1
Primary health care
What is primary health care?
The fundamental premise of primary health care is that all people, everywhere, have the right to receive the right care in their community.1 PHC attends to the majority of a person’s health needs throughout their lifetime, including physical, mental and social wellbeing. PHC is people-centred rather than disease-centred. It is a whole-of-society approach that includes health promotion, disease prevention, treatment, rehabilitation and palliative care.2
Primary health care attends to the majority of a person’s health needs throughout their lifetime.
Primary health care was formally defined in 1978, in the landmark Declaration of Alma-Ata, but use of the terms “primary care” and “PHC” pre-date 1978, and approaches that we now call primary health care were being pioneered by progressive public health practitioners several decades earlier. The World Health Organization (WHO) Declaration endorsed an international definition of PHC in 1978 as follows:
essential health care based on practical, scientifically sound and socially acceptable methods and technology made universally accessible to individuals and families in the community through their full participation and at a cost that the community and country can afford to maintain at every stage of their development in the spirit of self-reliance and self-determination. It forms an integral part both of the country’s health system, and of the overall social and economic development of the community. It is the first level of contact of individuals, the family and community with the national health system bringing health care as close as possible to where people live and work, and constitutes the first element of a continuing health care process.3
The WHO declaration also established these key principles of primary health care:
- universal access to care
- health equity as part of social justice
- individual and community participation and empowerment
- multi-sectoral policy and action
- integrated health services that meet people’s health needs throughout their lives
- health attainment through a fuller and better use of resources.
The 2018 Global Conference on Primary Health Care, held in Kazakhstan, affirmed these principles in a new declaration emphasising the critical role of PHC in meeting contemporary population health and health system challenges. The Declaration of Astana reinforces the ethical, political, social and economic imperative of achieving health equity and reducing disparities in health outcomes globally and for vulnerable populations. The declaration sets out this vision:
PHC and health services that are high quality, safe, comprehensive, integrated, accessible, available and affordable for everyone and everywhere, provided with compassion, respect and dignity by health professionals who are well-trained, skilled, motivated and committed.4
“PHC” is a broader term than “primary care”, which is used – mainly in the United Kingdom and northern America – to describe primary medical care or family practice.
A comprehensive approach
Comprehensive PHC is the most important part of the health system. Comprehensive PHC is vital to improving health outcomes and reducing health inequities – unnecessary, unfair and avoidable differences in health between groups within a population.5 A comprehensive PHC approach, as described in the Alma-Ata and Astana declarations, provides care in and through the community. In addition to meeting health needs across a person’s life span, comprehensive PHC attends to the broader social determinants of health through the involvement of other sectors in policy and action, such as food supply, education, housing, public infrastructure and communications.
In contrast, a selective PHC approach focuses on a disease or issue in isolation (for example, family planning, eradicating smallpox, reducing tuberculosis). After the Alma-Ata declaration, selective PHC was advocated as an interim strategy for improving health in low-income countries. A selective approach has had success in reducing diseases but has failed to promote community self-determination, equitable care and multi-sector action to improve and sustain health.6
Comprehensive PHC aims to empower individuals, families and communities to take charge of their own health and health care, and to tackle broader public health issues and risks to health. It also aims to meet the needs of defined populations, such as Indigenous peoples and those who, for various reasons, are missing out on services.7
Comprehensive PHC is vital to improving health outcomes and reducing health inequities.
Comprehensive PHC has a rich heritage. We highlight two early examples from South Africa where, in the late 1930s, public health practitioners who understood the links between broad aspects of health and development laid the foundations for a comprehensive curative and preventive service characterised by intersectoral action. The group argued that clinical services must be brought within the sphere of a broader social health scheme, and that health policy and practice must be informed by evidence. With government support, Kark, Cassel and colleagues established a rural health centre and trained community health workers to conduct an annual household health census, using the results to argue for sanitation and food production planning, and to study epidemiology and the influence of various environmental factors on people. These steps were the basis for what later became known as “community-oriented primary care”.8 It influenced the work of other PHC pioneers, such as the epidemiologist Susser and colleagues, who in the 1940s highlighted the connections between social justice and health, and the family, community and societal influences on health and disease. Although related ideas originated in the environmental conditions and epidemic contexts created by mass urban immigration (for example, in 19th-century industrial Britain and Europe), the South African approach in the mid-20th century heralded the emergence of community-oriented PHC and was pivotal for establishing international principles of PHC: health as a human right, health equity between populations as an aim of public health and service delivery by multidisciplinary teams.9 The right to health was institutionalised in the 1948 United Nations Universal Declaration of Human Rights.10
Health systems that are focused on PHC deliver better and more equitable outcomes at lower cost than other aspects of the health services delivery system. Studies by Starfield and colleagues found that countries with stronger and more comprehensive PHC generally had a healthier population and lower all-cause mortality, while countries with low PHC scores as a group had poorer health outcomes across various indicators. There was a positive association between adequate features of PHC (accessible, comprehensive, coordinated, continuous and accountable care) and the provision of preventive services, and between PHC and (in contrast to specialty care) greater health equity within populations.11 High-quality PHC is also associated with strong PHC policy, lower hospitalisation rates for conditions managed by good clinical care, and lower healthcare costs.12
Population health
What is population health?
Population health can be described as the study of health and disease in defined populations. It is an organised response to protect and improve the health outcomes of a population: for example, children, First Nations peoples, refugees, people with low incomes.
In population health there is a focus on populations as entities (rather than the individuals who make up the population), an emphasis on health promotion and disease prevention strategies at a population level, and concern with the underlying social, economic, biological, genetic, environmental and cultural determinants of health of whole population groups. For example, using a population health approach one would ask “why does this particular population have a high incidence of diabetes or renal disease?”, whereas working at an individual level one might ask “why did this person develop diabetes or renal disease?”
Common principles
Population health shares many principles with comprehensive PHC, including a focus on holistic health and equity, community empowerment, intersectoral collaboration, health promotion, integrated services, multidisciplinary teams and evidence-based practice. These principles also align with the holistic definition of Aboriginal health (see below).
Population health responses often involve changes to policies, systems and structures to maintain and improve health and to prioritise health interventions for groups who are most in need. It is widely accepted that a comprehensive PHC approach can improve population health outcomes. It can link and strengthen health systems to meet population health needs.
Population health responses often involve changes to policies, systems and structures.
A population health approach is fundamental in continuous quality improvement in primary health care. While CQI often uses data gathered from individual client records, these data are brought together to show trends in the population’s health or in service delivery, and to inform population health improvement strategies.
The social, cultural, structural and environmental determinants of health
“Social determinants” is the commonly used term to describe the non-medical and behavioural influences on health: the conditions in which people are born, grow, live, work and age, and the wider forces and systems that shape daily life (for example, food and housing security). According to the WHO, these social conditions are the single most important determinant of good health or poor health.13
The social determinants of health identified by the WHO are social gradient, stress, early life, social exclusion, work, unemployment, social support, addiction, food and transport.14 Education, gender and ethnicity also have a marked influence on how healthy a person is. Factors such as girls’ access to schooling and the number of years of education have been shown to affect maternal, infant and child health.15 Discrimination against ethnic and racial minorities shapes some people’s access to services, employment and resources, with significant effects on health and wellbeing.16 In these respects, the social determinants of health are shaped by political, social and economic structures – sometimes called “structural determinants of health” – that are largely beyond a person’s control.
The social and structural determinants of health highlight the inequalities in health between and within countries. For example, the average life expectancy in low-income countries is 62 years compared with 81 years in high-income countries.17 As a wealthy country with one of the highest life expectancies in the world and a universal health insurance system, Australia provides a telling example of how social and structural inequalities influence health and life expectancy within countries. There is an estimated 8-year gap in life expectancy between Aboriginal and Torres Strait Islander peoples and the Australian average, with two-thirds of the health gap attributed to preventable chronic conditions.18 The social determinants of health and wellbeing for Aboriginal and Torres Strait Islander Australians are complex, multi-dimensional and bound in the history and legacy of colonisation. At least 34 per cent of the health gap is linked to education, employment, income, incarceration and housing quality.19 Forty-four per cent of Indigenous peoples live in regional areas and 18 per cent in remote and very remote areas with poorer access to services and employment.20 Framed from an Aboriginal and Torres Strait Islander viewpoint, social determinants include the history of health, racism and marginalisation, poverty, control over health, powerlessness, family separation, land and reconciliation.21 Improving health involves genuine commitment to tackling these determinants and strengthening the cultural determinants of health and wellbeing, such as connection to Country and community, kinship, cultural expression, language and cultural leadership.
Environmental determinants, for example water and air quality and the impacts of extreme weather events, are also critical to health. The environmental effects of climate change pose an increasing risk to human health into the future.
A comprehensive approach to PHC takes intersectoral action on the various determinants of health.
A comprehensive approach to PHC takes intersectoral action on the various determinants of health to improve health and reduce health inequalities. It aims to improve the circumstances in which people live and work, and complements efforts to control major diseases, improve health systems and reduce poverty.22 This requires high-quality health systems that consistently deliver services to improve or maintain health, are valued and trusted, and respond to changing population needs.23
In Australia
In Australia, PHC encompasses a range of providers and services across the public, private and non-government sectors. PHC services include health promotion, prevention and screening, early intervention, treatment of acute conditions and management of chronic conditions. PHC services are delivered in settings such as general practices, community health centres, allied health practices and via communication technologies such as telehealth and video consultations. Use of these technologies increased during the Covid-19 pandemic. PHC professionals include, but are not limited to, general practitioners (GPs), nurses, nurse practitioners, allied health professionals, midwives, Aboriginal and Torres Strait Islander health practitioners and workers, pharmacists and dentists, and a broader network of community and social support workers. The Australian universal public health insurance scheme, Medicare, is funded to provide free or subsidised PHC, and approximately 35 per cent of total health funding is spent on PHC, similar to spending on hospital services.24
Despite Australia’s comparatively well-funded and well-functioning health systems, many Australians experience inequitable access to PHC services and a lack of integration between PHC and other parts of the health system. Policy and system reforms have been implemented to reduce the fragmentation of services and to improve the efficiency and integration of local systems to meet client and population needs. Examples include the 2020–2025 National Health Reform Agreement;25 the establishment of Primary Health Networks, which aim to streamline health services and improve care coordination; the trial of “Health Care Homes”;26 and MyMedicare,27 a voluntary patient registration model to formalise relationships between clients and general practices or between clients and PHC providers or both. Improvement is most needed in regional and remote areas, where around one-third of all Australians live, and where health outcomes are generally poorer relative to metropolitan areas. In fact, the prevalence of health risk factors, levels of illness and mortality generally worsen with increased distance from major cities, while access to PHC is reduced. So, while Australia matches or outperforms many comparable countries on selected measures of health, there is a need for a more equitable distribution of health resources and better access to core PHC services (listed below) across the population.28
Despite Australia’s comparatively well-funded and well-functioning health systems, many Australians experience inequitable access to PHC services.
A study conducted in 2012 found consensus among policymakers, academics, clinical practitioners and consumers on the essential PHC services that all Australians should expect to receive, regardless of where they live. These are the essential services:
- care of the sick and injured
- mental health and social and emotional wellbeing
- maternal and child health
- allied health
- sexual and reproductive health
- rehabilitation
- oral and dental health
- public health and illness prevention.
The essential PHC functions needed to support these services were identified as management (including governance and leadership), coordination, health infrastructure, quality systems, data systems, professional development and community participation.29
The Aboriginal and Torres Strait Islander approach
Aboriginal and Torres Strait Islander peoples are the first peoples of Australia, comprising hundreds of nations with distinct histories, languages and cultural traditions. Across diverse nations and communities, and shared with other Indigenous peoples, is a strong tradition of unity with the environment30 (often expressed in Australia as connection to Country) and a holistic view of health incorporating the spiritual, intellectual, physical and emotional dimensions of life. Health and survival are viewed as both a collective and individual intergenerational continuum.31 This concept underpins contemporary definitions of Aboriginal and Torres Strait Islander health and wellbeing. Seen through this lens, PHC is a holistic approach that is culturally embedded in a way that supports the social, emotional, physical and cultural wellbeing of Aboriginal and Torres Strait Islander peoples, families and communities.
Aboriginal and Torres Strait Islander Australians access PHC through Aboriginal community controlled and government-managed health services and through private general practices. Aboriginal community controlled health organisations emerged in the 1970s because mainstream services were not dealing adequately with the health needs of Aboriginal and Torres Strait Islander peoples who wanted to be able to provide care to their communities that was culturally appropriate, holistic and accessible. By the 1990s, these organisations were important providers of comprehensive PHC for Aboriginal and Torres Strait Islander peoples.32
Because most Aboriginal and Torres Strait Islander PHC services deliver care to the communities that operate and control them (through elected boards), they are also important for employment, professional education, community empowerment and social action. Aboriginal and Torres Strait Islander PHC services (which can be government-run or community controlled) have close relationships with the people they serve, local knowledge of community, and increased cultural awareness.33 The Aboriginal and Torres Strait Islander model of PHC delivery embodies comprehensive PHC as defined in the Declaration of Alma-Ata.
PHC complexity and systems approaches
PHC is complex in its scope and the way it is delivered. It requires the provision of holistic and client-centred care for people of all ages, for physical, psychological and social conditions, and for diseases affecting any body organ. It also needs to take account of complex health needs and personal and family circumstances. In terms of delivery, PHC providers are diverse, widely dispersed, relatively independent in their practice and work within a variety of funding and governance models with differing resources and infrastructure support. The PHC information systems available to providers are often relatively undeveloped and fragmented, yet PHC providers need to work closely with many other providers, funders, policymakers and their local communities to deliver effective care.34 Furthermore, the balance between acute and chronic health problems continues to shift globally, with increases in chronic conditions and comorbidities, and a corresponding need for health promotion, prevention, referral to specialised services (sometimes distant), integration of care and support for self-management. This complexity has implications for the PHC workforce, who need knowledge of public and population health perspectives and skills in client-centred care, partnering, using information and communication technology, and continuous quality improvement.35 The systems through which PHC is governed, managed and delivered need to respond effectively to these complexities.
PHC is complex in its scope and the way it is delivered.
Health systems and systems thinking
Advances in systems thinking have helped in understanding and attending to complexity in PHC. A system is a set of interacting parts, which form an integrated whole. All systems are made up of multiple elements, links between elements (the processes and interrelationships that hold the elements together) and a boundary that determines what is inside and outside the system. Systems thinking is a way of thinking about health systems as holistic, dynamic and interconnected.
The WHO defines a health system as “all organisations, people, and actions whose primary interest is to promote, restore, or maintain health”. This includes efforts to influence determinants of health as well as direct health-improving activities. The goals of a health system are “improving health and health equity in ways that are responsive, financially fair, and make the best, or most efficient, use of available resources”.36
Six building blocks for strengthening health systems
To advance health system goals, the WHO identified “six building blocks” for strengthening health systems:
- service delivery
- health workforce
- information
- medical products, vaccines and technologies
- financing
- leadership and governance.37
Each building block represents an essential health system function and is interdependent with other parts of the system, highlighting the need for integrated responses to build overall health system capacity.
The WHO model has been criticised for excluding a community health element, which may be added when interpreting the building blocks.38 Including “community” as a foundational building block recognises that health systems, through governments and policy leaders, need to respond to the effects of social and environmental determinants of health to design inclusive services tailored to community needs. It is also recognised that multi-sectoral approaches and community participation are needed to tackle underlying causes of poor health such as food insecurity, unsafe water and poor sanitation.39
Ten building blocks for high performance
Bodenheimer and colleagues studied exemplar PHC practices in the United States of America and used a similar building-blocks approach to describe key elements of high-performing, client-centred PHC. They propose engaged leadership, data-driven improvement, empanelment (patient registration) and team-based care as the foundation for implementing six other elements: client–team partnership; population management; continuity of care; prompt access to care; comprehensiveness and care coordination; and informing a template of the future (Figure 1.1).40
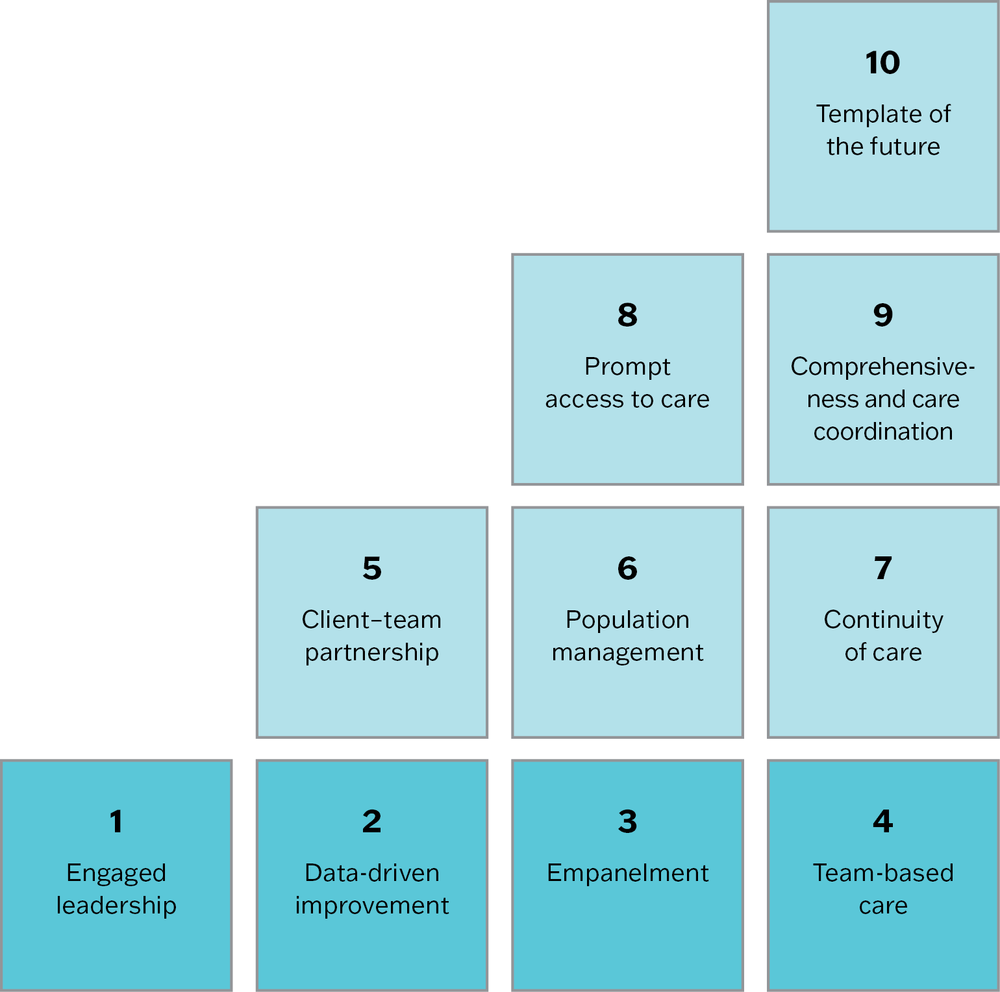
Figure 1.1 The 10 building blocks of high-performing primary health care. Adapted with permission from the Center for Excellence in Primary Care 2002. Source: 2012 UCSF Center for Excellence in Primary Care.
Innovative Care for Chronic Conditions Framework
The “Innovative Care for Chronic Conditions Framework” represents a systems approach to the prevention and management of chronic conditions in PHC settings. The Framework (Figure 1.2) presents the actions and interactions required at three levels of the healthcare system to achieve better outcomes for chronic conditions. Each part of the framework needs to function effectively, while interacting with and dynamically influencing actions and events at the other two levels.
- A positive policy environment serves to strengthen partnerships, support legislative frameworks and integrate policies into care and provide leadership and advocacy. Consistent financing is promoted, and human resources are developed and allocated.
- Healthcare organisations promote care continuity and coordination, encourage quality through leadership and incentives, organise and equip healthcare teams, use information systems, and support self-management and prevention.
- Actions are taken at the community level to raise awareness and reduce stigma, encourage better outcomes through leadership and support, mobilise and coordinate resources, and provide complementary services. Informed community partners and motivated healthcare teams link patients and families.
In each of these concepts of health system frameworks, the individual elements (or building blocks) are important, and effective interactions between the building blocks are essential for effective system functioning. Both PHC frameworks highlight continuous, well-coordinated care and engaged clients and communities as important aspects of service performance.
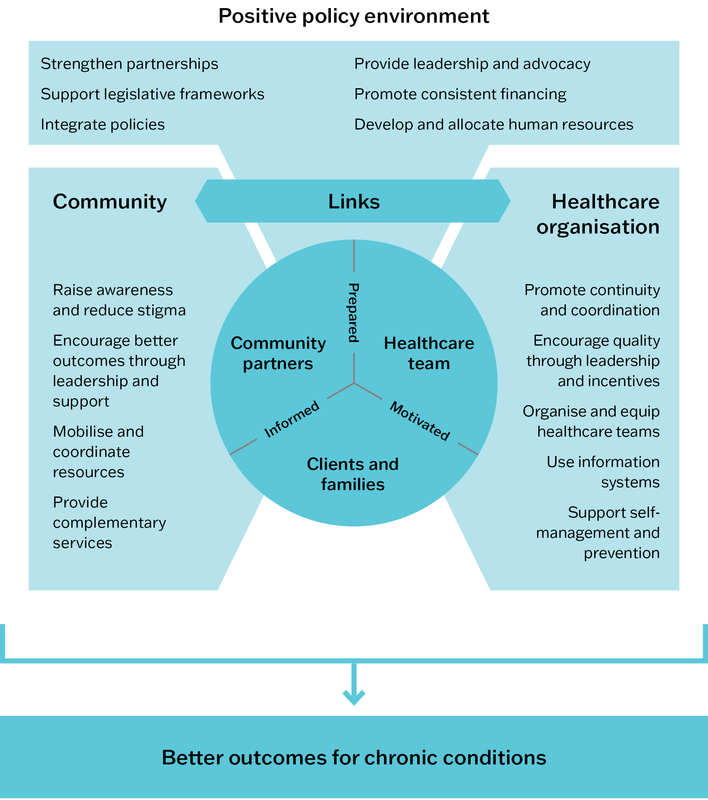
Figure 1.2 Innovative Care for Chronic Conditions Framework. World Health Organization 2002, 65.
Health services as complex adaptive systems
Health services are often described as complex adaptive systems. “Complexity” arises from a system’s interconnected parts, and “adaptivity” from its ability to change based on what occurs.41
Each individual PHC service is a complex adaptive system within larger complex adaptive systems (for example, government, organisation, community). Consistent with other systems, PHC systems have these characteristics:
- self-organising, whereby parts of the system tend to organise into an ordered state
- dynamic, interdependent and tightly linked – they are constantly adapting to change and evolving over time, with effects that may differ in the short and long term
- driven by interactions between systems components and governed by feedback, with responses having a flow-on effect that may be positive, negative or neutral
- nonlinear and often unpredictable, with changes in one part of the system producing unexpected changes in other parts, and effects that may be greater or less than what was intended
- sometimes counterintuitive in the way they behave – for example, a simple intervention that works well in one setting may not work in a similar setting
- often resistant to policy change, because of these features.42
Each individual PHC service is a complex adaptive system within larger complex adaptive systems.
Overall, a systems approach to PHC considers the many elements, dynamics and factors influencing health. By understanding how these elements operate independently, and how they depend on and influence one another, a systems approach can help with the design and integration of PHC staffing, processes, facilities, organisations and policies to promote better health and to improve client experiences and outcomes at lower cost.
Systems thinking is used to understand, analyse, learn from, manage and change how systems work. It is essential for improving the quality of PHC. We write about the skills and tools for systems thinking in Chapter 6.
Summary
This chapter has defined PHC and traced its development to understand how a comprehensive approach to PHC has evolved internationally and in Australia. We have explained important concepts in PHC, including population health, the social determinants of health, and systems approaches to care. These concepts also underpin quality improvement. In the next chapter, we define “quality” and CQI. We describe how CQI evolved in health care, before considering how conventional approaches to it need to be adapted for practical application in PHC in Chapter 3.
References
Anderson, I., F. Baum and M. Bentley, eds (2004). Beyond bandaids: exploring the underlying social determinants of Aboriginal health. Papers from the Social Determinants of Aboriginal Health Workshop, Adelaide, Darwin: Cooperative Research Centre for Aboriginal Health.
Australian Institute of Health and Welfare (2020). Australia’s health 2020 data insights. Canberra: Australian Government. Australia’s Health series no. 17. Cat. no. AUS 231.
Australian Institute of Health and Welfare (2018). Australia’s health 2018. Canberra: AIHW. Cat. no. AUS 221.
Australian Institute of Health and Welfare (2016). Primary health care in Australia. Canberra: AIHW. Cat. No. WEB 132.
Bailie, R., V. Matthews, J. Brands and G. Schierhout (2013). A systems-based partnership learning model for strengthening primary healthcare. Implementation Science 8. DOI: 10.1186/1748-5908-8-143.
Bodenheimer, T., A. Ghorob, R. Willard-Grace and K. Grumbach (2014). The 10 building blocks of high-performing primary care. Annals of Family Medicine 12(2): 166–71. DOI: 10.1370/afm.1616.
Burns, J., S. Burrow, N. Drew, M. Elwell, C. Gray, M. Harford-Mills et al. (2015). Overview of Australian Indigenous health status, 2014. Perth, WA: Australian Indigenous HealthInfoNet.
Center for Excellence in Primary Care (2012). What are the building blocks? https://cepc.ucsf.edu/what-are-building-blocks.
Commission on Social Determinants of Health (2008). Closing the gap in a generation: health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health. Geneva: World Health Organization.
Committee on Indigenous Health (2002). The Geneva Declaration on the Health and Survival of Indigenous Peoples. New York: United Nations Permanent Forum on Indigenous Issues.
Crear-Perry, J., R. Correa-de-Araujo, T. Lewis Johnson, M.R. McLemore, E. Neilson and M. Wallace (2021). Social and structural determinants of health inequities in maternal health. Journal of Women’s Health 30(2): 230–5. DOI: 10.1089/jwh.2020.8882.
de Savigny, D. and T. Adam, eds (2009). Systems thinking for health systems strengthening. Geneva, Switzerland: Alliance for Health Policy and Systems Research, World Health Organization.
Department of Health (2020). Primary health networks. https://www.health.gov.au/our-work/phn.
Department of Health and Aged Care (2024). MyMedicare. https://www.health.gov.au/our-work/mymedicare.
Department of Health and Aged Care (2021). National health reform agreement: long-term health reforms roadmap. Canberra: Australian Government.
Durie, M. (2004) Understanding health and illness: research at the interface between science and indigenous knowledge. International Journal of Epidemiology 33(5) 1138–43. DOI 10.1093/ije/dyh250.
Jackson, C. and S. Hambleton (2017). Australia’s Health Care Homes: laying the right foundations. Medical Journal of Australia 206(9): 380–1. DOI: 10.5694/mja16.01470.
Kark, S.l. and Cassel, J. (1999–2005). The Pholela Health Centre: A progress report. 1952. Bulletin of the World Health Organization 77 (5): 439–47.
Keleher, H. (2001). Why primary health care offers a more comprehensive approach to tackling health inequities than primary care. Australian Journal of Primary Health 7(2): 57–61. DOI: 10.1071/PY01035.
Kruk, M., A. Gage, C. Arsenault, K. Jordan, H. Leslie, S. Roder-Dewan et al. (2018). High-quality health systems in the Sustainable Development Goals era: time for a revolution. Lancet Global Health 6(11): E1196–E252.
Larkins, S., C.E. Woods, V. Matthews, S.C. Thompson, G. Schierhout, M. Mitropoulos et al. (2016). Responses of Aboriginal and Torres Strait Islander primary health-care services to continuous quality improvement initiatives. Frontiers in Public Health 3. DOI: 10.3389/fpubh.2015.00288.
Magnussen, L., J. Ehiri and P. Jolly (2004). Comprehensive versus selective primary health care: lessons for global health policy. Health Affairs 23(3): 167–76. DOI: 10.1377/hlthaff.23.3.167.
Marmot, M. (2005). Social determinants of health inequalities. Lancet 365: 1099–104.
Mensch, B., E. Chuang, A. Melnikas and S. Psaki (2019). Evidence for causal links between education and maternal and child health: systematic review. Tropical Medicine and International Health 24(5): 504–22. DOI: 10.1111/tmi.13218.
National Aboriginal Community Controlled Health Organisation (2022). Publications and resources. Key facts. https://www.naccho.org.au/publications-resources/.
Productivity Commission (2021). Innovations in care for chronic health conditions. Productivity Reform Case Study. Canberra: Commonwealth of Australia.
Sacks, E., M. Morrow, W. Story, K. Shelley, D. Shanklin, M. Rahimtoola et al. (2019). Beyond the building blocks: integrating community roles into health systems frameworks to achieve health for all. BMJ Global Health 3(Suppl 3): e001384. DOI: 10.1136/bmjgh-2018-001384.
Starfield, B. (2012). Primary care: an increasingly important contributor to effectiveness, equity, and efficiency of health services. SESPAS report 2012. Gaceta Sanitaria 26(S): 20–6. DOI: 10.1016/j.gaceta.2011.10.009.
Starfield, B. (1994). Is primary care essential? Lancet 344(8930): 1129–33. DOI: 10.1016/S0140-6736(94)90634-3.
Starfield, B., L. Shi and J. Macinko (2005). Contribution of primary care to health systems and health. Milbank Quarterly 83(3): 457–502.
Sterman, J. (2006). Learning from evidence in a complex world. American Journal of Public Health 96(3): 505–14. DOI: 10.2105/AJPH.2005.066043.
Susser, M. (1999). Pioneering community-oriented primary care. World Health Organization. Bulletin of the World Health Organization 77(5): 436–8.
Susser, M. (1993). Health as a human right: an epidemiologist’s perspective on the public health. American Journal of Public Health 83(3): 418–26. DOI: 10.2105/AJPH.83.3.418.
Thomas, S., J. Wakerman and J. Humphreys (2015). Ensuring equity of access to primary health care in rural and remote Australia – what core services should be locally available? International Journal for Equity in Health 14(1): 111. DOI: 10.1186/s12939-015-0228-1.
Thomas, S.L., J. Wakerman and J.S. Humphreys (2014). What core primary health care services should be available to Australians living in rural and remote communities? BMC Family Practice 15: 143. DOI: 10.1186/1471-2296-15-143.
Whitehead, M. (1992). The concepts and principles of equity and health. International Journal of Health Services 22(3): 429–45. DOI: 10.2190/986L-LHQ6-2VTE-YRRN.
Wilkinson, R. and M. Marmot, eds (2003). Social determinants of health: the solid facts, 2nd edn. Copenhagan, Denmark: World Health Organization.
World Health Organization (2018a). Declaration of Astana. Global Conference on Primary Health Care: From Alma-Ata towards universal health coverage and the Sustainable Development Goals. Astana, Kazakhstan 25–26 October 2018: World Health Organization and the United Nations Children’s Fund (UNICEF).
World Health Organization (2018b). Health inequities and their causes. https://www.who.int/news-room/facts-in-pictures/detail/health-inequities-and-their-causes.
World Health Organization (2018c). Primary health care. http://www.who.int/primary-health/en/.
World Health Organization (2008). The world health report 2008: primary health care – now more than ever. Geneva, Switzerland: WHO.
World Health Organization (2007). Everybody’s business: strengthening health systems to improve health outcomes: WHO’s framework for action. Geneva, Switzerland: WHO.
World Health Organization (2005). Preparing a health care workforce for the 21st century: the challenge of chronic conditions. Geneva, Switzerland: WHO.
World Health Organization (2002). Innovative care for chronic conditions: building blocks for action: global report. Geneva, Switzerland: WHO.
World Health Organization (1978). Declaration of Alma-Ata. International Conference on Primary Health Care, Alma-Ata, USSR: WHO.
Yach, D. and S. Tollman (1993). Public health initiatives in South Africa in the 1940s and 1950s: lessons for a post-apartheid era. American Journal of Public Health 83(7): 1043–50. DOI: 10.2105/AJPH.83.7.1043.
1 World Health Organization 2018c.
2 World Health Organization 2018c.
3 World Health Organization 1978, 2–3.
4 World Health Organization 2018a, 1.
5 Starfield, Shi and Macinko 2005; Whitehead 1992.
6 Magnussen, Ehiri and Jolly 2004.
7 Keleher 2001; World Health Organization 2008, 2018b.
8 Kark and Cassel 1999-2005; Yach and Tollman 1993.
9 Susser 1993, 1999.
10 Susser 1993.
11 Starfield 1994, 2012; Starfield, Shi and Macinko 2005.
12 Starfield 2012.
13 Commission on Social Determinants of Health 2008.
14 Wilkinson and Marmot 2003.
15 Mensch, Chuang et al. 2019.
16 Anderson, Baum and Bentley 2004; Crear-Perry, Correa-de-Araujo et al. 2021.
17 World Health Organization 2018b.
18 Productivity Commission 2021.
19 Burns, Burrow et al. 2015.
20 Australian Institute of Health and Welfare 2020.
21 Anderson, Baum and Bentley 2004.
22 Marmot 2005.
23 Kruk, Gage et al 2018.
24 Australian Institute of Health and Welfare 2016.
25 Department of Health and Aged Care 2021.
26 Department of Health 2020; Jackson and Hambleton 2017.
27 Department of Health and Aged Care 2024.
28 Australian Institute of Health and Welfare 2018; Thomas, Wakerman and Humphreys 2015.
29 Thomas, Wakerman and Humphreys 2014.
30 Durie 2004.
31 Committee on Indigenous Health 2002.
32 National Aboriginal Community Controlled Health Organisation 2022.
33 Larkins, Woods et al. 2016.
34 Bailie, Matthews et al. 2013.
35 World Health Organization 2005.
36 World Health Organization 2007, 2.
37 World Health Organization 2007.
38 Sacks, Morrow et al. 2019.
39 Sacks, Morrow et al. 2019.
40 Bodenheimer, Ghorob et al. 2014.
41 de Savigny and Adam 2009.
42 de Savigny and Adam 2009; Sterman 2006.