suicide prevention: impact evaluation of a mentoring approach to modify suicide risk for remote Indigenous Australian students at boarding school. Report. BMC Public Health 16: 98. DOI: 10.1186/s12889-016-2762-1.
McGinnis, J., P. Williams-Russo and J. Knickman (2002). The case for more active policy attention to health promotion. Health Affairs 21(2): 78–93. DOI: 10.1377/ hlthaff.21.2.78.
McLaughlin, C. and A. Kaluzny, eds (1994). Continuous quality improvement in health care: theory, implementation, and applications. Gaithersburg, MD: Aspen Publications.
National Health and Medical Research Council (2018). Ethical conduct in research with Aboriginal and Torres Strait Islander Peoples and communities: guidelines for researchers and stakeholders. Canberra: Commonwealth of Australia.
Nattabi, B., V. Matthews, J. Bailie, A. Rumbold, D. Scrimgeour, J. Ward et al. (2017). Wide variation in sexually transmitted infection testing and counselling at Aboriginal primary health care centres in Australia: analysis of longitudinal continuous quality improvement data. BMC Infectious Diseases 17: 148. DOI: 10.1186/s12879-017-2241-z.
Onnis, L.-A., M. Hakendorf, M. Diamond and K. Tsey (2019). CQI approaches for evaluating management development programs: a case study with health service managers from geographically remote settings. Evaluation and Program Planning 74: 91–101. DOI: https://doi.org/10.1016/j.evalprogplan.2019.03.003.
Percival, N., L. O’Donoghue, V. Lin, K. Tsey and R. Bailie (2016). Improving health promotion using quality improvement techniques in Australian Indigenous primary health care. Front Public Health 4: 53. DOI: 10.3389/fpubh.2016.00053.
Powell, A., R. Rushmer and H. Davies (2009). A systematic narrative review of quality improvement models in health care. Edinburgh, UK: NHS Quality Improvement Scotland.
Read, C., A. Mitchell, J. de Dassel, C. Scrine, D. Hendrickx, R. Bailie et al. (2018). Qualitative evaluation of a complex intervention to improve rheumatic heart disease secondary prophylaxis. Journal of the American Heart Association 7(14). DOI: 10.1161/JAHA.118.009376.
Redman-MacLaren, M., N.N. Turner, J. Taylor, A. Laycock, K. Vine, Q. Thompson et al. (2021). Respect is central: a critical review of implementation frameworks for continuous quality improvement in Aboriginal and Torres Strait Islander primary health care services. Frontiers in Public Health
16: 9. DOI: 10.3389/fpubh.2021.630611.
Riley, W., H. Parsons, G. Duffy, J. Moran and B. Henry (2010). Realizing transformational change through quality improvement in public health. Journal of Public Health Management Practice 16(1): 72–8. DOI: 10.1097/PHH.0b013e3181c2c7e0.
Ryerson University Research Ethics Board (2017). Guidelines for research involving Indigenous peoples in Canada. Toronto, Canada: Toronto Metropolitan University.
Schierhout, G., J. Hains, D. Si, C. Kennedy, R. Cox, R. Kwedza et al. (2013). Evaluating the effectiveness of a multifaceted, multilevel continuous quality improvement program in primary health care: developing a realist theory of change. Implementation Science 8: 119. DOI: 10.1186/1748-5908-8-119.
Schierhout, G., V. Matthews, C. Connors, S. Thompson, R. Kwedza, C. Kennedy et al. (2016). Improvement in delivery of type 2 diabetes services differs by mode of care: a retrospective longitudinal analysis in the Aboriginal and Torres Strait Islander primary health care setting. BMC Health Services Research 16: 560. DOI: 10.1186/s12913-016-1812-9.
Schouten, L., M. Hulscher, J. van Everdingen, R. Huijsman and R. Grol (2008). Evidence for the impact of quality improvement collaboratives: systematic review. BMJ 336(7659): 1491–4. DOI: 10.1136/bmj.39570.749884.BE.
Shojania, K. and J. Grimshaw (2005). Evidence-based quality improvement: the state of the science. Health Affairs 24(1): 138–50. DOI: 10.1377/hlthaff.24.1.138.
Smith, G., R. Kirkham, C. Gunabarra, V. Bokmakarray and C.P. Burgess (2018). “We can work together, talk together”: an Aboriginal Health Care Home. Australian Health Review 43(5): 486–91. DOI: 10.1071/ah18107.
Sollecito, W. and J. Johnson (2019). McLaughlin and Kaluzny’s continuous quality improvement in health care. Burlington, MA: Jones & Bartlett Learning.
The Pūtaiora Writing Group (2010). Te Ara Tika. Guidelines for Māori research ethics: a framework for researchers and ethics committee members. Auckland, New Zealand: Health Research Council of New Zealand.
Tricco A., J. Antony, N. Ivers, H. Ashoor, P. Khan, E. Blondal et al. (2014). Effectiveness of quality improvement strategies for coordination of care to reduce use of health care services: a systematic review and meta-analysis. Canadian Medical Association Journal 186(15): E568–78. DOI: 10.1503/cmaj.140289.
Tricco, A., N. Ivers, J. Grimshaw, D. Moher, L. Turner, J. Galipeau et al. (2012). Effectiveness of quality improvement strategies on the management of diabetes: a systematic review and meta-analysis. Lancet 379(9833): 2252–61. DOI: 10.1016/S01406736(12)60480-2.
Turner, N., J. Taylor, S. Larkins, K. Carlisle, S. Thompson, M. Carter et al. (2019). Conceptualizing the association between community participation and CQI in Aboriginal and Torres Strait Islander PHC Services. Qualitative Health Research 29(13): 1904–15. DOI: 10.1177/1049732319843107.
Wells, S., O. Tamir, J. Gray, D. Naidoo, M. Bekhit and D. Goldmann (2018). Are quality improvement collaboratives effective? A systematic review. BMJ Quality and Safety 27(3): 226–40. DOI: 10.1136/bmjqs-2017-006926.
Wensing, M., H. Wollersheim and R. Grol (2006). Organizational interventions to implement improvements in patient care: a structured review of reviews. Implementation Science 1: 2. DOI: 10.1186/1748-5908-1-2.
Wise, M., S. Angus, E. Harris and S. Parker (2013). National appraisal of continuous quality improvement initiatives in Aboriginal and Torres Strait Islander primary health care: final report. Melbourne: Lowitja Institute.
World Health Organization (2023). WHO guidelines. https://www.who.int/publications/guidelines/en/.
World Health Organization (2015). Primary Health Care Performance Initiative. https://improvingphc.org/.
Zuchowski, I., D. Miles, C. Woods and K. Tsey (2017). Continuous quality improvement processes in child protection: a systematic literature review. Research on Social Work Practice 29(4). DOI: 10.1177/1049731517743337.
1 McLaughlin and Kaluzny 1994.
2 Sollecito and Johnson 2019.
3 Sollecito and Johnson 2019, 18.
4 National Health and Medical Research Council 2018; World Health Organization 2023.
5 de Silva 2014; Lindenauer 2008; Schouten, Hulscher et al. 2008; Wells, Tamir et al. 2018.
6 Gardner, Dowden et al. 2010; Wise, Angus et al. 2013.
7 Best, Greenhalgh et al. 2012; Powell, Rushmer and Davies 2009; Wise, Angus et al. 2013.
8 Shojania and Grimshaw 2005; Wensing, Wollersheim and Grol 2006.
9 Allen and Clarke Consulting 2013; Wise, Angus et al. 2013.
10 Schierhout, Hains et al. 2013.
11 MacIsaac, Tam et al. 2019.
12 Bailie, Si et al. 2007.
13 Greenhalgh, Robert et al. 2004; Kaplan, Provost et al. 2012.
14 Gardner, Dowden et al. 2010; Larkins, Carlisle et al. 2019; Turner, Taylor et al. 2019; Wise, Angus et al. 2013.
15 Riley, Parsons et al. 2010; Schierhout, Hains et al. 2013.
16 Bailie, Matthews et al. 2017.
17 Shojania and Grimshaw 2005; Wensing, Wollersheim and Grol 2006.
18 Sollecito and Johnson 2019.
19 Wensing, Wollersheim and Grol 2006.
20 For example, Gachupin, Lameman and Molina 2019; National Health and Medical Research Council 2018; Ryerson University Research Ethics Board 2017; The Pūtaiora Writing Group 2010.
21 Bailie, Si et al. 2007.
22 Larkins, Carlisle et al. 2019; Redman-MacLaren, Turner et al. 2021; Turner, Taylor et al. 2019.
23 Bailie, Laycock et al. 2019; de Witt, Cunningham et al. 2018.
24 Larkins, Carlisle et al. 2019; Smith, Kirkham et al. 2018; Turner, Taylor et al. 2019.
25 World Health Organization 2015.
26 Dzau, Mate and O’Kane 2022.
27 Bailie, Matthews et al. 2017; Tricco, Ivers et al. 2012.
28 Booske, Athens et al. 2010; McGinnis, Williams-Russo and Knickman 2002.
29 McCalman, Bailie et al. 2018.
30 Diaz, Vo et al. 2019; Gibson-Helm, Rumbold et al. 2016; Gibson-Helm, Teede et al. 2015.
31 Edmond, Tung et al. 2018; McAullay, McAuley et al. 2018.
32 Bailie, Laycock et al. 2019.
33 Langham, McCalman et al. 2017.
34 Matthews, Schierhout et al. 2014; Schierhout, Matthews et al. 2016.
35 Gunaratnam, Schierhout et al. 2019; Nattabi, Matthews et al. 2017.
36 Read, Mitchell et al. 2018.
37 Percival, O’Donoghue et al. 2016.
38 Brimblecombe, Bailie et al. 2017.
39 McCalman, Bainbridge et al. 2018.
40 Onnis, Hakendorf et al. 2019.
41 McCalman, Bainbridge et al. 2016.
42 Zuchowski, Miles et al. 2017.
43 Tricco, Ivers et al. 2012.
44 Tricco, Antony et al. 2014.
45 Harris, Green et al. 2015.