10
Improving diabetes care
Diabetes
Diabetes is a chronic condition marked by high levels of glucose in the blood. It is caused by the body’s inability to effectively produce or use insulin, a hormone that regulates blood glucose. Undiagnosed or poorly managed diabetes leads to serious damage to many of the body’s systems over time, and to premature death. Adults with diabetes have two to three times the risk of heart attacks and strokes. Reduced blood flow and nerve damage from uncontrolled diabetes increase the risk of ulcers, infection and limb amputation. Diabetes is among the leading causes of kidney failure and causes 2.6 per cent of global blindness.1
Diabetes is the world’s fastest growing chronic condition. The global prevalence of diabetes among adults rose from 4.7 per cent (108 million) in 1980 to 8.5 per cent (422 million) in 2014,2 and was estimated to be 9.3 per cent (463 million people) in 2019, and projected to rise to 10.2 per cent (578 million) by 2030.3 The International Diabetes Federation reported that diabetes caused 6.7 million deaths in 2021, with 75 per cent of people with diabetes living in low- and middle-income countries and almost half of people with diabetes not diagnosed.4
Type 2 diabetes is the most common form of diabetes and results from a combination of genetic and environmental factors. Although genetics play a major role, the risk of developing type 2 diabetes increases with factors such as high blood pressure, high blood cholesterol, overweight or obesity, poor diet and insufficient physical activity. Multiple risk factors increase the chances of developing diabetes, including historical, social and cultural factors that have resulted in health, social and economic inequities. These factors also challenge effective disease management.5 Indigenous Peoples and other racial or ethnic minorities who experience oppression have comparatively higher rates of diabetes, and diabetes-related complications and mortality.6 Until recently, type 2 diabetes was mostly seen in adults, but incidence among children is rising. Women who develop gestational diabetes, and their children, have increased risk of developing type 2 diabetes in the future. Type 1 diabetes, which is managed with insulin, generally occurs from childhood and is not preventable with current knowledge.7
Aboriginal and Torres Strait Islander peoples
Type 2 diabetes contributes significantly to the disease burden of Aboriginal and Torres Strait Islander peoples, with cardiovascular and metabolic diseases responsible for most of the gap in life expectancy compared with the non-Indigenous population. Diabetes risk factors are higher for Aboriginal and Torres Strait Islander peoples and prevalence is increasing.8 In 2018–19, 13 per cent of Aboriginal and Torres Strait Islander adults reported having diabetes or high sugar levels. This increased with age, from 0.8 per cent for those aged 18–24, to more than one-third of those aged 55 and over (36 per cent).9 The age of onset is younger than for non-Indigenous Australians, and the rate of new diagnoses among young people is rising.10
The evidence of severe and increasing impact of diabetes has led to development of programs and strategies to improve diabetes health outcomes, including through holistic, culturally appropriate care tailored to meet the needs of communities. The above statistics highlight the critical importance of effective diabetes prevention and management. Programs and services need to be supported by broader actions that address the historical and social causes of Aboriginal and Torres Strait Islander health inequity – colonisation, land dispossession, displacement, disempowerment, social and economic exclusion, and systemic racism11 – and that embrace Indigenous values and concepts of health and wellbeing.
Recommended clinical care
A comprehensive PHC approach
Recommendations for improving diabetes prevention and management apply across populations and settings. Diabetes prevention programs need to work across the life cycle. Effective diabetes management requires earlier detection of undiagnosed diabetes, good quality care including management of comorbidities and service integration, social and emotional wellbeing support for clients, access to medications, self-management education and specialist treatment when complications develop.
Diabetes prevention
A holistic approach can help people to reduce their risk of developing type 2 diabetes. Prevention measures should include public health approaches (for example, ensuring access to affordable healthy foods, appropriate services and resources); community health promotion programs (for example, supporting communities and groups to develop and deliver prevention programs); and individual approaches that identify people at high risk using risk assessment tools, provide clients with education, and support people to increase physical activity, reduce obesity, eat healthy foods and avoid tobacco use.
Identifying risk – early detection
Australian guidelines recommend screening people for risk of type 2 diabetes every three years from 40 years of age, and from 18 years for Aboriginal and Torres Strait Islander peoples.12 The CARPA Standard Treatment Manual recommends a preventive health check, which includes diabetes screening, every two years for Aboriginal and Torres Strait Islander peoples 15 years and older, or annually for people with identified risk factors.13
Anyone who is identified with high risk factors for diabetes should be screened with fasting blood glucose (or glycated haemoglobin) every three years. People with an impaired glucose tolerance or fasting glucose test (not limited by age) should be screened every 12 months.
Managing comorbidities
Most clients with diabetes have at least one other chronic condition, which may or may not be diabetes related but which influences clinical management. Common comorbidities are high blood pressure, dyslipidaemia (abnormally high levels of fat in the blood), obesity, chronic kidney disease, chronic obstructive pulmonary disease and mental health problems.
Complications of diabetes
Having diabetes causes other health problems over time, making good diabetes management even more important. These other problems commonly include circulatory complications (coronary heart disease, stroke and peripheral vascular disease, which increases the risk of developing foot complications and can lead to amputations); renal complications (diabetic nephropathy or kidney damage, and chronic kidney failure); eye health complications (retinopathy, cataracts and glaucoma); nerve damage (peripheral neuropathy and autonomic neuropathy, which can affect organ function); depression and “diabetes distress” (a response to the emotional burden of managing diabetes).14
Care and management
Client-centred diabetes care aims to improve the person’s health and quality of life. Treatment decisions need to be based on best-practice clinical guidelines and be made from a position of understanding the client’s thoughts, fears, preferences and expectations, and their social, cultural, family and community context. Does the client have the resources needed for treatment and self-care? Do you need to link them with other agencies and support networks? Providing culturally safe care is essential (for example, engaging translators when required, responding to cultural values, involving staff with the same cultural or ethnic background in care delivery).
High-quality diabetes care includes cardiovascular risk assessment, visual acuity check, dilated eye check and foot check at least every 12 months, with appropriate follow-up and referral for specialist care as required. Up-to-date influenza and pneumococcal vaccinations are also recommended. Planning disease management in partnership with clients and organising multidisciplinary team care take account of many important factors: biomedical, medications, any complications of diabetes, cultural factors, social and emotional wellbeing, health literacy and available resources.
Chronic disease management plans should be developed and regularly reviewed in consultation with clients and their families or carers as appropriate. An initial review should be done within the first month after diagnosis, and then every three to six months, depending on the therapies used and the complexity of health issues.15 Regular review of management plans can result in improved care processes and clinical outcomes.16
Meeting the complex clinical care needs of all people diagnosed with diabetes requires well-functioning systems at different health system levels and coordination amongst different providers. PHC systems should support team-based care, community involvement, patient registries and embedded decision-support tools. PHC systems should also support the integration of clinical consultations by PHC teams, laboratory tests, specialist services, and community programs that protect and promote health and wellbeing.
Findings: quality of diabetes care
The data presented below on the quality of diabetes care come mainly from six research papers and key reports published by the ABCD CQI research program between 2007 and 2016. These are the most recent audit data available for analysis. Studies analysed more than 17,879 client records from 160 PHC centres between 2005 and 2014. Approximately half of the centres were in geographically remote locations; urban and regional PHC centres were also represented. PHC stakeholders participated in data interpretation to identify priority evidence-to-practice gaps and factors influencing improvement.
Clinical care: testing and control of blood glucose levels
Blood glucose (glycated haemoglobin or HbA1c) measurement is used to assess long-term blood glucose control. Good blood glucose control substantially reduces the risk of microvascular disease in diabetes, including kidney disease, retinopathy and neuropathy.
- Goals for HbA1c levels vary according to client circumstances; the general aim is for a level of 6.5–7.5 per cent (or 48–58 millimole per mole).
- Checks are recommended every three to six months (HbA1c readings assess blood glucose levels over the past three months).
- Follow-up action for an abnormal HbA1c reading should involve counselling about blood glucose control and closer monitoring. People with repeated or especially high readings need referral to a doctor for assessment and action, which may involve multiple interventions and medication adjustment.
Clinical audit and interpretation of the HbA1c data from the audits found several key points for CQI:
- Improvement was needed in regular monitoring of HbA1c, and in follow-up of abnormal HbA1c results and review of medication.
- Over time, the median rate of six-monthly HbA1c checks for clients with diabetes was relatively high (around 75 per cent) (Figure 10.1). There was consistently wide variation across health centres, which did not appear to improve over time for those health centres at the lower end of the range.
- Follow-up action for abnormal HbA1c results showed an improving trend in medication review across audit cycles. Median rates increased from 25 per cent to 60 per cent between cycles 1 and 4, but the variation in rates between health centres was consistently wide, ranging from 0 to 100 per cent in audit cycles 1 to 4 (Figure 10.2).17
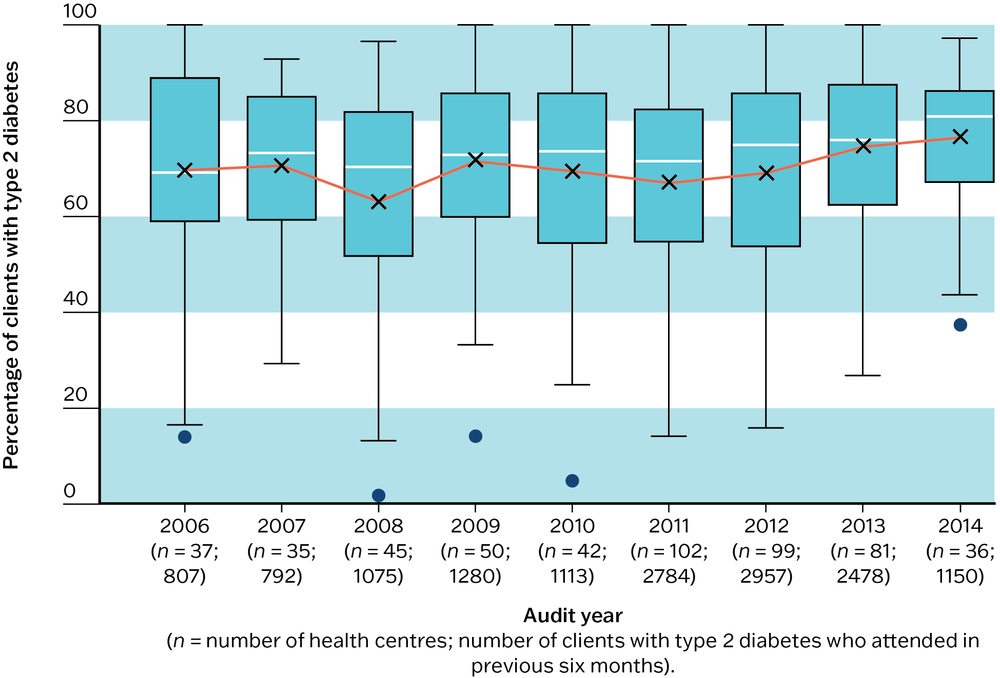
Figure 10.1 Mean health centre delivery of HbA1c checks within six months, by audit year for all health centres. Source: Matthews, Connors et al. 2015.
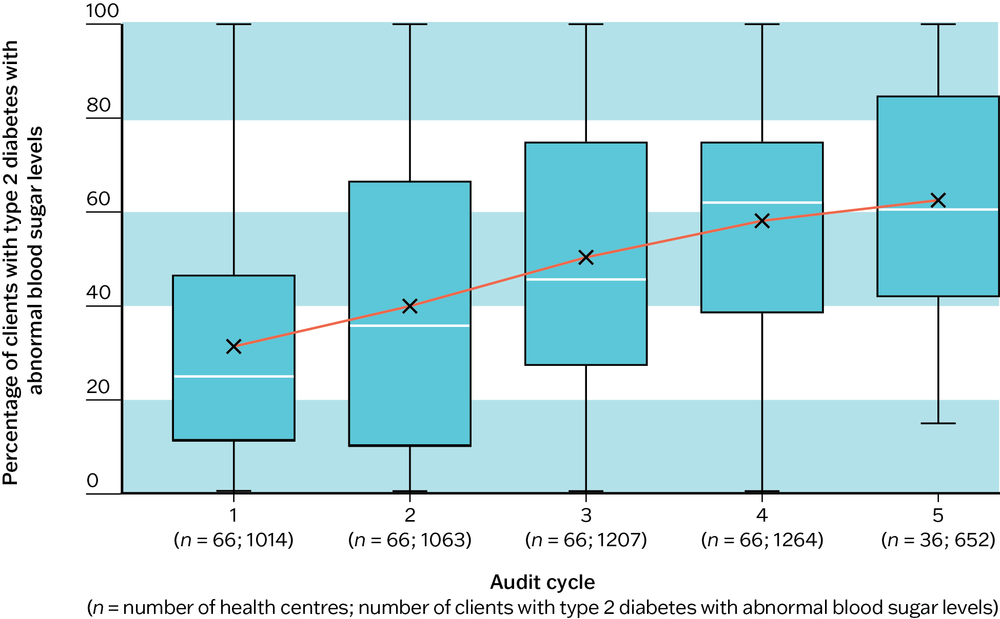
Figure 10.2 Mean health centre rates of medication review or adjustment for patients with abnormal HbA1c, by audit cycle for health centres that have at least three years of audit data. Source: Matthews, Connors et al. 2015.
Cardiovascular disease risk assessment and blood pressure control
People who have diabetes and pre-existing cardiovascular disease are at high risk of a cardiovascular event (see Chapter 16). The risk is also high if people with diabetes are older than 60 years, or if they have microalbuminuria (a high level of protein in the urine), moderate or severe chronic kidney disease, high blood cholesterol (serum total cholesterol over 7.5 mmol/L), or high blood pressure (more than or equal to 140/90 mmHg).18 Good blood pressure control is important for good diabetes care. Blood pressure targets are based on informed decision-making between clients and clinicians, considering the benefits and harms.
- Target blood pressure for people with diabetes depends on comorbidities and complications. The general target is less than or equal to 130/80 mmHg.19 Therapy is strongly recommended for clients with diabetes and systolic blood pressure more than or equal to 140 mmHg. A blood pressure target less than 140/90 mmHg is recommended for people with diabetes and hypertension. A systolic blood pressure target less than 120 mmHg may be considered when the priority is to prevent stroke.20
- When a client has a high blood pressure reading, it is important that appropriate follow-up action is taken: at least counselling the client about blood pressure control and frequent monitoring.
- A client with a repeated or especially high reading should be referred to a doctor for assessment and action, which may involve adjustment of medications and therapy to lower blood pressure (for example, angiotensin converting enzyme inhibitor or angiotensin receptor blocker) and should include discussion about lifestyle.
- Once control is achieved, blood pressure should be measured every three–six months.21
Clinical audit and interpretation of the data from the audits found several key points for CQI:
- Improvement was needed in regular monitoring of blood pressure, and in follow-up of abnormal blood pressure results and review of medication.
- Rates of medication review or adjustment for clients with abnormal blood pressure was generally low but improved over successive audit cycles. Median rates increased from 7 per cent to more than 30 per cent over four cycles (Figure 10.3).
- There was wide variation in blood pressure control and rates of medication review or adjustment between health centres.22
Follow-up of abnormal total cholesterol showed similar results and trends.
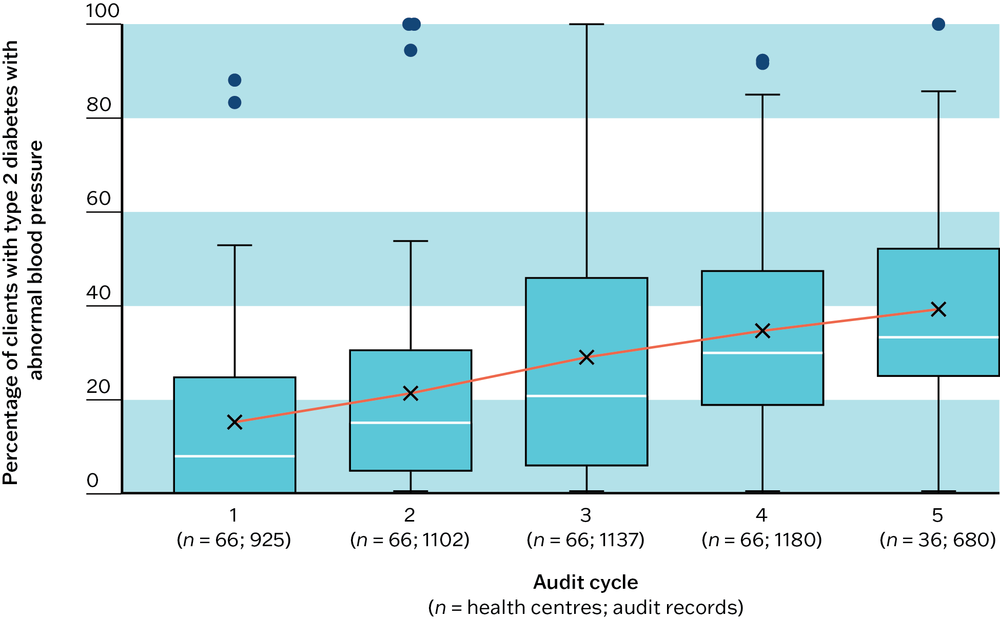
Figure 10.3 Mean health centre rates of medication review or adjustment for clients with abnormal blood pressure, by audit cycle for health centres that have at least three years of audit data. Source: Matthews, Connors et al. 2015.
Risk factors, brief intervention, counselling and education
Routine diabetes care involves identifying factors that are likely to progress disease severity and complications, and supporting clients to reduce these risks and self-manage their illness. Screening, brief intervention and, when necessary, counselling and referral may focus on social risk factors (food security, housing condition, financial support, family environment, experiences of trauma), or behavioural risk factors (for example, smoking, alcohol intake, other drug use, weight management, nutrition, exercise needs and social and emotional wellbeing).
Data from over 15,000 clinical audit records of clients with type 2 diabetes were collected from 162 PHC centres between 2005 and 2014. Analysis over nine audit cycles showed the following information:
- Delivery of brief intervention, counselling and education about risk factors showed improvement in early audit cycles, which then plateaued.
- Variation in these care processes for nutrition, physical activity and high-risk alcohol and other drug use may be influenced by the composition of PHC teams, allocation of work within teams, staff perceptions about the effectiveness and accessibility of support services, and different policies and practices for recording these care processes in client records.23
Diabetes and depression
Having diabetes more than doubles a person’s risk of developing depression.24 The combination of diabetes and depression presents a major clinical challenge as the outcomes of both conditions are generally worsened by the presence of the other: quality of life is poorer, diabetes self-management is impaired, the risk of diabetes complications is increased, and life expectancy is reduced.25 Coexisting diabetes and depression is associated with a 50 per cent increase in mortality risk.26 Despite this knowledge and the availability of effective screening tools, depression is frequently missed in people with diabetes.27 (See also Chapter 15, Improving mental health and wellbeing care.)
The high prevalence of diabetes in Aboriginal and Torres Strait Islander peoples and their reported high or very high levels of psychological distress and mental illness28 indicate that a high percentage of Aboriginal and Torres Strait Islander peoples who have diabetes experience depression.
The CQI research found low rates of screening for social and emotional wellbeing amongst people with diabetes. Screening and diagnosed depression were even lower for people with severe disease. Analysis of data from 62 PHC centres and 1,592 clinical audit records of clients with type 2 diabetes resulted in these findings:
- 14 health centres (23 per cent) had no documented depression in the records of clients with diabetes. For the remaining 48 health centres, documented depression varied between 3.3 and 36.7 per cent.
- One-third of the clients (45 of 140) with documented depression in their medical records had no recorded diagnosis of depression but had been prescribed a medication commonly used to treat depression.29
A later study of 1,174 clinical audit records of clients with type 2 diabetes from 44 PHC centres resulted in these findings:
- Documentation of screening for depression and of diagnosed depression was low overall (5 per cent and 6 per cent respectively) and even lower for clients with renal disease and with poorly controlled diabetes.
- Screening for depression was lower for those on medication for blood glucose control compared to those not on glucose-lowering medication.
- Antidepressant prescription was not associated with level of diabetes control or disease severity.30
Comprehensive diabetes care
Audit and systems assessment data for various aspects of diabetes care were brought together to analyse the overall quality of type 2 diabetes care (17,879 client records, 162 PHC centres). The audit tool used to collect the data included 22 best-practice indicators for type 2 diabetes care.31 The systems assessment tool included 5 key components and 18 scored items relating to PHC system support.32
The importance of continuous quality improvement work was reinforced by the findings, which enabled diabetes care to improve. Over the course of the audit years, these were the findings that emerged:
- The mean and median levels of care ranged between 60 and 80 per cent of service items, with some health centres delivering fewer than 40 per cent of the elements of best-practice care. There was an improvement trend and reducing variation between health centres over the final four years of data collection (Figure 10.4).
- Health centres with longer participation in CQI were more likely to be in the top quartile of delivery for all aspects of diabetes care.33
- There were different patterns of improvement for different aspects of diabetes care. While follow-up of abnormal results, screening for emotional wellbeing, recording of risk factors and brief interventions improved, there was no clear improvement for six-monthly checks of HbA1c, medication prescription, emotional wellbeing support and adult vaccinations.34
- Variation between health centres was less in the areas of medication prescriptions and medication review following abnormal findings, brief interventions and health centre systems. Variation did not reduce for six-monthly HbA1c checks, documentation of follow-up plan for abnormal blood pressure, emotional wellbeing screening and support, recording of risk factors and adult vaccinations.35
- Adherence to best-practice guidelines was linked to geographical remoteness of health centres (the more remote, the greater the adherence) and regularity of client attendance. Clients were more likely to receive higher quality care with increasing age, disease severity, comorbidity or complications, or a combination of these. Health centre factors explained most of the differences in level of service delivery rather than client factors.36
- Systems assessments identified the need to strengthen systems for more effective links between PHC services and communities, and links with other services and resources.37
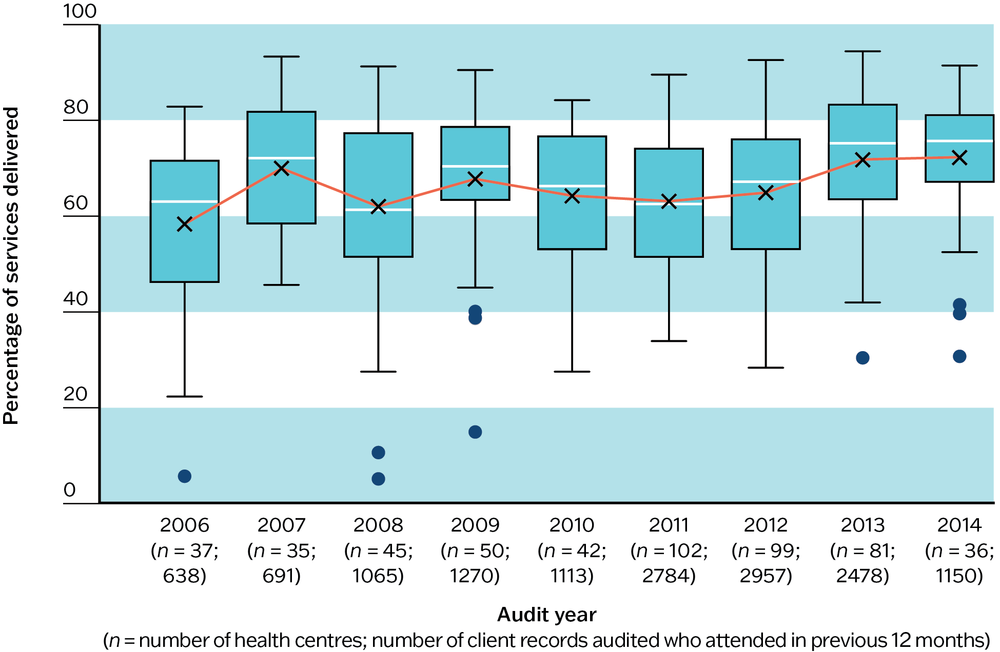
Figure 10.4 Trends in overall type 2 diabetes care. Source: Matthews, Connors et al. 2015.
Health centres with longer participation in CQI were more likely to be in the top quartile of delivery for all aspects of diabetes care.
Note: composite indicators include up to 22 best-practice indicators present in the type 2 diabetes audit tool: current chronic disease management plan; chronic disease management or medication discussion; influenza and pneumococcal vaccination; weight and waist circumference recorded (within six months); body mass index; blood pressure (within six months); visual acuity; dilated eye check; feet check; nutrition and physical activity advice; blood glucose level (within six months); urine albumin:creatinine ratio; estimated glomerular filtration rate; full lipid profile; total cholesterol; brief intervention if smoker or high risk alcohol user.
Across the studies, there was a need to strengthen systems and processes to support adherence to evidence-based clinical guidelines. Stakeholder input to data interpretation identified barriers and strategies for system improvement, as follows:
- staff recruitment and retention (for example, improving induction, training and mentoring programs; focusing on building a stable, qualified workforce)
- capacity to provide client-centred care (for example, modifying roles and career pathways for community health workers towards provision of comprehensive care; developing staff skills in holistic care; providing resources)
- community engagement and participation in the design of service delivery (for example, invest in strengthening health literacy and community leadership for quality improvement, develop staff skills in linking with the community)
- training and development of PHC teams and management (for example, in clinical skills, team building and collaboration, CQI knowledge and skills).38
Key messages for improving diabetes care
This CQI research identifies clear priorities and strategies for improving diabetes care in PHC and includes stakeholder interpretation of CQI data. Patterns of diabetes care delivery in Aboriginal and Torres Strait Islander PHC communities are likely to reflect, at least to some extent, care delivery in international settings.
There are common evidence-to-practice gaps in diabetes care that call for system-wide and local attention:
- follow-up of abnormal findings and review of medication, strengthening regular monitoring of blood glucose levels and reviewing and adjusting medication for clients with a recent abnormal blood glucose level, total cholesterol or blood pressure result
- adherence to evidence-based current treatment guidelines
- assessment and support regarding emotional wellbeing
- recording of risk factors, particularly cardiovascular risk assessment and healthy weight indicators, and recording of brief interventions and referrals (such as advice or referrals for physical activity and quit smoking programs)
- coverage of adult vaccinations
- development of systems for more effective links between PHC centres and communities.
There are several strategies that can be taken to improve the quality of diabetes care:
- At the local level, encourage regular attendance by clients with diabetes and those at high risk of developing diabetes.
- At different levels of the health system, focus on reducing systemic barriers and strengthening enablers for providing best-practice diabetes care. These are among the most important:
- staff recruitment and retention
- capacity to provide client-centred care
- community engagement and participation in the design of service delivery
- training and development of PHC teams and management.
Success in tackling systemic barriers for diabetes care will have a positive effect on the delivery of best-practice care for other chronic conditions and for PHC more generally.
- Involve a range of stakeholders in planning how to improve comprehensive diabetes care, including clients and carers or families, PHC practitioners and staff, health service and district and regional managers, support organisations and policymakers.
Sustained commitment by everyone involved in CQI is required to realise and demonstrate improvement.
Improving diabetes care in Aboriginal and Torres Strait Islander PHC
Our research into the quality of diabetes care for Aboriginal and Torres Strait Islander peoples spans almost 15 years, and studies show persistent wide variation in performance between different aspects of diabetes care and between health services and centres. While many aspects of diabetes care are being done well in many health centres, there are important and consistent gaps between evidence and practice in some aspects of diabetes care. Our research indicates that these gaps are system-wide and likely to be due to deficiencies in the broader PHC system. Together with the growing prevalence of diabetes at earlier ages, this evidence reinforces, firstly, the critical importance of taking both system-level and local action to improve diabetes prevention and care for Aboriginal and Torres Strait Islander peoples, and, secondly, the need to shape these actions to meet the self-determined needs of Aboriginal and Torres Strait Islander communities.
The concept of comprehensive diabetes care aligns with the holistic nature of Aboriginal and Torres Strait Islander wellbeing. Our research on engaging stakeholders in interpreting quality-of-care data provides evidence that the PHC workforce has the collective knowledge to find practical solutions to improving diabetes care. Effective processes for engaging communities in planning service design, and culturally competent and well-prepared PHC teams are key.39
Best-practice type 2 diabetes care involves team care and dictates that clients receive certain services at regular intervals. It is unsurprising that health centres with a higher percentage of clients not attending in the previous six months were less likely to provide best-practice diabetes care,40 but notable that health centre factors and jurisdiction-level support for CQI were more influential than client factors in adherence to best practice.41 A focus on improving health centre systems, therefore, is crucial for improving diabetes care.
A focus on improving health centre systems is crucial for improving diabetes care.
Every care-delivery context provides challenges for PHC teams (for example, coordinating and monitoring comprehensive delivery by multiple service providers in urban locations; managing high staff turnover, dispersed populations and limited access to specialist services in remote PHC settings). Flexible models of care, well-functioning care systems, good documentation of client care and use of CQI can help in overcoming these challenges. Policy and infrastructure support and organisational commitment to CQI has been associated with steady improvements or maintenance of high-quality diabetes care for Aboriginal and Torres Strait Islander communities.42
References
Australian Chronic Disease Prevention Alliance: National Vascular Disease Prevention Alliance (2012). Guidelines for the management of absolute cardiovascular disease risk. Melbourne: National Stroke Foundation.
Australian Institute of Health and Welfare (2023). Aboriginal and Torres Strait Islander Health Performance Framework 1.09 Diabetes. National Indigenous Australians Agency. Canberra: Australian Government. https://www.indigenoushpf.gov.au/measures/1-09-diabetes.
Australian Institute of Health and Welfare (2022). Australia’s health 2022: First Nations People – Indigenous health and wellbeing. Canberra: Australian Government. https://www.aihw.gov.au/reports/australias-health/indigenous-health-and-wellbeing.
Australian Institute of Health and Welfare (2015). Cardiovascular disease, diabetes and chronic kidney disease – Australian facts: Aboriginal and Torres Strait Islander people. Cardiovascular, Diabetes and Chronic Kidney Disease Series no. 5. Cat. no. CDK 5. Canberra: AIHW.
Bailie, R., V. Matthews, S. Larkins, S. Thompson, P. Burgess, T. Weeramanthri et al. (2017). Impact of policy support on uptake of evidence-based continuous quality improvement activities and the quality of care for Indigenous Australians: a comparative case study. BMJ Open 7. DOI: 10.1136/bmjopen-2017-016626.
Diabetes Australia (n.d.). Depression and mental health. Diabetes Australia. https://www.diabetesaustralia.com.au/living-with-diabetes/preventing-complications/depression-and-mental-health/.
Durey, A. and S. Thompson (2012). Reducing the health disparities of Indigenous Australians: time to change focus. BMC Health Services Research 12: 151. DOI: 10.1186/1472-6963-12-151.
Gabb, G., A. Mangoni, C. Anderson, D. Cowley, J. Dowden, J. Golledge et al. (2016). Guideline for the diagnosis and management of hypertension in adults – 2016. Medical Journal of Australia 205(2): 85–9. DOI: 10.5694/mja16.00526.
Gaskin, D., R. Thorpe, E. McGinty, K. Bower, C. Rohde, J. Young et al. (2014). Disparities in diabetes: the nexus of race, poverty, and place. American Journal of Public Health 104(11): 2147–55. DOI: 10.2105/AJPH.2013.301420.
Holt, R. and W. Katon (2012). Dialogue on diabetes and depression: dealing with the double burden of co-morbidity. Journal of Affective Disorders 142: S1–S3. DOI: 10.1016/S0165-0327(12)00632-5.
International Diabetes Federation (2021). Facts and Figures. International Diabetes Federation. https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-Figures.html.
Lin, E., S. Heckbert, C. Rutter, W. Katon, P. Ciechanowski, E. Ludman et al. (2009). Depression and increased mortality in diabetes: unexpected causes of death. Annals of Family Medicine 7(5): 414–21. DOI: 10.1370/afm.998.
Matthews, V., C. Connors, A. Laycock, J. Bailie and R. Bailie (2015). Chronic illness care for Aboriginal and Torres Strait Islander people: final report. ESP Project: Priority Evidence-Practice Gaps and Stakeholder Views on Barriers and Strategies for Improvement. Brisbane: Menzies School of Health Research.
Matthews, V., G. Schierhout, J. McBroom, C. Connors, C. Kennedy, R. Kwedza et al. (2014). Duration of participation in continuous quality improvement: a key factor explaining improved delivery of type 2 diabetes services. BMC Health Services Research 14(1): 578. DOI: 10.1186/s12913-014-0578-1.
Menzies School of Health Research and One21seventy (2015). Vascular and metabolic syndrome management clinical audit tool. Brisbane: Menzies School of Health Research.
Menzies School of Health Research and One21seventy (2012). Systems assessment tool – all client groups. Darwin: Menzies School of Health Research.
Naqshbandi, M., S. Harris, J. Esler and F. Antwi-Nsiah (2008). Global complication rates of type 2 diabetes in Indigenous peoples: A comprehensive review. Diabetes Research and Clinical Practice 82(1): 1–17. DOI: https://doi.org/10.1016/j.diabres.2008.07.017.
National Heart Foundation of Australia (2016). Guidelines for the diagnosis and management of hypertension in adults – 2016. Melbourne: National Heart Foundation of Australia.
Remote Primary Health Care Manuals, ed. (2022). CARPA standard treatment manual for remote and rural practice. Alice Springs, NT: Flinders University. https://www.remotephcmanuals.com.au/home.html.
Ride, K. and S. Burrow (2016). Review of diabetes among Aboriginal and Torres Strait Islander people. Australian Indigenous HealthInfoNet. Western Australia: Edith Cowan University.
Royal Australian College of General Practitioners (2020). Management of type 2 diabetes: a handbook for general practice. Melbourne: RACGP.
Saeedi, P., I. Petersohn, P. Salpea, B. Malanda, S. Karuranga, N. Unwin et al. (2019). Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edn. Diabetes Research and Clinical Practice 157: 107843-43. DOI: 10.1016/j.diabres.2019.107843.
Schierhout, G., V. Matthews, C. Connors, S. Thompson, R. Kwedza, C. Kennedy et al. (2016). Improvement in delivery of type 2 diabetes services differs by mode of care: a retrospective longitudinal analysis in the Aboriginal and Torres Strait Islander primary health care setting. BMC Health Services Research 16(1): 560. DOI: 10.1186/s12913-016-1812-9.
Schierhout, G., T. Nagel, D. Si, C. Connors, A. Brown and R. Bailie (2013). Do competing demands of physical illness in type 2 diabetes influence depression screening, documentation and management in primary care: a cross-sectional analytic study in Aboriginal and Torres Strait Islander primary health care settings. International Journal of Mental Health Systems 7(1): 16. DOI: 10.1186/1752-4458-7-16.
Si, D., M. Dowden, C. Kennedy, R. Cox, L. O’Donoghue, H. Liddle et al. (2011). Indigenous community care: documented depression in patients with diabetes. Australian Family Physician 40(5): 331–3.
Titmuss, A., E. Davis, A. Brown and L. Maple-Brown (2019). Emerging diabetes and metabolic conditions among Aboriginal and Torres Strait Islander young people. Medical Journal of Australia 210(3): 111113.e1. DOI: 10.5694/mja2.13002.
Titmuss, A., E. Davis, V. O’Donnell, M. Wenitong, L. Maple-Brown, A. Haynes et al. (2022). Youth-onset type 2 diabetes among First Nations young people in northern Australia: a retrospective, cross-sectional study. Lancet. Diabetes and Endocrinology 10(1): 11–13. DOI: 10.1016/S2213-8587(21)00286-2.
Wickramasinghe, L., P. Schattner, M. Hibbert, J. Enticott, M. Georgeff and G. Russell (2013). Impact on diabetes management of general practice management plans, team care arrangements and reviews. Medical Journal of Australia 199(4): 261–5. DOI: 10.5694/mja13.10161.
World Health Organization (2021, 10 November). Diabetes: key facts. World Health Organization. https://www.who.int/news-room/fact-sheets/detail/diabetes.
1 World Health Organization 2021.
2 World Health Organization 2021.
3 Saeedi, Petersohn et al. 2019.
4 International Diabetes Federation 2021.
5 Gaskin, Thorpe et al. 2014; Naqshbandi, Harris et al. 2008.
6 Australian Institute of Health and Welfare 2015; Gaskin, Thorpe et al. 2014; Naqshbandi, Harris et al. 2008.
7 World Health Organization 2021.
8 Australian Institute of Health and Welfare 2015.
9 Australian Institute of Health and Welfare 2023.
10 Titmuss, Davis et al. 2019; Titmuss, Davis et al. 2022.
11 Durey and Thompson 2012; Ride and Burrow 2016.
12 Royal Australian College of General Practitioners 2020.
13 Remote Primary Health Care Manuals 2022.
14 Ride and Burrow 2016.
15 Royal Australian College of General Practitioners 2020.
16 Wickramasinghe, Schattner et al. 2013.
17 Matthews, Connors et al. 2015.
18 National Heart Foundation of Australia 2016.
19 Australian Chronic Disease Prevention Alliance: National Vascular Disease Prevention Alliance 2012.
20 Gabb, Mangoni et al. 2016.
21 Remote Primary Health Care Manuals 2022; Royal Australian College of General Practitioners 2020.
22 Matthews, Connors et al. 2015.
23 Schierhout, Matthews et al. 2016.
24 Diabetes Australia n.d.
25 Holt and Katon 2012.
26 Lin, Heckbert et al. 2009.
27 Holt and Katon 2012.
28 Australian Institute of Health and Welfare 2022.
29 Si, Dowden et al. 2011.
30 Schierhout, Nagel et al. 2013.
31 Menzies School of Health Research and One21seventy 2015
32 Menzies School of Health Research and One21seventy 2012.
33 Matthews, Connors et al. 2015; Schierhout, Matthews et al. 2016.
34 Matthews, Connors et al. 2015; Schierhout, Matthews et al. 2016.
35 Matthews, Connors et al. 2015; Schierhout, Matthews et al. 2016.
36 Matthews, Schierhout et al. 2014.
37 Matthews, Connors et al. 2015.
38 Matthews, Connors et al. 2015.
39 Matthews, Connors et al. 2015.
40 Matthews, Schierhout et al. 2014.
41 Matthews, Connors et al. 2015; Matthews, Schierhout et al. 2014.
42 Bailie, Matthews et al. 2017.