2
Continuous quality improvement
What is quality in health care?
The World Health Organization (WHO) defines quality in health care as “the extent to which health care services provided to individuals and patient populations improve desired health outcomes. In order to achieve this, health care must be safe, effective, timely, efficient, equitable and people centred.”1 Each of these terms is worth examining:
- effective – providing evidence-based healthcare services to those who need them
- safe – minimising risk and avoiding harm, which includes avoiding preventable injuries and reducing medical errors, and involves safe care systems and safe practices
- people-centred – providing care that responds to the preferences, needs and values of individuals and communities. Clients should be engaged in care decisions.
Realising the benefits of high-quality health care requires services that display the following characteristics:
- timely – reducing wait times and delays in providing and receiving health care
- equitable – providing care that does not differ in quality according to individual characteristics such as gender, sexuality, race, ethnicity, geographical location or socio-economic status
- integrated – making available the full range of health services, which work together to provide “joined up” care throughout the life course
- efficient – maximising resource use and avoiding waste of supplies, space, capital, time and opportunities.2
Other concepts closely linked to quality in health care are access, continuity of care and value.
Access and quality
Access to primary health care (PHC) is central to receiving care that is timely, efficient, equitable and people-centred. Access can be defined as the opportunity to identify healthcare needs, to seek healthcare services, to reach, to obtain or use healthcare services and to have service needs met.3
Providing access to PHC services continues to be a key issue in many low- and middle-income countries. Overcoming barriers to accessing care is also critical for improving health equity in wealthy countries where race, ethnicity, socio-economic status, disability status, age, gender, sexual orientation, gender identity or geographic location can influence access to care and social services. Indigenous peoples in colonised countries,4 resettled refugees5 and people experiencing homelessness6 are among groups at risk of inequitable access to services.
Levesque and colleagues identified five dimensions of healthcare accessibility: approachability; acceptability; availability or accommodation; affordability; and appropriateness.7 We found these dimensions to be useful criteria for analysing the complex range of factors influencing Aboriginal and Torres Strait Islander Australians’ access to healthcare services.8 Accessibility is both a precursor to providing high-quality health care and one measure of PHC quality.
Continuity of care and quality
Continuity of care is the ability to provide uninterrupted care across programs, practitioners and levels of service over time. Care continuity is a core value and major focus of both PHC and general practice, and is a crucial element of high-quality PHC. It is associated with greater client satisfaction, lower mortality, fewer hospital admissions and improved health and system outcomes.9 Continuity of care is of growing importance as populations increasingly live with chronic and complex illnesses, and other health and social challenges (for example, food and housing insecurity, warming climates).
There are many aspects of care continuity, such as ongoing client–practitioner relationships, ongoing management of chronic illness or disability, teamwork for care coordination, cross-boundary care (for example, between PHC, specialist and hospital services), and transfer of information that follows the client.10
Continuity of care is a crucial element of high-quality PHC.
PHC models in some countries are being reformed to promote continuity of care. These include the Patient-centred Medical Home (United States of America), Primary Care Home (United Kingdom) and Health Care Homes (Australia – see below).
Value and quality
The concepts of value and quality are closely connected in health care, with policy debate around value-based care gaining momentum.11 The idea of value-based health care is not new. Promoting better health at lower cost is an identified benefit of using a systems approach, and definitions of quality care include efficiency and sustainability concepts. But, as the cost of health care is rising faster than economies are growing, there is increasing emphasis on the need for health systems to spend their resources in a cost-effective way. Value-related issues differ between low- and middle-income countries and high-income countries. In the former, improving access to essential PHC services is a “high-value” investment as countries aim for universal healthcare coverage. High-income countries aiming for more value-based models are likely to prioritise system integration and the strengthening of existing healthcare infrastructure and operations.
Value and quality are closely connected in health care.
Four types of value are reflected in current thinking around a value-based approach: personal value (appropriate care to achieve client goals); technical value (best possible outcomes with available resources); allocative value (equitable resource distribution across population groups); and societal value (contribution to social participation and connectedness).12
The World Economic Forum’s definition of value-based health care explicitly focuses on the value delivered to the client: “the health outcomes that matter to patients relative to the resources or costs required”.13 By focusing on health outcomes instead of the volume of services delivered, value-based care systems help providers to manage cost increases, make the best use of finite resources and deliver improved care. Value is measured with a dual focus on improving accountability and improving quality.
Domains of quality are often measured in terms of meeting expected standards: for example, with indicators that measure clinical outcomes, care processes or care structures. Indicators may or may not measure client perceptions of quality care. But measures of value-based care do include client perspectives of value while factoring in the cost (to providers, clients and their families or carers) of delivering care.14 This development supports the increasing use of quality improvement tools that measure care outcomes and experiences from a client viewpoint (see Chapter 5). Importantly, the change in approach stimulates discussion around who decides what is valuable and valued in health care, and provides greater scope for consumer-led measures of quality and consumer involvement in service design. For example, communities may place high value on the availability of cultural healing practices through the PHC clinic, or in-home visits for new mothers, elderly or disabled clients. Value-based care aligns with the way we define PHC and “quality” in several ways: it is client-centred; recognises complexity; and depends on integrated work by providers. Value-based care allows for different perceptions of value (for example, cultural safety) and aims for equity and efficiency in care.
In Australia, projects trialling the use of client-centred outcomes to improve the value of care include the staged rollout of the Health Care Homes model. The model promotes continuity of care and provides PHC practices with monthly bundled payments to care for registered clients with chronic conditions.15 Measures being used to evaluate the model include use of services (including potentially preventable hospitalisations), client and service experiences, and the cost of care for the government, providers and clients.
What is continuous quality improvement?
Quality improvement in health care is an interdisciplinary and participatory process designed to raise the standards of care to maintain, restore and improve outcomes for individuals and populations. Continuous quality improvement (CQI) is one method of quality improvement, in which data are systematically collected and used in cyclical learning processes, such as the plan-do-study-act model.16 We favour CQI over other approaches because of its focus on continuous learning and improvement. Other terms used under the broad banner of quality management are “quality assurance”, a process focused on determining standards, guidelines and procedures to prevent risks to quality, and “quality control”, which focuses more on testing the quality of a service or product.
CQI is about ongoing learning and improvement.
Batalden and Davidoff defined CQI as “the combined and unceasing efforts of everyone—healthcare professionals, patients and their families, researchers, payers, planners and educators—to make the changes that will lead to better patient outcomes (health), better system performance (care) and better professional development (learning)”.17 This definition is based on a conviction that health care would be able to realise its potential if making positive change was part of everyone’s job, in all parts of the health system. This accurately defines CQI in a PHC context, where many stakeholders need to be involved in improving and, in some contexts, transforming care. The definition is also consistent with the concept of a learning health system, where evidence and experience are continually brought together and applied to deliver higher quality, safer, more efficient care.18
Another widely accepted definition comes from McLaughlin and Kaluzny, who defined CQI as “a structured organisational process for involving personnel in planning and executing a continuous flow of improvements to provide quality health care that meets or exceeds expectations”.19 CQI is therefore both an approach and a process to improve the quality of care. A common concept across these definitions is continuous, collective effort to improve care systems and health outcomes.
Features of CQI
The following features are guiding principles for implementing or strengthening CQI.20
Data-driven continuous cycles of learning and improvement
In general, CQI facilitates ongoing improvement by using objective data to analyse and improve processes. It involves an ongoing cycle of gathering data on how well organisational systems are functioning and developing and implementing improvements. A 2014 study found consensus among quality improvement researchers and practitioners that all CQI methods involve these elements:
- systematic data-guided activities
- design for local conditions
- iterative development and testing.21
An essential starting point is the systematic and objective assessment of performance, and of the systems that support good performance. Good-quality information is needed, so that goals can be set, and strategies developed for improving care. Changes are made and the effects are monitored, leading to further change. CQI assumes that the effort to improve processes is never-ending, and that organisational and individual learning is ongoing.
Until recently, CQI processes and data had a strong focus on elements of clinical care for particular conditions or population groups. There is increasing focus on using CQI to address the social, cultural, structural and environmental determinants of health.
Small, incremental improvements
CQI aims for small changes that are realistic and achievable. Incremental changes made over successive CQI cycles are more likely to be sustainable than major, one-off changes. It takes time for small, incremental improvements in care quality to be reflected in data, which reinforces the importance of implementing continuous cycles of improvement.
CQI involves ongoing data-driven cycles of learning and improvement, aiming for small incremental changes that are realistic and achievable.
Systems focus
CQI places emphasis on the efficient and effective functioning of organisational systems, and how system factors influence quality. CQI processes assume that people engaged within systems are well placed to identify system deficiencies and options for improvement. The focus of CQI to date has largely been on care teams and processes (sometimes called “clinical micro-systems”), but increasing attention is being paid to the way higher level systems influence the effective functioning of clinical micro-systems. This development is expanding the focus of CQI to include the way “meso-level” systems (those at organisational or community level) and “macro-level” systems (health and other large-scale systems) influence quality and value in health care. CQI can be used to strengthen policy, managerial and professional processes for delivering high-quality care: that is, the entire “production system”.
Use of systems thinking
As highlighted in Chapter 1, health systems are complex, typically including many providers, organisations of varying size, and providing care for diverse health conditions, clients and communities. Systems thinking is a way of thinking about systems as holistic, dynamic and interconnected. The use of systems thinking in CQI helps in analysing and understanding the complex interactions that occur between different parts of the healthcare system and predicting the effects of system adjustments (for example, on integration of care, on client experiences and outcomes).
CQI uses systems thinking: a way of thinking about systems as holistic, dynamic and interconnected.
Client or “customer” focus
CQI focuses on the evidence-based processes and outcomes that matter to users and potential users of the service (for example, people who are unable to access PHC), including clients and families or carers, organisations that refer clients or receive referrals from the PHC service, funders, and those who interact with the service in other ways.
Data is used for learning and decision-making, not blame
The primary purpose of data and measurement in CQI is learning. CQI data should not be used for performance monitoring, reward or punishment. Use of data for such purposes may detract from the quality of the data and its use and potential for driving improvement.
Decentralised and participative
CQI places ownership of improvement processes in the hands of the people who implement these processes. This does not absolve management of fundamental responsibility. Where there are weaknesses in the service system, management and policymakers should bear responsibility for system improvement. But CQI encourages those directly involved in care processes to be part of solutions for overcoming system weaknesses.
Values the contribution of everyone who is involved in care
CQI increases the dignity of the people involved because it recognises the important role of each member of the team and involves them as partners and leaders in the design and implementation of an improvement process. It respects the knowledge and experience that each person brings to the process and assumes that all are intrinsically motivated to do good work. Organisations involved in CQI often experience improvements in morale and higher levels of staff engagement. CQI provides evidence of the quality of work being done, and justification for staff to take pride in their work.
Leadership for improvement
There is substantial CQI experience in the manufacturing, business and health sectors to show that improvement in performance is strongly linked to leadership and people management. It is not a top-down approach, but it requires commitment and leadership for improvement at all levels of an organisation to create a culture that drives out fear and blame, seeks truth, respects and inspires people, and continually strives for improvement.
Responsive to context
CQI is sensitive to context. Locally relevant data are analysed, and changes planned and implemented using contextual knowledge – which is why participatory processes are important. Improvement initiatives that are not sufficiently sensitive and responsive to context are bound to fall short of goals.
CQI is sensitive and responsive to context.
A strategic approach
As described above, CQI needs to be part of a strategic approach to improvement, reflected in organisational goals, principles and strategic plans.
Origins and development
CQI has its origins in the total quality management (TQM) philosophy and techniques developed in the manufacturing industries in the early 20th century. Core concepts have been adapted for use in health care. Table 2.1 tracks major developments and pioneers in the shift from a total quality management approach to a CQI approach in health care.
|
1930s |
|
|
1950s |
|
|
1960s |
|
|
1970s |
|
|
1980s |
|
|
1990s |
|
|
2000s onwards |
|
|
Source: Sollecito and Johnson 2019. | |
Table 2.1 Key developments in CQI in health care.
The shift from TQM to CQI reflected a major change in approach to health services management. Many organisations continue to adapt CQI to their healthcare contexts, and CQI processes have been integrated into clinical governance in many settings. The scope for adapting CQI is part of its intuitive appeal, but it does present challenges for cross-organisational comparisons and learning, especially in PHC. We discuss some of these challenges and solutions in the following chapters.
Advancements in health care have enabled CQI uptake and implementation. These include the availability of evidence-based practice guidelines against which to measure health service performance, and the development of information technology systems. Increased knowledge about the factors that affect health have helped to define care priorities and focus improvement efforts.
Advancements in CQI have seen the development of a range of tools and techniques. Examples are tools for collecting and analysing data, for assessing systems and teamwork, and for measuring client experiences. There are techniques for identifying causes of variation in quality, for setting goals, planning improvements, managing change and other processes. Throughout these developments, the relevance of foundational quality improvement work, such as the plan-do-study-act cycle, has endured.
Quality improvement cycles
Plan-do-study-act cycle – the scientific method
We have described data-driven ongoing cycles of improvement as a feature of CQI. The plan-do-study-act (PDSA)27 cycle is a widely used framework for this approach. PDSA cycles use a small-scale iterative approach to test changes in real work or community settings. They enable teams to make rapid assessment and provide flexibility to adjust a change according to feedback to ensure that the solutions developed are fit for purpose.28
The broad use of the PDSA cycle in health care responds to Deming’s premise that organisational management needed to undergo transformation through deliberative learning, the “system of profound knowledge”. By applying this cycle, teams can develop insights into systems, variations in care and psychology to build theory about how to achieve improvement. This theory is tested by making changes and learning from data whether the changes are improvements, and what further improvements are needed.
The plan-do-study-act cycle is widely used in CQI.
The simplicity of the PDSA cycle also contributes to its wide use. The four steps of the cycle (plan, do, study, act) provide a structure, a common language and an orderly process whereby workers can be engaged in improving organisational systems and outcomes. At the same time, it offers scope to use a variety of other tools to collect data, measure quality and drive improvement strategies.
The PDSA cycle has been used in high- and low-resource settings, in public health and traditional medical care.29 It has been used to improve the quality of comprehensive PHC, including various aspects of clinical care, health promotion and food security.30
Taylor and colleagues describe five features of any PDSA process:
- iterative cycles – lessons learnt from one cycle link and inform cycles that follow
- prediction-based test of change – the expected change should be in line with the target for improvement, as identified in the plan stage
- small-scale testing – with the expectation that changes may be scaled out as confidence grows, and that interventions will be adapting according to feedback and learning
- data – used over time to understand variation in the system and the effect of change
- documentation – to support and share learning.31
We suggest a need to modify “small-scale testing” in many PHC contexts. In a single PHC centre, it may not make sense to make a change to a specific process on a scale smaller than the whole centre. A change made across the whole centre may need to be tested for a short period of time – but long enough for the change to have a measurable effect on the target for improvement. Where a PHC service covers multiple PHC centres, the initial testing can be done in one or two centres before extending the change to other centres, based on what is learnt from the initial testing.
There are many adaptations and representations of the PDSA cycle. Figure 2.1 captures the fundamental elements.32 We expand on how to use PDSA cycles in Chapter 6.
Improvement scientists Langley and colleagues combined the PDSA cycle with three questions to develop a framework they called the “Model for Improvement”. The questions can be asked in any order.
- “What are we trying to accomplish?” This question clarifies the improvement aim.
- “How will we know that a change is an improvement?” This question guides the feedback that will be gathered.
- “What changes can we make that will result in improvement?” This question focuses the actions to be taken.33
These questions reflect the importance of careful study and reflection, described by Don Berwick as “inductive learning – the growth of knowledge through making changes and then reflecting on the consequences of those changes”.34
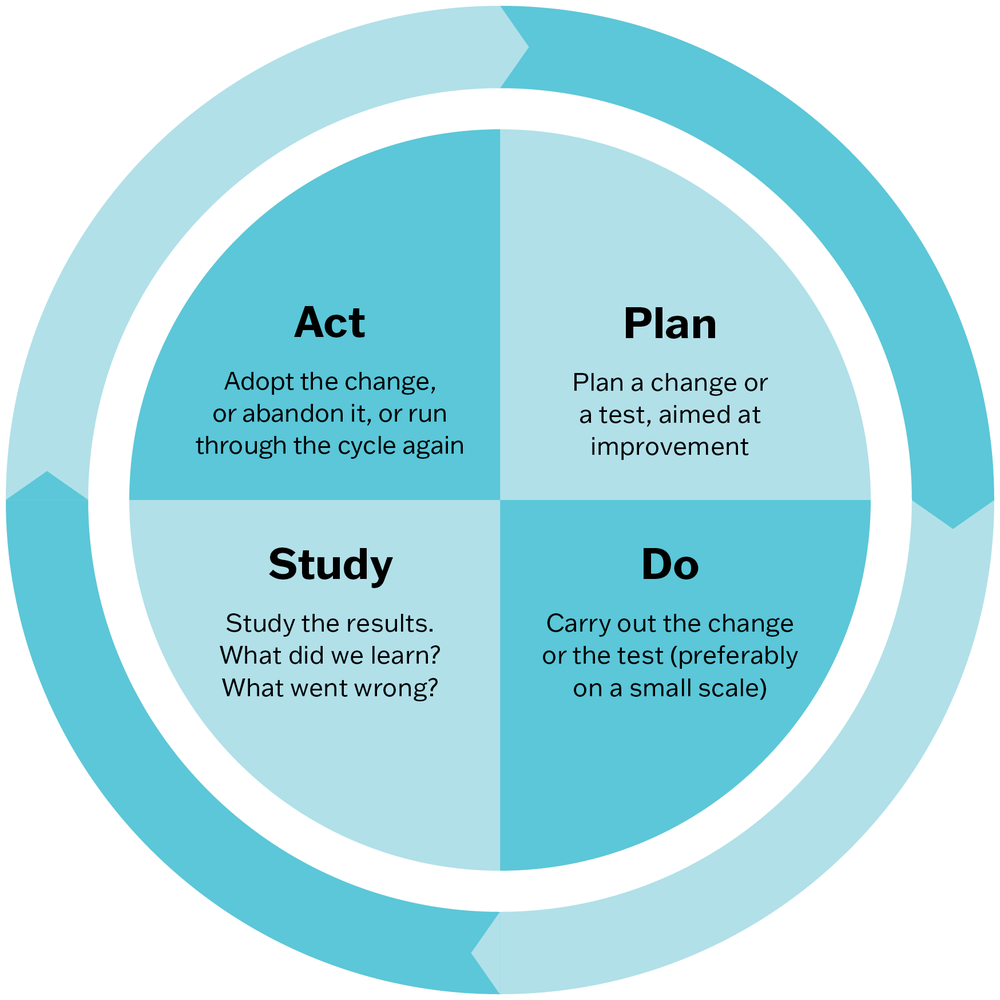
Figure 2.1 The PDSA Cycle. Adapted from: Deming, W. Edwards. foreword by Kevin Edwards Cahill, The New Economics for Industry, Government, Education, third edition, The PDSA Cycle, page 91 © 2018 Massachusetts Institute of Technology, by permission of The MIT Press.
Summary
This chapter has defined quality and CQI in health care and considered related concepts such as “access” and “value”. We have described the key features of CQI and how it evolved in health care, and summarised how CQI cycles are used to improve care. In the next chapter, we discuss how conventional approaches to CQI need to be adapted for practical application in PHC settings.
References
Agency for Healthcare Research and Quality (2019). About learning health systems. https://www.ahrq.gov/learning-health-systems/about.html.
Al-Azri M. (2008). Continuity of care and quality of care – inseparable twin. Oman Medical Journal 23(3): 147–9 PMC3282321.
Bailie, J., G. Schierhout, A. Laycock, M. Kelaher, N. Percival, L. O’Donoghue et al. (2015). Determinants of access to chronic illness care: a mixed-methods evaluation of a national multifaceted chronic disease package for Indigenous Australians. BMJ Open 5(11): e008103. DOI: 10.1136/bmjopen-2015-008103.
Bailie, R., V. Matthews, J. Brands and G. Schierhout (2013). A systems-based partnership learning model for strengthening primary healthcare. Implementation Science 8: 143. DOI: 10.1186/1748-5908-8-143.
Bailie, R.S., D. Si, L. O’Donoghue and M. Dowden (2007). Indigenous health: effective and sustainable health services through continuous quality improvement. Medical Journal of Australia 186(10): 525–7.
Batalden, P.B. and F. Davidoff (2007). What is “quality improvement” and how can it transform healthcare? Quality and Safety in Health Care 16(1): 2–3. DOI: 10.1136/qshc.2006.022046.
Berwick, D.M. (1996). A primer on leading the improvement of systems. BMJ 312 (7031): 619–22. DOI: 10.1136/bmj.312.7031.619.
Brimblecombe, J., R. Bailie, C. van Den Boogaard, B. Wood, S. Liberato, M. Ferguson et al. (2017). Feasibility of a novel participatory multi-sector continuous improvement approach to enhance food security in remote Indigenous Australian communities. SSM – Population Health 3(C): 566–76. DOI: 10.1016/j.ssmph.2017.06.002.
Coulter, A. (2017). Measuring what matters to patients. BMJ 356: j816. DOI: 10.1136/bmj.j816.
Davies, A. and L. Wood (2018). Homeless health care: meeting the challenges of providing primary care. Medical Journal of Australia 209(5): 230–4. DOI: 10.5694/mja17.01264.
Davy, C., S. Harfield, A. McArthur, Z. Munn and A. Brown (2016). Access to primary health care services for Indigenous peoples: a framework synthesis. International Journal for Equity in Health 15(1): 163. DOI: 10.1186/s12939-016-0450-5.
Deming, W.E. (2018). The new economics for industry, government, education, 3rd edn. Cambridge, MA: MIT Press.
Cahill, K.E. (2018). Foreword. In W. Edwards Deming, The New Economics for Industry, Government, Education, 3rd edition: 19. Cambridge, MA: MIT Press.
European Commission (2019). Defining value in “value-based healthcare”: report of the expert panel on effective ways of investing in health (EXPH). Luxembourg: European Union. DOI: 10.2875/872343.
Jackson, C. and L. Ball (2018). Continuity of care: vital, but how do we measure and promote it? Australian Journal of General Practice 47: 662–4. DOI: 10.31128/AJGP-05-18-4568.
Langley, G., R. Moen, K. Nolan, T. Nolan, C. Norman and L. Provost (2009). The improvement guide: a practical approach to enhancing organisational performance. San Franscisco, CA: Jossey-Bass.
Levesque, J.-F., M.F. Harris and G. Russell (2013). Patient-centred access to health care: conceptualising access at the interface of health systems and populations. International Journal for Equity in Health 12: 18. DOI: 10.1186/1475-9276-12-18.
Nilsen, P., J. Thor, M. Bender, J. Leeman, B. Andersson-Gäre and N. Sevdalis (2022). Bridging the silos: a comparative analysis of implementation science and improvement science. Frontiers in Health Services 1: 817750. DOI: 10.3389/frhs.2021.817750.
Ogrinc, G., S. Mooney, C. Estrada, T. Foster, D. Goldmann, L. Hall et al. (2008). The SQUIRE (Standards for QUality Improvement Reporting Excellence) guidelines for quality improvement reporting: explanation and elaboration. Quality and Safety in Health Care 17(Suppl 1): i13. DOI: 10.1136/qshc.2008.029058.
Percival, N., L. O’Donoghue, V. Lin, K. Tsey and R. Bailie (2016). Improving health promotion using quality improvement techniques in Australian Indigenous primary health care. Frontiers in Public Health 4: 53. DOI: 10.3389/fpubh.2016.00053.
Rakhmanova, N. and B. Bouchet (2017). Quality improvement handbook: a guide for enhancing the performance of health care systems. Durham, NC: FHI 360.
Rubenstein, L., D. Khodyakov, S. Hempel, M. Danz, S. Salem-Schatz, R. Foy et al. (2014). How can we recognize continuous quality improvement? International Journal for Quality in Health Care 26(1): 6–15. DOI: 10.1093/intqhc/mzt085.
Russell G., M. Harris, I.-H. Cheng, M. Kay, S. Vasi, C. Joshi et al. (2013). Coordinated primary health care for refugees: a best practice framework for Australia. Report to the Australian Primary Health Care Research Institute. Melbourne: Southern Academic Primary Care Research Unit.
Sollecito, W. and J. Johnson (2019). McLaughlin and Kaluzny’s continuous quality improvement in health care. Burlington, MA: Jones & Bartlett Learning.
Taylor, M., C. McNicholas, C. Nicolay, A. Darzi, D. Bell and J. Reed (2014). Systematic review of the application of the plan–do–study–act method to improve quality in healthcare. BMJ Quality & Safety 23: 290–8. DOI: 10.1136/bmjqs-2013-001862.
Woolcock, K. (2019). Value based health care: setting the scene for Australia. Deeble Institute for Health Policy Research. Canberra: Australian Healthcare and Hospital Association.
World Economic Forum (2017). Value in healthcare: laying the foundation for health system transformation. Geneva, Switzerland: World Economic Forum.
World Health Organization (2023). Quality of care. https://www.who.int/health-topics/quality-of-care#tab=tab_1.
1 World Health Organization 2023.
2 Rakhmanova and Bouchet 2017; World Health Organization 2023.
3 Levesque, Harris and Russell 2013.
4 Davy, Harfield et al. 2016.
5 Russell, Harris et al. 2013.
6 Davies and Wood 2018.
7 Levesque, Harris and Russell 2013.
8 Bailie, Schierhout et al. 2015.
9 Jackson and Ball 2018.
10 Al-Azri 2008.
11 Coulter 2017; European Commission 2019.
12 European Commission 2019.
13 World Economic Forum 2017, 8.
14 Woolcock 2019.
15 Woolcock 2019.
16 Bailie, Matthews et al. 2013.
17 Batalden and Davidoff 2007, 2.
18 Agency for Healthcare Research and Quality 2019.
19 Sollecito and Johnson 2019, 4–5.
20 As numerous sources and CQI resources identify these features, specific sources are not cited.
21 Rubenstein, Khodyakov et al. 2014.
22 Information about the framework is expanded in Chapter 4.
23 Berwick 1996.
24 Sollecito and Johnson 2019.
25 Nilsen, Thor et al. 2022.
26 Ogrinc, Mooney et al. 2008.
27 Deming 2018.
28 Taylor, McNicholas et al. 2014.
29 Sollecito and Johnson 2019.
30 Bailie, Si et al. 2007; Brimblecombe, Bailie et al. 2017; Percival, O’Donoghue et al. 2016.
31 Taylor, McNicholas et al. 2014.
32 Deming 2018, 91.
33 Langley, Moen et al. 2009.
34 Berwick 1996, 620.