11
Improving preventive health care
Preventive health care
How health is defined influences how preventive care is approached. In a Western medical model, preventive care focuses on the prevention of illness to decrease disease and associated risk factors, improve health outcomes and ease demand on health services. Preventive care is crucial for reducing the burden of chronic illnesses such as type 2 diabetes and for preventing diseases such as polio and rheumatic heart disease. Preventive measures can be applied at all stages of the life span and along a disease continuum, to prevent illness and further decline in health over time. When approached in a holistic way, preventive care is tailored to the health needs of individuals, communities and populations, and supports people to manage their own health. When such opportunities are missed, it leads to increased illness in the population, higher use of hospital care, higher healthcare costs and continuing health inequities for certain groups (for example, Indigenous peoples, refugees, people with disabilities).
While the Western medical model is dominant in many parts of the world, other models and knowledges are important for preventing illness and promoting health, including in specific populations within “Western” countries. Preventive approaches grounded in Indigenous worldviews, for example, may challenge the person-centred approach prevalent in Western approaches, centralising the connections between people, their lived experiences, histories, cultures and environments that protect health and enable wellbeing.1 Chinese medicine and India’s Ayurveda centralise individualised lifestyle practices and integrated preventive strategies.2 In various approaches, good preventive care is critical in the shift towards primary health care (PHC) that reflects the values and cultures of consumers, aims for better quality of life and outcomes, and uses healthcare resources effectively.
A Western approach to preventive care is widely adopted in PHC services and defines four levels of prevention.
- Primordial prevention – action taken to prevent future hazards to health and to decrease factors known to increase disease risks. Examples are promoting healthy behaviours in childhood, improving housing and sanitation, tackling systemic racism, reducing air pollution and taking action on climate change.
- Primary prevention – aims to avoid the development of disease or disability in healthy people and generally focuses on specific risk factors for certain diseases or injuries. Examples in PHC settings are immunisation against infectious diseases (for example, childhood and Covid-19 vaccines), health education, interventions supporting behaviour change (for example, healthy eating, not smoking) and community programs to protect health (for example, by strengthening cultural practices). Primary prevention may include “passive” strategies (for example, nutrient-enriched foods) and legislation to reduce harm (for example, restricting the sale of tobacco and alcohol, mandating the use of seatbelts in vehicles).
- Secondary prevention – aims to reduce the effect of a condition or injury by detecting it and halting or slowing its progress. Examples are screening people for risk factors and early detection of diseases (for example, assessing cardiovascular risk), and interventions to reduce risks (for example, changes to diet, preventive drug therapies). Screening and early detection has limited value unless systems and resources are available to follow up people “at risk”. Providing affordable treatment is a key challenge in low-resource settings.3
- Tertiary prevention – aims to reduce the effect of an ongoing illness or an injury with lasting effects. An example is helping people to manage long-term, complex health problems (for example, chronic illness, brain injury) so their ability to function, quality of life and life expectancy are improved. Clients who need this level of preventive care have considerable contact with healthcare providers.4
Prevention and public health were elevated during the Covid-19 pandemic. Data has shown that people with preventable chronic conditions, health vulnerabilities (for example, smoking, some disabilities), poor and elderly people and those not traditionally well served by health systems (for example, Indigenous peoples, people living in rural and remote areas) are at greater risk of adverse outcomes linked to Covid-19. The data has provided evidence that more needs to be invested in keeping people healthy and reducing health inequities. 5
Clinical PHC teams generally deliver primary, secondary and tertiary prevention. A comprehensive approach to PHC addresses the clinical, social, cultural and environmental determinants of health as part of prevention and health promotion. The main focus of this chapter is the quality of preventive clinical care provided to individuals and populations, rather than the prevention of health issues from a public health, population health or health promotion perspective.
Preventive health and Aboriginal and Torres Strait Islander peoples
Preventable chronic disease is the largest contributor to the difference in health status between Aboriginal and Torres Strait Islander peoples and non-Indigenous Australians. While important gains are being made (for example, through Indigenous-led strengths-based prevention programs), two-thirds of 2018–19 National Aboriginal and Torres Strait Islander Health Survey respondents reported at least one chronic condition, and 36 per cent reported 3 or more.6 It is not the same for everyone everywhere, but overall, rates of diabetes are higher compared with non-Indigenous Australians7 and type 2 diabetes occurs at earlier ages.8 Aboriginal and Torres Strait Islander peoples are more likely to report cardiovascular disease,9 and in 2018 the burden of chronic kidney disease was almost eight times as high among First Nations people as non-Indigenous people.10 Self-reported experience of psychological distress was 2.7 times the rate of other Australians11 and rates of hospital admission for most health problems were higher.12 These health inequities provide clear evidence of the need for best-practice preventive health care with broad population coverage at all levels, and culturally safe services that build on Aboriginal and Torres Strait Islander knowledge, resilience and strengths to improve outcomes. Strong cultural, family and community connections, continuing cultural practices and a holistic approach to wellness are linked with positive health and wellbeing.13
This chapter reports on clinical preventive care. However, the social determinants of health account for a third of the health gap and result in differences in health risks, exposures, access to services and health outcomes throughout a person’s life.14 Clinical preventive care is important but does not adequately address the social determinants and further actions are needed across the health system and other sectors. Action is needed to improve poor housing, health hardware and living conditions that increase the risk of preventable conditions, including infectious diseases and chronic illnesses, for many communities.15 Tackling racism and economic exclusion,16 and supporting Aboriginal and Torres Strait Islander peoples’ rights to self-determine how services and programs are designed, delivered and managed are also essential for protecting and improving health.
Since the introduction of Medicare-funded Indigenous-specific health assessments in 1999, clinical preventive care services have been progressively expanded for Aboriginal and Torres Strait Islander peoples of all ages. There has been a substantial increase in the delivery of health assessments, but it is difficult to assess the effect of this expansion on improving health outcomes. Research shows that health assessments may not be reaching those most in need, thereby reducing the potential benefits at a population level,17 and that the rate of follow-up of health assessments has been low.18
Recommended preventive health care
A comprehensive PHC approach
Clinical preventive care should follow a life-course approach. Screening and illness prevention services for child and youth health should continue into adulthood. General prevention measures for adults are consistent with the measures identified for preventing diabetes in the previous chapter. They include community health promotion programs, identifying people at high risk using recommended assessment tools, providing client education and promoting changes that reduce health risks as needed (for example, focusing on exercise, weight reduction, diet, smoking, alcohol intake, emotional wellbeing), and appropriate therapies to reduce the effects of illness and to improve health.
Preventive health assessments and other preventive interventions
These types of interventions may be delivered opportunistically during clinical encounters in PHC settings, or through integrated approaches between PHC providers and other services (for example, breast cancer screening). Strategies for increasing the delivery of prevention services might include electronic reminders in clinical information systems when screening is due, doing health assessments incrementally over multiple sessions and offering outreach programs (for example, to deliver vaccinations in work and community settings).
Follow-up of abnormal results
PHC teams or practitioners should always plan to follow up people who have had preventive health assessments and screening, so that abnormalities found during assessments can be addressed. Clients’ social and emotional wellbeing can also be affected by the outcomes of screening, especially when a new condition is diagnosed. Counselling should be available.
Client-centred preventive care
Regardless of where or how prevention services are delivered, they should support holistic assessment of the client’s health, recognising the interdependence of many risk factors and determinants of disease. The person’s strengths and potential to change high-risk health behaviours, their health literacy, life circumstances, family and community support are considered when planning strategies to reduce health risks and provide ongoing care. Continuing engagement with PHC services needs to be encouraged. Cultural safety should be a priority, and may involve, for example, the engagement of Aboriginal and Torres Strait Islander health practitioners and other culturally specific support services.
Findings: quality of preventive care
The data presented below on the quality of preventive care come mainly from nine research papers and key reports published by the ABCD CQI research program between 2003 and 2019. Studies analysed more than 17,108 records of people aged between 15 and 55 years who had not been diagnosed with a chronic illness. The ABCD Preventive services audit tool19 was used to collect data from 137 PHC centres between 2005 and 2014 (the most recent audit data available for analysis). The majority of health centres (almost 80 per cent) were located in geographically remote locations and 73 per cent were government managed. Stakeholders participated in data interpretation to identify priority evidence-to-practice gaps and factors influencing improvement.
Comprehensive preventive care
Audit data relating to 26 best practice indicators for preventive care were brought together to analyse the overall quality of preventive health care from 2005 to 2014 (17,108 client records, 137 PHC centres).
Clinical audit and interpretation of the data from the audits found several key points for continuous quality improvement.
- Delivery of recommended preventive care varied widely between service items.20
- Clear improvements were made in overall adherence to recommended preventive care. The mean and median levels of care delivery improved from 30 to 35 per cent in 2005 to about 60 per cent in 2014 (Figure 11.1).21
- A smaller PHC centre service population was associated with greater adherence to best practice guidelines.22
- No reduction occurred in the variation in the level of preventive care delivery between health centres. Variation increased over the four consecutive audit cycles 2011–2014 (Figure 11.1).23
- Variation between PHC centres in the level of delivery of preventive care may be partly explained by community–PHC centre linkages, organisational culture, effectiveness of team structure and function, degree of staff turnover, availability of community health workers (for example, Aboriginal and Torres Strait Islander health practitioners), allied health professionals and other resources, and use of information technology systems for recall and reminders.24
- There was a small upward trend in the overall level of delivery of preventive care for services who participated in three or more CQI cycles. This suggests that a sustained commitment to CQI will result in improvements in the delivery of care for those services.25
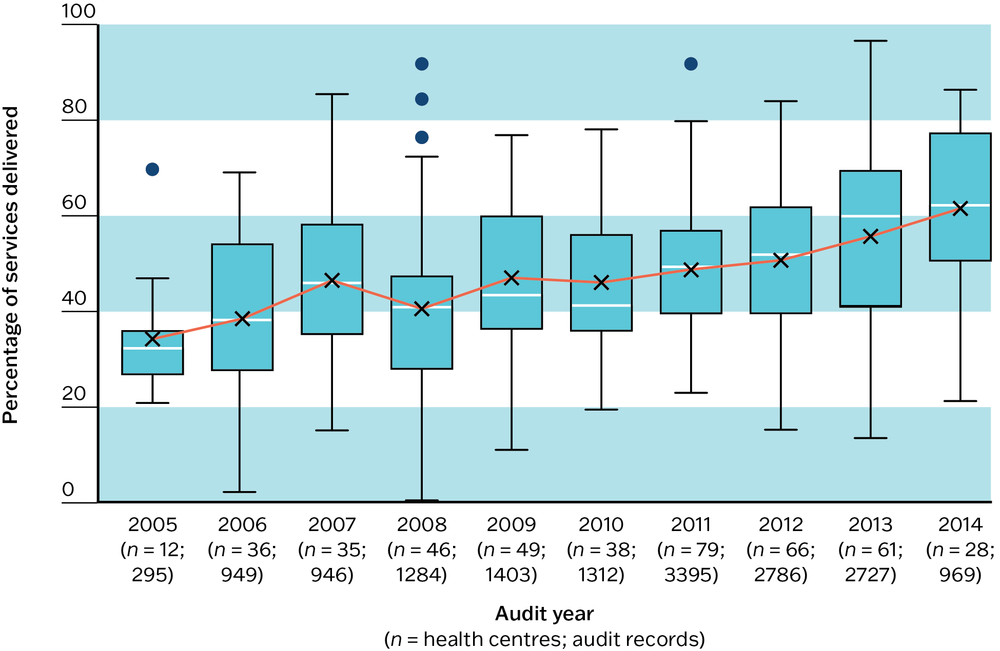
Figure 11.1 Trends in overall service delivery to well clients. Source: J. Bailie, V. Matthews et al. 2017.
Over audit years there were clear improvements in the overall service delivery of preventive health care.
Note: the overall preventive care service delivery composite figure includes these checks and measurements: of weight, waist circumference, blood pressure, urinalysis, blood glucose level, sexually transmitted infections (gonorrhoea, chlamydia and syphilis), Pap smear, oral health, nutrition, physical activity, recording of smoking and alcohol status, brief intervention if smoker or high-risk alchohol user or both.
Planning for follow-up care: abnormal clinical results
Routine preventive care involves following up clients who have abnormal results from screening tests or risk factors for disease and chronic illnesses (or both). Follow-up care may include, for example, a plan for repeat measurement or the retesting of abnormal results, and may involve medical prescriptions, counselling, and referrals to medical specialists, allied health professionals or programs that support change (for example, to stop smoking or increase physical activity) as part of a management plan.
Analysis of data (17,108 audited records, 137 PHC centres, 2005–14) showed these results:
- The highest priority for improvement was the follow-up of clients with abnormal blood pressure, blood glucose levels and lipid profiles.
- Follow-up rates remained consistently low across the years, particularly for abnormal blood glucose and lipids testing (Figure 11.2a, b and c). This represents a significant missed opportunity for improving early intervention for chronic diseases.
- There was wide variation in follow-up between PHC centres across the years. A concerning proportion of clients had no plan for follow-up. This was the case for follow-up of abnormal tests for blood pressure, blood glucose levels and lipids (Figure 11.2a, b and c).
- Only a small proportion of “well” adults had records of, or plans for, follow-up of abnormal clinical findings in 2005–09 audits.26 Audit data from 2012–14 showed similar results,27 highlighting the need for more focus on this area of preventive care.
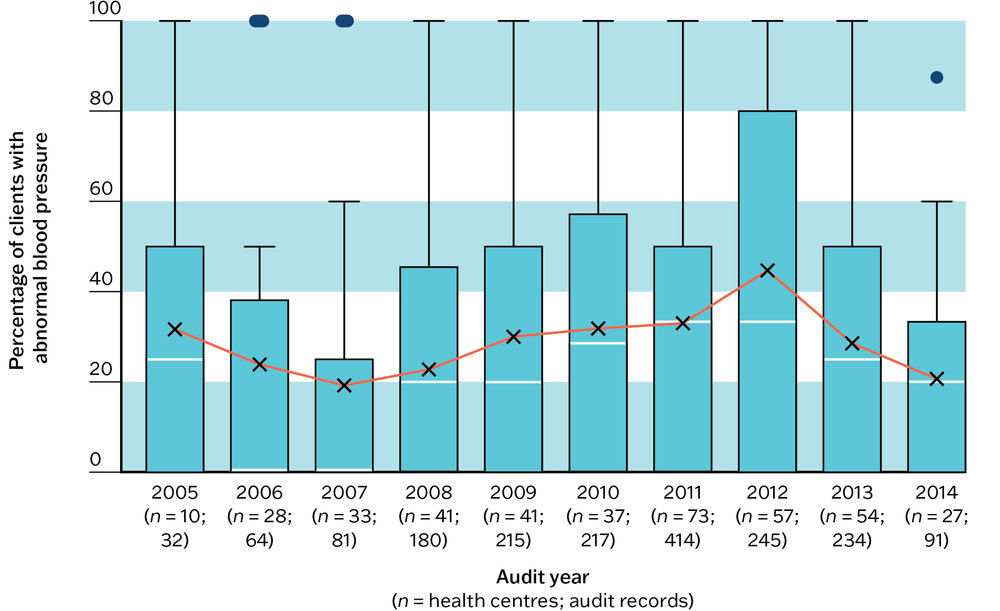
Figure 11.2a Mean health centre record of plan for follow-up by audit year for abnormal blood pressure. Source: J. Bailie, Matthews et al. 2017.
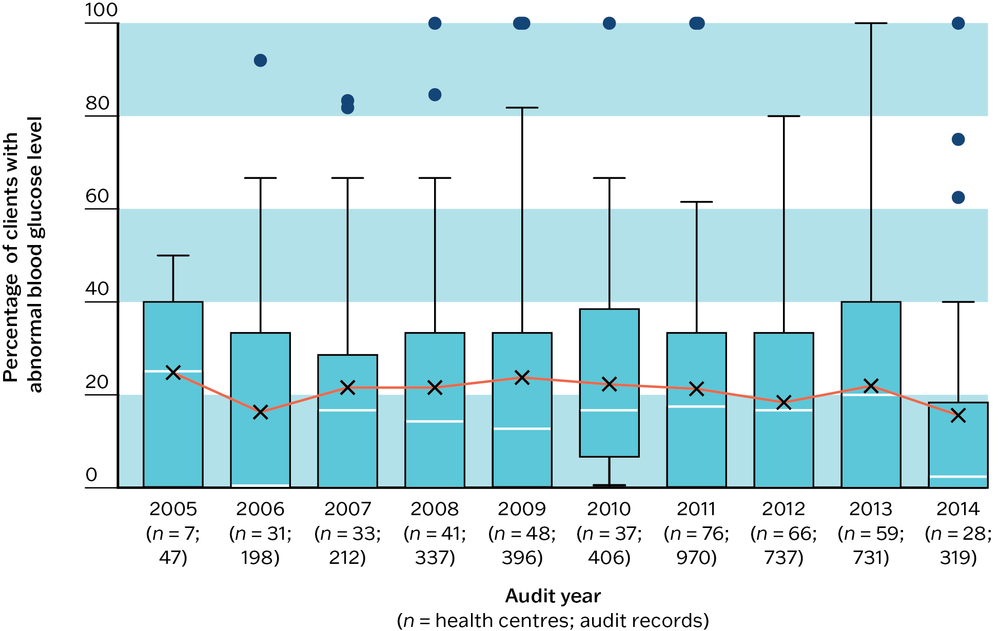
Figure 11.2b Mean health centre record of plan for follow-up by audit year for abnormal blood glucose level. Source: J. Bailie, Matthews et al. 2017.
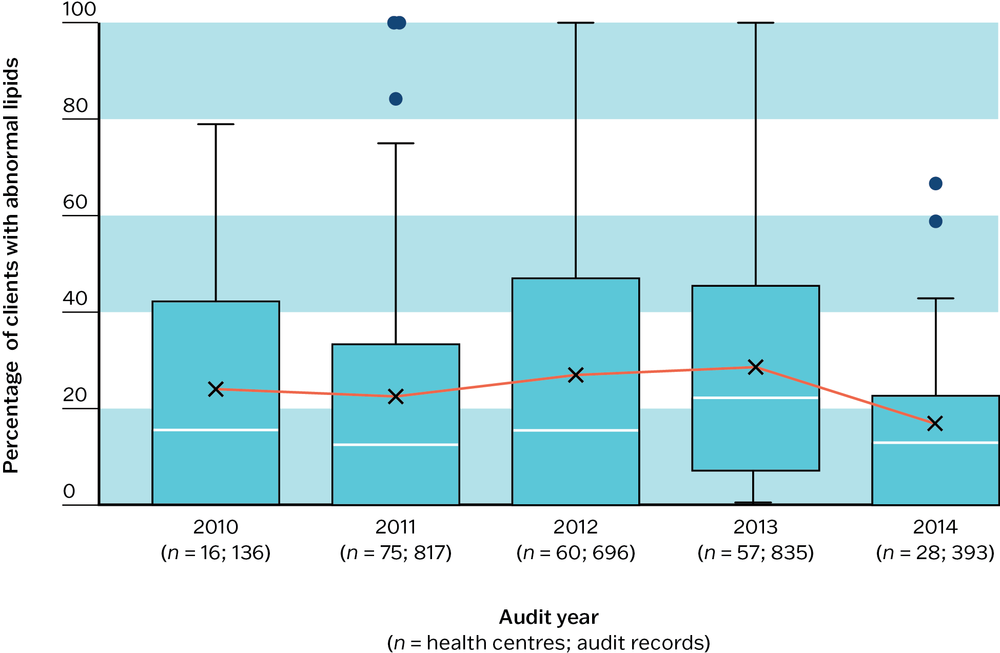
Figure 11.2c Mean health centre record of plan for follow-up by audit year for abnormal lipid profile. Source: J. Bailie, Matthews et al. 2017.
Emotional wellbeing screening, support and follow-up
Screening for emotional wellbeing and following best-practice pathways for those at risk are important parts of preventive care. They are particularly important for population groups experiencing high rates of illness and trauma, social and economic exclusion, or displacement.
Recommended care includes use of standard screening tools for emotional wellbeing (for example, Kessler 10; Patient Health Questionnaire 9). Social and emotional wellbeing assessment tools that have been culturally validated for use with Aboriginal and Torres Strait Islander adults include the Patient Health Questionnaire 9,28 the Aboriginal Resilience and Recovery Questionnaire,29 the Aboriginal and Islander Mental Health Initiative Northern Territory,30 and the Here and Now Aboriginal Assessment.31 Formal and informal discussions about emotional wellbeing (for example, guided by culturally specific resources32) can also be used to assess risk; discussions should be documented in client records. Options for follow-up action with clients assessed as at risk may include brief interventions, counselling, cognitive behaviour therapy, medication, strengths-based Indigenous programs (for example, Family Wellbeing Empowerment Program), and other types of support such as referral to housing and employment services.
There is a need to increase rates of emotional wellbeing screening, and to improve the ability of PHC services to provide appropriate support and follow-up for clients identified as being at risk, as part of preventive care.
- Analysis of audit data (3,571 client records, 95 PHC centres, 2012–14) found wide variation between PHC centres in the use of standard tools to assess emotional wellbeing, but low levels generally. In the majority of PHC centres this was being done for fewer than 20 per cent of clients.
- A small proportion of clients – less than 10 per cent in the majority of PHC centres – had a record of concern of being at risk for emotional wellbeing, but this is as high as 40 to 60 per cent in a few PHC centres.
- For clients assessed as being at risk, there was wide variation between PHC centres in referral or in provision of brief interventions, counselling or psychotropic medication, and no evidence of improvement in delivery of these follow-up services over time (Figure 11.3a, b and c).33
- Recording a subsequent review of clients who had been identified at risk, or having a report from an external service as a result of a referral, also varied widely between PHC centres.
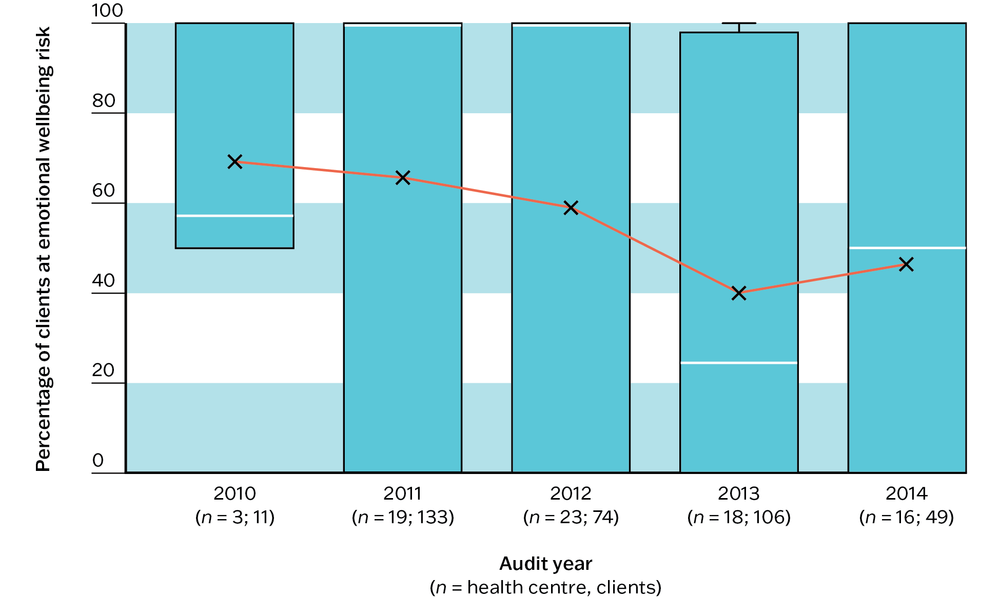
Figure 11.3a Mean health centre percentage (by audit year) of clients identified at social and emotional wellbeing risk using a standard tool, with a record of follow-up action: brief intervention. Source: J. Bailie, Matthews et al. 2017.
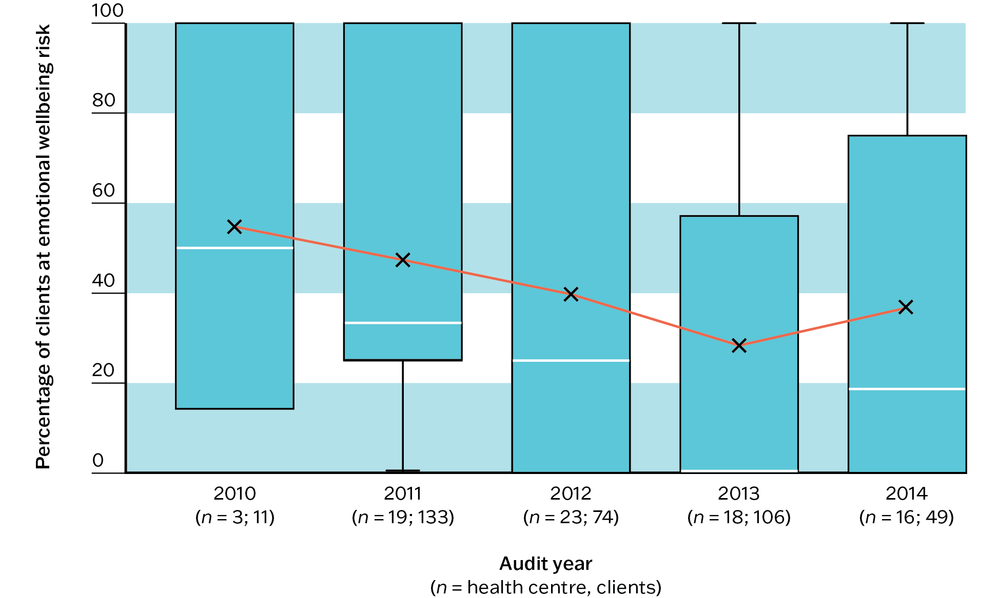
Figure 11.3b Mean health centre percentage (by audit year) of clients identified at social and emotional wellbeing risk using a standard tool, with a record of follow-up action: counselling. Source: J. Bailie, Matthews et al. 2017.
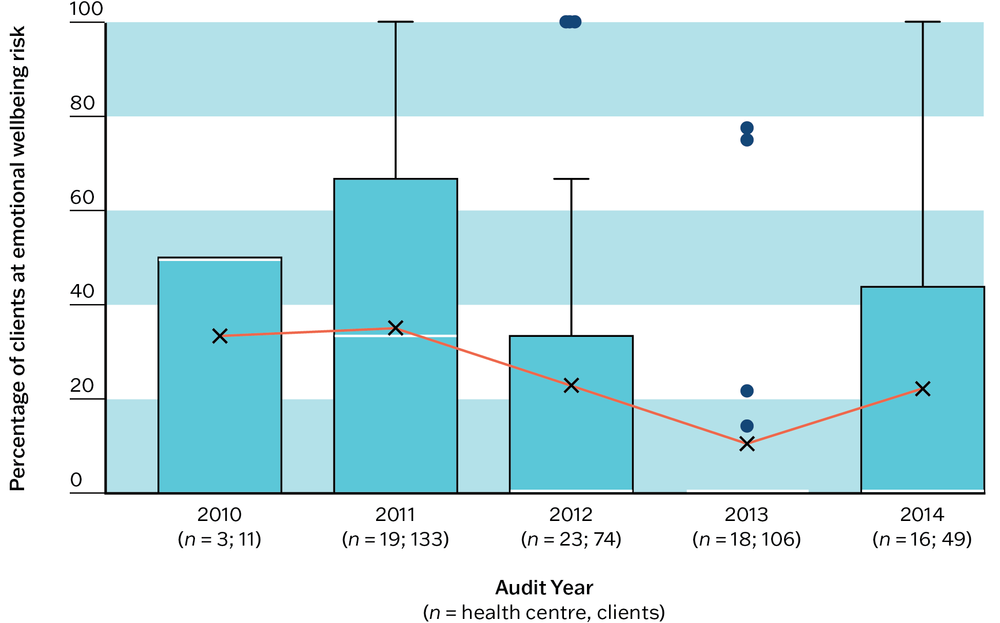
Figure 11.3c Mean health centre percentage (by audit year) of clients identified at social and emotional wellbeing risk using a standard tool, with a record of follow-up action: medication review. Source: J. Bailie, Matthews et al. 2017.
Preventive health assessments
Best-practice guidelines for preventive health assessments for Aboriginal and Torres Strait Islander peoples include indicators of health risk across 17 topics: lifestyle; antenatal care; child health; health of young people; health of older people; eye health; hearing; oral health; respiratory health; acute rheumatic fever and rheumatic heart disease; cardiovascular disease; type 2 diabetes; kidney health; sexual health; cancer; family abuse; and mental health.34 The focus of this chapter is preventive care for generally well adults. Separate ABCD CQI tools and processes are used to audit preventive health assessments for children and antenatal care (see Chapters 12 and 13.)
Preventive health assessments for adults were delivered at low levels. In the 2012–14 audit data, the mean rate of assessment using the recommended Adult Health Check assessment tool (Australian Medicare Benefits Schedule rebate item number 715) was just over 20 per cent and use of an alternative health check tool was even lower. The proportion of eligible clients receiving recommended preventive care ranged from 18 per cent to 85 per cent for individual preventive services.35 Audit data showed that some aspects of screening and support for preventive care were being provided and documented at high levels by health centres. There was relatively better recording of these elements of care:
- up-to-date health summaries and immunisation records
- measurement of weight
- measurement of blood glucose level
- measurement of blood pressure, pulse rate and rhythm
- delivery of brief interventions for clients identified as drinking alcohol at high-risk levels, and for tobacco use.36
Better recording of care was needed for these elements:
- completing cardiovascular risk assessments – the mean across 92 health centres from 2012–2014 was 20 per cent
- urinalysis – the median level of delivery (95 PHC centres, 2012–14) was approximately 50 per cent
- lipid profile – the median level of delivery (95 PHC centres, 2012–14) was approximately 40 per cent
- inquiry or brief intervention about environmental and living conditions, family relationships and substance abuse – median rates for all three items ranged from 20 per cent to just over 30 per cent
- emotional wellbeing screening and support for clients identified as being at risk37
- oral health checks.38
Across the studies, there was a need to strengthen systems and processes to support preventive care. Stakeholder input to data interpretation identified drivers and strategies for system improvement, as follows:
- strong community participation in the local PHC service (for example, improve staff understanding of the culture, diversity and main features of the local population, involve community members in health service governance)
- appropriate PHC team structure and function to provide preventive care (for example, allocate resources and roles for preventive care with targeted recruitment; provide training, including to supporting client self-management; improve teamwork; establish links with other care providers for referral and care continuity)
- effective service delivery structures and supports (for example, adequate and flexible funding models for preventive care, incentives for delivering health assessments, employment of local community members in the PHC service)
- well-functioning clinical information systems and decision support tools (for example, adjust clinical information systems as needed to recall clients for health assessments and follow-up, record test results and follow-up action, calculate cardiovascular risk)
- PHC teams trained in using clinical information systems and documenting preventive care in client records
- use of data for CQI in preventive care (for example, allocate time and resources for CQI, bring in technical help to extract and interpret data if needed, plan and review improvement)
- improved client health literacy and strong links between preventive care and community health promotion programs.
Key messages for improving preventive health care
Patterns of preventive healthcare delivery in Aboriginal and Torres Strait Islander PHC communities are likely to reflect, at least to some extent, care delivery in international settings. This CQI research identifies clear priorities and strategies for improving preventive health care.
There are common evidence-to-practice gaps in preventive care that call for system-wide and local attention:
- planning for follow-up of clients with abnormal blood pressure, blood glucose levels and lipid profile
- completing cardiovascular risk assessments
- recording of urinalysis and lipid profiles
- recording of inquiry about environmental and living conditions, family relationships and substance use
- providing appropriate support and follow-up for clients identified as being at risk with respect to emotional wellbeing
- strengthening “PHC team structure and function” and “continuity of care”.
There is a need to focus on the main drivers of best practice preventive care. These are the most important:
- strong community participation in the local PHC service
- appropriate PHC team structure and function to provide preventive care
- effective service delivery structures and supports
- well-functioning clinical information systems and decision support tools
- PHC teams trained in using clinical information systems and documenting preventive care in client records
- use of data for CQI in preventive care
- improved client health literacy and strong links between preventive care and community health promotion programs.
All involved in preventive care should aim to spread and continue improvement:
- taking action to improve systems for delivering preventive care will strengthen other areas of care (for example, chronic illness care)
- sustained commitment to CQI is needed to achieve and sustain improvement.
Sustained commitment to CQI is needed to achieve and sustain improvement.
Improving preventive care in Aboriginal and Torres Strait Islander PHC
Improving the delivery of preventive care for Indigenous Australians is crucial to closing the health gap between Aboriginal and Torres Strait Islander and non-Indigenous Australians. Despite efforts to improve preventive care at the PHC level and national policy initiatives, recommended best-practice preventive care is not consistently provided. Our research into the quality of preventive care for Aboriginal and Torres Strait Islander peoples since 2005 highlights major gaps in the delivery of recommended preventive care, particularly the recording of care provided, and a lack of follow-up of abnormal clinical findings. While many aspects of preventive care are being done well in many health centres, these common gaps and the persistent wide variation between health centres in the delivery of preventive services indicate deficiencies in the broader PHC system.39
This evidence reinforces the critical importance of taking both system-level and local action to improve preventive care, including effective processes for engaging Aboriginal and Torres Strait Islander communities in planning and delivering preventive services. There is need for, firstly, prevention activities based on needs identified by clients and communities; secondly, close collaboration between health promotion staff and clinicians within PHC teams; and, finally, a multi-sector, systems-wide approach that involves multiple service agencies and focuses the attention of funders towards all levels of prevention. A health system aimed at reducing the increasing burden of disease, reducing health inequity and preparing for emerging health threats will serve all Australians well.40
A health system aimed at reducing the increasing burden of disease, reducing health inequity and preparing for emerging health threats will serve all Australians well.
Medicare rebates for annual preventive health assessments are available for all Aboriginal and Torres Strait Islander peoples of any age through the Medicare Benefits Schedule rebate item number 715. The rate of Aboriginal and Torres Strait Islander peoples who received an Indigenous-specific health check stabilised around 28 per cent in 2023, with people 65 years and older having the highest rates of health checks (42 per cent of the population in 2023), compared with 15- to 34-year-olds at 23 per cent. Older people also had the highest rates of follow-up (56 per cent), and women had higher rates of health checks and follow-up than men across all adult age groups.41 The earlier onset of chronic diseases among the Aboriginal and Torres Strait Islander population indicates an urgent need to target younger people for health checks, and to increase the delivery of health assessments overall, as part of a holistic approach to PHC.
A key factor in improving preventive care for Aboriginal and Torres Strait Islander clients is the availability of appropriate services for client referral. Remote practitioners may reasonably be reluctant to carry out services such as visual acuity testing and oral health checks where there are limited options for referral for treatment. Client care can also be compromised in urban settings if services make strategic decisions to increase service remuneration through Medicare-funded health assessments without adequate resources to provide follow-up care.42
Our studies indicate that PHC teams generally know the content and objectives of best-practice preventive healthcare delivery, but high demand for acute care, competing demands on staff time and inadequate staffing levels in PHC services present barriers to delivering preventive care. This is borne out in audit data, which show that 48 per cent of clients last attended their health service for acute care and only 11 per cent for a preventive health assessment. Dedicated preventive care resources, workflow strategies that enable delivery of preventive care and clear role definitions help PHC teams to provide recommended preventive services.43 Clinical services need to complement community-led programs that use strengths-based and culturally based approaches to protect health. CQI offers opportunities to reflect on the context in which PHC is operating and to seek input from different stakeholders about how to improve care. It provides data that can be used to advocate for public health measures and policy change.
The upward trend in overall delivery of preventive care for services that participated in three or more CQI cycles suggests that a sustained commitment to CQI will result in improvements in the delivery of care for those services.44 At higher levels of the health system, policy and infrastructure support and organisational commitment to CQI have been associated with steady improvements or maintenance of high-quality preventive care for Aboriginal and Torres Strait Islander communities.45
Policy and infrastructure support and organisational commitment to CQI have been associated with steady improvements in preventive care.
References
Australian Institute of Health and Welfare (2024a). Aboriginal and Torres Strait Islander Health Performance Framework: summary report August 2024. Canberra: AIHW. https://www.indigenoushpf.gov.au/report-overview/overview/summary-report.
Australian Institute of Health and Welfare (2024b) Australia’s health 2024: health and wellbeing of First Nations people. Canberra: Australian Government. https://www.aihw.gov.au/reports/australias-health/indigenous-health-and-wellbeing.
Australian Institute of Health and Welfare (2024c). Chronic kidney disease: Australian facts. Cat. no. CDK 2024. Canberra: AIHW. https://www.aihw.gov.au/reports/chronic-kidney-disease/chronic-kidney-disease/contents/about.
Australian Institute of Health and Welfare (2024d). Diabetes. Cat. no. CVD 96. Canberra: Australian Government. https://www.aihw.gov.au/reports/diabetes/diabetes/contents/summary.
Australian Institute of Health and Welfare (2024e). Health checks and follow-ups for Aboriginal and Torres Strait Islander people. Cat. no. IHW 209 https://www.aihw.gov.au/reports/indigenous-australians/indigenous-health-checks-follow-ups/contents/summary.
Australian Institute of Health and Welfare (2018). Australia’s health 2018. Cat. no. AUS 221. Canberra: AIHW.
Bailie, C., V. Matthews, J. Bailie, P. Burgess, K. Copley, C. Kennedy et al. (2016). Determinants and gaps in preventive care delivery for Indigenous Australians: a cross-sectional analysis. Frontiers in Public Health 4: 34. DOI: 10.3389/fpubh.2016.00034.
Bailie, J., V. Matthews, A. Laycock, R. Schultz and R. Bailie (2016). Preventive health care for Aboriginal and Torres Strait Islander people: final report. ESP Project: Priority Evidence-Practice Gaps and Stakeholder Views on Barriers and Strategies for Improvement. Brisbane: Menzies School of Health Research.
Bailie, J., V. Matthews, A. Laycock, R. Schultz, C. Burgess, D. Peiris et al. (2017). Improving preventive health care in Aboriginal and Torres Strait Islander primary care settings. Globalization and Health 13(1). DOI: 10.1186/s12992-017-0267-z.
Bailie, J., G. Schierhout, M. Kelaher, A. Laycock, N. Percival, L. O’Donoghue et al. (2014). Follow-up of Indigenous-specific health assessments – a socioecological analysis. Medical Journal of Australia 200(11): 653–7. DOI: 10.5694/mja13.00256.
Bailie R., J. Griffin, M. Kelaher, T. McNeair, N. Percival, A. Laycock et al. (2013). Sentinel sites evaluation: final report. Canberra: Report prepared by Menzies School of Health Research for the Australian Government Department of Health.
Bailie, R., V. Matthews, S. Larkins, S. Thompson, P. Burgess, T. Weeramanthri et al. (2017). Impact of policy support on uptake of evidence-based continuous quality improvement activities and the quality of care for Indigenous Australians: a comparative case study. BMJ Open 7(10). DOI: 10.1136/bmjopen-2017-016626.
Bailie, R., D. Si, C. Connors, R. Kwedza, L. O’Donoghue, C. Kennedy et al. (2011). Variation in quality of preventive care for well adults in Indigenous community health centres in Australia. BMC Health Services Research 11: 139. DOI: 10.1186/1472-6963-11-139.
Bodeker, G. (2020). Asian traditions of wellness: background paper. Asian Development Outlook 2020 Update: Wellness in Worrying Times. Manila: Asian Development Bank.
Crinall, B., J. Boyle, M. Gibson-Helm, D. Esler, S. Larkins and R. Bailie (2017). Cardiovascular disease risk in young Indigenous Australians: a snapshot of current preventive health care. Australian and New Zealand Journal of Public Health 41(5): 460–6. DOI: 10.1111/1753-6405.12547.
Department of Health (2021). National Preventive Health Strategy 2021–2030. Canberra: Commonwealth of Australia.
Dudgeon, P., M. Wright, Y. Paradies, D. Garvey and I. Walker (2014). Aboriginal social, cultural and historical contexts. In Working Together: Aboriginal and Torres Strait Islander Mental Health and Well-being Principles and Practice. Dudgeon P., Milroy H. and Walker R. Canberra: Commonwealth Government 3–24.
Durey, A. and S. Thompson (2012). Reducing the health disparities of Indigenous Australians: time to change focus. BMC Health Services Research 12: 151. DOI: 10.1186/1472-6963-12-151.
Gee, G. (2016). Resilience and recovery from trauma among Aboriginal help seeking clients in an urban Aboriginal community controlled organisation. PhD thesis, University of Melbourne.
Getting it Right Collaborative Group, M. Hackett, A. Teixeira-Pinto, S. Farnbach, N. Glozier, T. Skinner et al. (2019). Getting it Right: validating a culturally specific screening tool for depression (aPHQ- 9) in Aboriginal and Torres Strait Islander Australians. Medical Journal of Australia 211(1): 24–30. DOI: 10.5694/mja2.50212.
Heke, I., D. Rees, B. Swinburn, R.T. Waititi and A. Stewart (2018). Systems thinking and indigenous systems: native contributions to obesity prevention. AlterNative: An International Journal of Indigenous Peoples 15(1): 22–30. DOI: 10.1177/1177180118806383.
Institute for Work and Health (2015). What researchers mean by primary, secondary and tertiary prevention. https://www.iwh.on.ca/what-researchers-mean-by/primary-secondary-and-tertiary-prevention.
Janca, A., Z. Lyons, S. Balaratnasingam, D. Parfitt, S. Davison and J. Laugharne (2015). Here and Now Aboriginal Assessment: background, development and preliminary evaluation of a culturally appropriate screening tool. Australasian Psychiatry 23(3): 287–92. DOI: 10.1177/1039856215584514.
Menzies School of Health Research (n.d). Resources. Menzies School of Health Research. https://www.menzies.edu.au/Resources.
Menzies School of Health Research and One21seventy (2013). Preventive services clinical audit tool. Brisbane: Menzies School of Health Research.
National Aboriginal Community Controlled Health Organisation and Royal Australian College of General Practitioners (2024). National guide to a preventative health assessment for Aboriginal and Torres Strait Islander people, 4th edn. Melbourne: RACGP.
Oti, S., S. van de Vijver, G. Gomez, C. Agyemang, T. Egondi, C. Kyobutungi et al. (2016). Outcomes and costs of implementing a community-based intervention for hypertension in an urban slum in Kenya. Bulletin of the World Health Organization 94(7): 501–09. DOI: 10.2471/BLT.15.156513.
Ride, K. and S. Burrow (2016). Review of diabetes among Aboriginal and Torres Strait Islander people. Australian Indigenous HealthInfoNet. Western Australia: Edith Cowan University.
Russell, L. (2010). Indigenous health checks: a failed policy in need of scrutiny. Menzies Centre for Health Policy: University of Sydney. https://ses.library.usyd.edu.au/bitstream/2123/11447/1/atsihealthchecks2.pdf.
Si, S., J. Moss, T. Sullivan, S. Newton and N. Stocks (2014). Effectiveness of general practice-based health checks: a systematic review and meta-analysis. British Journal of General Practice 64(618): e47–e53. DOI: 10.3399/bjgp14X676456.
Titmuss, A., E. Davis, A. Brown and L. Maple-Brown (2019). Emerging diabetes and metabolic conditions among Aboriginal and Torres Strait Islander young people. Medical Journal of Australia 210(3). DOI: 10.5694/mja2.13002
Verbunt, E., J. Luke, Y. Paradies, M. Bamblett, C. Salamone, A. Jones et al. (2021). Cultural determinants of health for Aboriginal and Torres Strait Islander people – a narrative overview of reviews. International Journal for Equity in Health 20(1): 1–181. DOI: 10.1186/s12939-021-01514-2.
Wellmob (n.d.). Wellmob: healing our way. Social, emotional and cultural wellbeing online resources for Aboriginal and Torres Strait Islander people. https://wellmob.org.au.
World Health Organization (2020). Health promotion and disease prevention through population-based interventions, including action to address social determinants and health inequity. http://www.emro.who.int/about-who/public-health-functions/health-promotion-disease-prevention.html.
Yashadhana, A., N. Pollard-Wharton, A. Zwi and B. Biles (2020). Indigenous Australians at increased risk of COVID-19 due to existing health and socioeconomic inequities. Lancet Regional Health. Western Pacific 1: 100007-07. DOI: 10.1016/j.lanwpc.2020.100007.
1 Durey and Thompson 2012; Heke, Rees et al. 2018.
2 Bodeker 2020.
3 Oti, van de Vijver et al. 2016.
4 Institute for Work and Health 2015; World Health Organization 2020.
5 Department of Health 2021; Yashadhana, Pollard-Wharton et al. 2020.
6 Australian Institute of Health and Welfare 2024b.
7 Australian Institute of Health and Welfare 2024d.
8 Titmuss, Davis et al. 2019.
9 Australian Institute of Health and Welfare 2024a.
10 Australian Institute of Health and Welfare 2024c.
11 Australian Institute of Health and Welfare 2018; Dudgeon, Wright et al. 2014.
12 Australian Institute of Health and Welfare 2024a.
13 Verbunt, Luke et al. 2021.
14 Australian Institute of Health and Welfare 2018.
15 Verbunt, Luke et al. 2021.
16 Durey and Thompson 2012; Ride and Burrow 2016.
17 J. Bailie, Schierhout et al. 2014; R. Bailie, Griffin et al. 2013; Russell 2010; Si, Moss et al. 2014.
18 J. Bailie, Schierhout et al. 2014; R. Bailie, Griffin et al. 2013.
19 Menzies School of Health Research and One21seventy 2013.
20 C. Bailie, Matthews et al. 2016.
21 J. Bailie, Matthews et al. 2016.
22 C. Bailie, Matthews et al. 2016.
23 J. Bailie, Matthews et al. 2016.
24 C. Bailie, Matthews et al. 2016.
25 J. Bailie, Matthews et al. 2016.
26 R. Bailie, Si et al. 2011.
27 J. Bailie, Matthews et al. 2016.
28 Getting it Right Collaborative Group, Hackett et al. 2019.
29 Gee 2016.
30 Download Aboriginal and Islander Mental Health Initiative (AIMhi) resources from Menzies School of Health Research n.d.
31 Janca, Lyons et al. 2015.
32 Such as resources available from Wellmob n.d.
33 J. Bailie, Matthews et al. 2017.
34 National Aboriginal Community Controlled Health Organisation and Royal Australian College 2024.
35 C. Bailie, Matthews et al. 2016.
36 C. Bailie, Matthews et al. 2016; J. Bailie, Matthews et al. 2016; J. Bailie, Matthews et al. 2017.
37 J. Bailie, Matthews et al. 2016; J. Bailie, Matthews et al. 2017.
38 R. Bailie, Si et al. 2011.
39 C. Bailie, Matthews et al. 2016; J. Bailie, Matthews et al. 2016; J. Bailie, Matthews et al. 2017; R. Bailie, Si et al. 2011; Crinall, Boyle et al. 2017.
40 Department of Health 2021.
41 Australian Institute of Health and Welfare 2024e.
42 C. Bailie, Matthews et al. 2016.
43 J. Bailie, Matthews et al. 2016; J. Bailie, Matthews et al. 2017.
44 J. Bailie, Matthews et al. 2016.
45 J. Bailie, Matthews et al. 2017.