12
Improving child health
Children’s health
There is strong evidence of the vital role of health care in the early years to ensure that health throughout the life course is the best it can be.1 Primary health care (PHC) can play an important role, particularly during pregnancy when the foundations are laid and in the early years that set the beginning of health trajectories that may be difficult to shift.2
Over the past quarter century, child mortality globally has more than halved, yet in 2018 an estimated 6.2 million children and adolescents under the age of 15 years died, mostly from preventable causes. Of these deaths, 5.3 million occurred in the first five years of life, with almost half of these in the first month of life. Among the leading causes of death are congenital anomalies, pneumonia, diarrhoea and malaria. More than half of early child deaths are preventable or can be treated with simple, affordable interventions including immunisation, adequate nutrition, safe water and food, and appropriate health care.3
High-quality preventive care for babies and children should begin a continuum of preventive PHC services that extends into youth and adulthood. Good preventive care in childhood can have long-term positive effects on individual and population health, and focuses on increasing protective factors and reducing risks that affect children’s health and wellbeing. It involves monitoring growth and development, decreasing the risk of diseases (for example, through immunisation, prompt treatment of infection or illness and education to prevent chronic illnesses in adulthood), early identification and referral for children and families who need targeted specialist services, and protecting children who are at risk (for example, from poverty, violence or abuse). Holistic child health care also involves acute care and general clinical management of health and wellbeing needs.
Globally, 10 to 15 per cent of all children and 40 per cent of disadvantaged children under five years of age are estimated to have developmental problems that affect their long-term social, emotional and educational outcome.4 These developmental problems may be experienced in fine or gross motor skills, communication, play, speech, language, hearing, vision, learning and cognition. In many places, PHC staff are the only service providers who reach young children and their families. Globally, PHC staff provide more than 90 per cent of health care for families during a child’s first five years of life and are in a unique position to improve child developmental outcomes through early detection and management of developmental problems.5
Child health screening and intervention in PHC settings require that health professionals have access to concise, context-specific, evidence-based clinical guidance and continuously evaluate their practice against it.6 Effective delivery systems and resources to follow up at-risk children and their families, and provide interventions when needed, are also essential. These are key challenges for improving child health, particularly in settings with a low level of resources.
PHC staff are in a unique position to improve child developmental outcomes.
Health of Aboriginal and Torres Strait Islander children
Aboriginal and Torres Strait Islander families and communities have taken important action to achieve improvements in children’s health and wellbeing, and there are positive trends in measures for birth weight, infant mortality, early childhood education, ear health, and basic skills for life and learning.7 The proportion of mothers who smoke at any time during pregnancy fell from 52 per cent in 2009 to 44 per cent in 2019.8 Indigenous children were first to reach the target of 95 per cent for national immunisation coverage.9 In 2022, 99 per cent of Indigenous children were enrolled in a preschool program in the year before full-time schooling age and the percentage of Indigenous children completing the final year of secondary school has improved.10
In addition to families and carers, many people and organisations are working to enable Aboriginal and Torres Strait Islander children to grow up healthy, happy and safe, but significant health inequities persist. There was little improvement in the Aboriginal and Torres Strait Islander infant mortality rate in the decade to 201911 and no improvement in the percentage of children assessed as being developmentally on track between 2018 (baseline) and 2021.12 While rates of ear disease among Aboriginal and Torres Strait Islander children are decreasing, the 2018–19 National Aboriginal and Torres Strait Islander Health Survey found 3 in 10 (29 per cent) children aged 7–14 had measurable hearing loss.13 In 2014–15, among Indigenous children aged 4–14 years, 67 per cent had experienced at least one significant stressor in the previous 12 months.14
In addition to families and carers, many people and organisations are working to enable Aboriginal and Torres Strait Islander children to grow up healthy, happy and safe.
A limitation of data about Aboriginal and Torres Strait Islander children’s health is that much data comes from remote communities, whereas most Indigenous children live in urban settings.15 Living in remote areas also presents particular health challenges. For example, a relatively recent study across six Aboriginal communities in northern Australia found 42 per cent of children aged 6–24 months were anaemic.16 Anaemia is linked with poor cognitive development and educational outcomes,17 and is caused mainly by iron deficiency, and by poverty, poor environmental conditions and chronic infection. Social and environmental factors also underlie the development of acute rheumatic fever (ARF) in childhood – the incidence of ARF and rheumatic heart disease in some Aboriginal and Torres Strait Islander communities is among the highest documented globally (see Chapter 17). Trachoma persists among children living in at-risk areas (Chapter 19). A high proportion of children living in remote communities experience chronic otitis media in their developmental years, which causes hearing loss that is associated with developmental delays and effects on education outcomes. Education, social, environmental and clinical interventions are needed to improve children’s health in these settings, as part of comprehensive PHC.18
Indigenous Australians experience widespread socio-economic challenges. Aboriginal and Torres Strait Islander children are over-represented in the homelessness, child protection and youth justice systems.19 These factors link directly to the trauma of colonisation, racism and oppression, and highlight the importance of tackling the social and structural determinants of health. They also highlight the resilience of Aboriginal and Torres Strait Islander communities. A 2016 study of factors linked with good mental health among 1,005 urban Aboriginal children aged 4–17 years in New South Wales found 72 per cent were not at high risk for emotional or behavioural problems. Healthy eating, not suffering from frequent infections and having a carer who was not highly psychologically distressed were contributing factors, while being raised in foster care or in four or more homes since birth increased risk.20 A study of 725 urban Aboriginal children younger than 8 years found 32 per cent were at high, 28 per cent at moderate, and 40 per cent at low or no developmental risk.21
Policy initiatives such as “Closing the Gap”,22 Commonwealth funding under the Medical Benefits Scheme for health checks23 for Aboriginal and Torres Strait Islander peoples, improvement in data surveillance systems and use of CQI are important for monitoring and improving child health. Regardless of the setting or circumstances in which children live, high-quality PHC with integrated service approaches and strengths-based, community-led responses that affirm cultural connections are needed for improving child health and wellbeing.24
Findings: quality of child health care
Comprehensive child health care includes prevention, detection of developmental problems, early intervention, care and support for children living in a range of geographical settings and circumstances. On-target child growth and development are important signs that a child is physically, emotionally, culturally and spiritually healthy. Important information to track a child’s development includes a growth chart and a current completed health check. For example, the Australian government advises PHC providers to administer a “child health check” annually to each Indigenous child across the country. Child health checks are used to plan and track the management of care, through regular checking of risk factors, scheduled services, required pathology tests, immunisations and specialist care, brief interventions and conversations with the family and child about health and wellbeing. These items, episodes of acute care, management of illnesses and disabilities, and referrals are documented in a child’s health record to provide an overall picture of the care delivered. PHC services should use a recall system for recommended child health checks, immunisations, follow-up of abnormal results and treatments.
The data presented below on the quality of care provided to children come mainly from 14 research papers and key reports published by the ABCD CQI research program between 2008 and 2018. Studies analysed more than 10,405 records of children aged between 3 months and 15 years, and 265 systems assessments completed by PHC teams. Audit data were collected from 132 PHC centres between 2007 and 2013. Stakeholders participated in data interpretation to identify priority evidence-to-practice gaps and factors influencing improvement.
Comprehensive PHC for children
The ABCD child health audit tool25 (see Table 12.2) was used to collect data about the delivery of child health services, to assess the quality of overall adherence to child health care in accordance with best-practice guidelines. Over five consecutive audit cycles these findings were made:
- significant improvements in quality of care, which appear to be related to PHC services participating in regular CQI activities26
- evidence of improvement for most indicators, including overall child health care; measles, mumps and rubella vaccination at 4 years; clinical examinations (recording of weight, ear checks, developmental milestones); follow-up of children with growth faltering; records of advice, brief interventions and improvement in health centre systems27
- reduced variation between PHC centres for most indicators, including overall child health, most clinical examinations, and health centre systems assessment scores28
- no clear evidence of improvement in having immunisation charts in children’s health files, or a record of a haemoglobin check or follow-up of children with anaemia29
- no reduction in variation for recording of Hepatitis B immunisation at birth, haemoglobin check or follow-up of children with anaemia.30
Figure 12.1 shows trends in the quality of overall child health service delivery, based on 10 indicators or items of care: weight, height, head circumference, hip exam, testes check, ear exam, breastfeeding, nutrition advice, sudden infant death syndrome prevention, and developmental check. Successive audit cycles showed evidence of improvement for overall child health care, and variation in the delivery of child health services reduced between health centres. There was also less variation across health centres in the fourth and fifth audit cycles; PHC centres with the lowest levels of overall delivery of care improved their performance.31
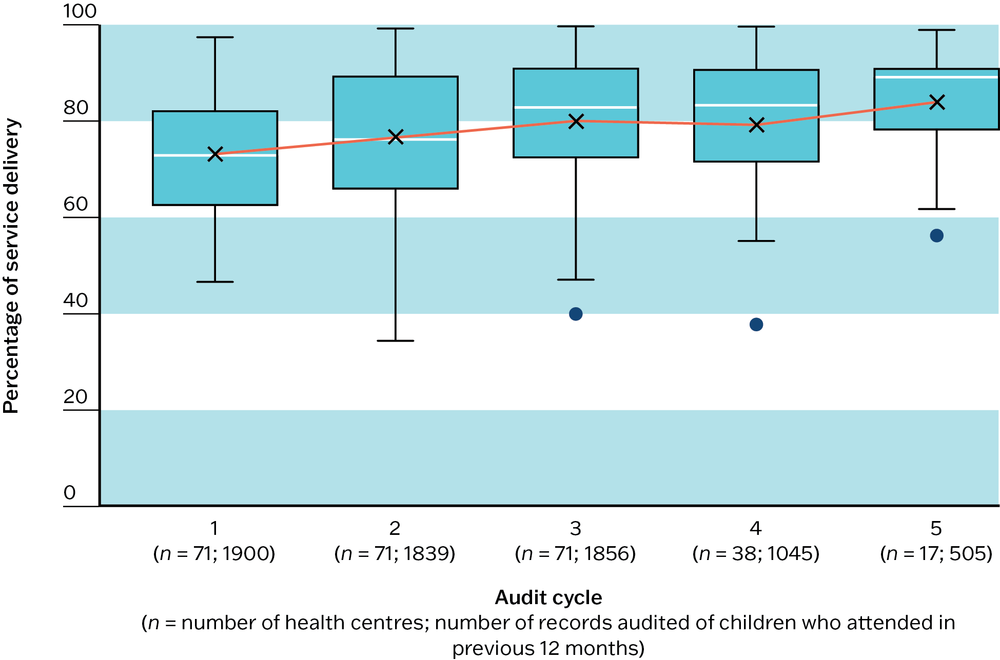
Figure 12.1 Trends in overall child health service delivery. Source: R. Bailie, Matthews et al. 2014.
Monitoring and recording of growth and development measures and follow-up of abnormal findings
Growth and development checks should be delivered at specific ages and intervals, according to guideline-recommended care.32 For example, screening guidelines for Aboriginal and Torres Strait Islander children recommend that weight, length or height, and head circumference be checked at age one week, four, six, 12 and 18 months of age, then at least annually to age five years. Body mass index should be plotted annually for children from two years. Recommended checks for infants and children up to 15 years generally include respiratory, ear and eye examinations, listening to the heart, oral hygiene and skin checks, with inquiries about hearing and vision concerns and other items of care.33
Developmental milestones are used to check a child’s development, or ability to perform increasingly complex fine- and gross-motor activities, speech and language, and social interactions as they mature. Early detection of developmental problems is important for accessing interventions and maximising their positive effects. The use of standardised developmental screening tools is recommended. The Ages and Stages Questionnaire (ASQ-3) and Bayley-III tools are widely used in Australia, and a culturally adapted ASQ-Talking about Raising Aboriginal Kids (ASQ-TRAK) has been developed for monitoring the development of Australian Aboriginal children.34 Other resources are available.35
Key growth and health measures
Analyses of 10,405 audit records of children collected from 132 PHC centres between 2007 and 2013 showed that many records did not include a recent record of the child’s weight, or a recent record of haemoglobin monitoring. There was wide variation between PHC centres in the proportion of children with recent records. This also applied for the monitoring and recording of developmental milestones, including for vision and hearing (see below). There was wide variation between PHC centres in the recording of follow-up actions, such as a follow-up weight check, nutrition advice or action plans for children assessed with growth faltering.36
Developmental care and participation in CQI
Another study analysed the developmental care records of children aged from three months to five years (2,466 client records, 109 PHC centres, from 2012 to 2014), to find the following:
- All participating PHC centres (100 per cent) included the five age-specific developmental care items in their clinic’s protocols (assessment of parent–child interaction, developmental milestones, vision and hearing, and advice or brief intervention about the physical and mental stimulation of the child). However, only 48 per cent of children had received the composite measure (five items) of basic developmental care in the previous 12 months: assessment of parent–child interaction, assessment of developmental milestones, assessment of vision, assessment of hearing, and advice about physical and mental stimulation of the child.
- Only 4 per cent of children younger than five years were documented as having developmental problems (for example, deficits in motor, communication, play, speech and language skills, hearing, vision, learning or cognition). This percentage is far lower than global averages, indicating a need to improve practitioner skills in developmental assessment.
- Among the children who had developmental problems identified, most (93 per cent) received clinic follow-up or relevant referral or both.37
- Sustained participation in CQI improved access and documentation of developmental care (Figure 12.2). There was an important dose–response of improved delivery of developmental care with improved participation in CQI. Further, CQI was effective for improving developmental care in a range of PHC settings, including government-managed and community controlled PHC services, remote and non-remote locations, and small and large populations.38
- There was a need for improved resourcing of developmental care and CQI in PHC centres.39
- Context-specific developmental screening tools and more uniform recording methods were also needed.40
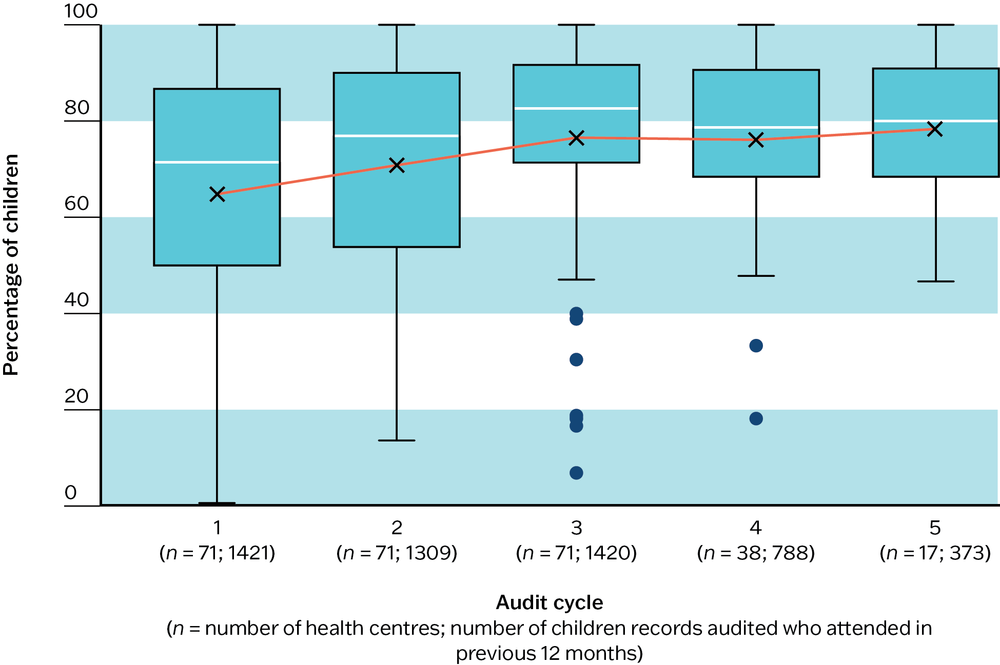
Figure 12.2 Mean percentage of children younger than four years of age attending within the previous 12 months who had a developmental milestones check, by audit cycle for health centres that have at least three years of audit data. Source: R. Bailie, Matthews et al. 2014.
Improved participation in CQI improved the delivery of developmental care.
Across CQI studies, there was a need to strengthen systems in these areas:
- recording of weight, haemoglobin and developmental milestones
- recording and follow-up action for children with growth faltering, anaemia, chronic ear infections and developmental delay
- recording and follow-up action for risks related to the domestic environment, financial situation, housing and food security
- continued participation in CQI, targeted staff training for child health and a systematic approach to delivering developmental care services for children.41
Immunisation
Immunisation schedules for vaccine preventable diseases (for example, diphtheria, polio, tetanus, hepatitis B, measles, mumps and rubella) vary in specific detail between countries and between jurisdictions in Australia. Child immunisation schedules are regularly and frequently updated. The table below reflects general Australian recommendations at the time of the CQI studies cited in this section.
|
|
Vaccine |
|---|---|
|
Birth |
hepatitis B |
|
2 months |
HepB-DTPa_Hib_IPV (hepatitis B, diphtheria, tetanus, acellular pertussis (whooping cough), haemophilus influenza type B, polio) pneumococcal vaccine (13vPCV) rotavirus |
|
4 months |
HepB-DTPa_Hib_IPV pneumococcal vaccine (13vPCV) rotavirus |
|
6 months |
HepB-DTPa_Hib_IPV influenza (annually): for those with certain medical risk factors 6 months and older, and Aboriginal and Torres Strait Islander children aged from 6 months to 5 years. pneumococcal vaccine (13vPCV): Aboriginal and Torres Strait Islander children and medically at-risk children rotavirus (3rd dose depends on brand of vaccine) |
|
12 months |
hepatitis A – 1st dose: Aboriginal and Torres Strait Islander children in high-risk areas measles, mumps and rubella (MMR) meningococcal ACWY pneumococcal vaccine (13vPCV) |
|
18 months |
DTPa haemophilus influenza type B (Hib) hepatitis A – 2nd dose: Aboriginal and Torres Strait Islander children measles, mumps, rubella, chickenpox (MMRV) |
|
4 years |
DTPa-IPV (diphtheria, tetanus, acellular pertussis (whooping cough) and polio) pneumococcal vaccine (23vPPV): medically at-risk children |
|
10–15 years |
DTPa human papilloma virus (HPV): usually 2 doses influenza – every year: Aboriginal and Torres Strait Islander peoples 15 years and older |
Table 12.1 Australian vaccination recommendations.
Analysis of trend audit data (10,405 child health records, 132 PHC services, between 2007 and 2013) found that there was room for improvement in immunisation coverage in all age groups across Australian jurisdictions, and progressively lower coverage for children in older age groups. This was particularly marked for immunisations scheduled for children older than 10 years. There was some improvement in the systematic recording of immunisations and in the delivery of immunisations scheduled for delivery at two years and older, but no evidence of improvement in recording of delivery of immunisations scheduled for delivery at birth (Figure 12.3).
There is an ongoing need to strengthen attention to:
- delivery and recording of immunisations scheduled for delivery at birth42
- delivery and recording of immunisations scheduled at birth and at two years and older43
- integrating systems for the timely delivery, recording and communication between PHC centres and other providers of child health services44
- immunisation charts and recordings in the clinical records of children in some PHC services.45
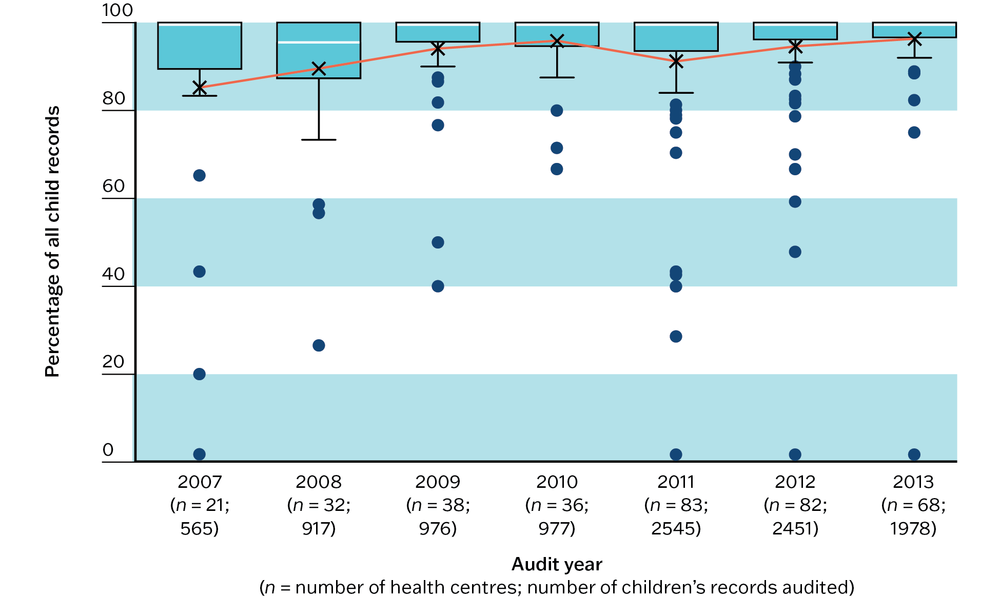
Figure 12.3a Mean percentage (by audit year for all health centres) of children with an immunisation chart present. Source: R. Bailie, Matthews et al. 2014.
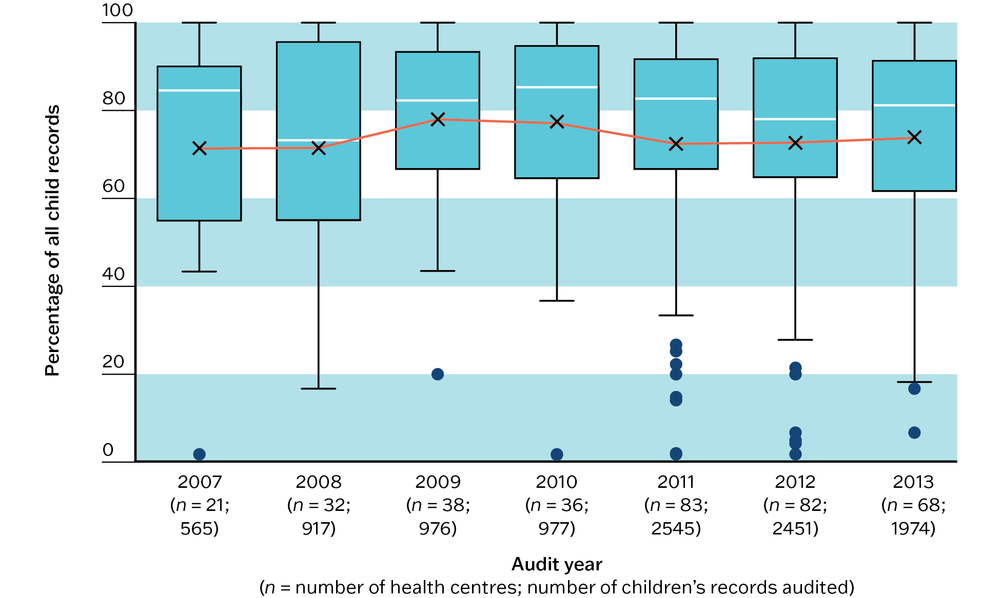
Figure 12.3b Mean percentage (by audit year for all health centres) of children with recorded hepatitis B immunisation at birth. Source: R. Bailie, Matthews et al. 2014.
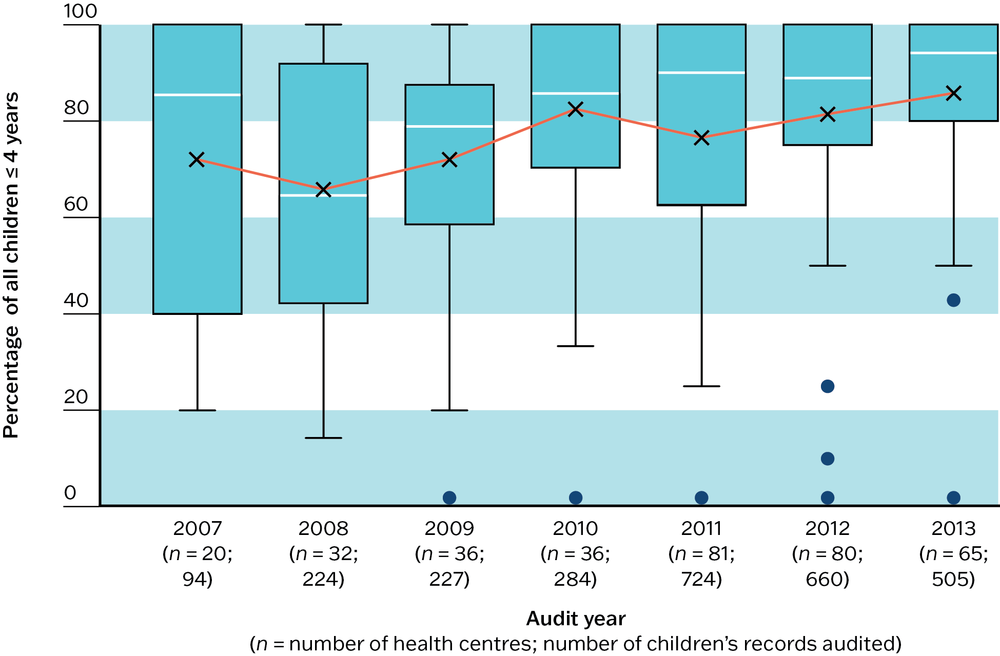
Figure 12.3c Mean percentage (by audit year for all health centres) of children with measles, mumps, rubella immunisation at four years of age. Source: R. Bailie, Matthews et al. 2014.
Example: improving timeliness of child immunisations through CQI
An Australian PHC service, covering a large geographical area, identified problems with the timeliness of immunisation for children and with client pathways. From the infant’s first visit to the child-and-family health nurse to the Aboriginal and Torres Strait Islander child health check, children and their caregivers were required to make multiple visits. This resulted in low compliance. The main clinic is in a regional town and an outreach clinic provides health care to several smaller communities. The outreach clinic has a maternity, midwife and antenatal program and a Healthy Start (newborns to 5-year-olds) program that includes immunisation, regular health checks and a children’s dental team.
As part of a continuous quality improvement process, the following strategies were implemented:
- The child-and-family nurse and doctor explored clinical processes and client pathways with the service’s health system support team.
- Data on completed child health checks and immunisation data were examined to establish a baseline for monitoring, and to guide discussions.
- The team reviewed client lists every morning for children who were overdue for their child health checks and immunisations. They restructured the clinic schedule to enable clients to go straight from the nurse to the doctor, ensuring that the child-and-family nurse and doctor were rostered on the same day.
- The service set up regular feedback and monitoring of results to the child health team to track improvement.
The continuous quality improvement process resulted in better team understanding of the timeliness indicator and its importance, and in monthly monitoring of timeliness data for children who have seen both a child and family health nurse and doctor in the one visit. Other outcomes of the process were increased staff interest in performance indicators and collecting and using data for CQI.46
Childhood anaemia
A low haemoglobin reading is often a sign of iron deficiency anaemia. Anaemia is defined as a haemoglobin level less than 110 g/dl for children aged 6–59 months.47
In Australia, the national guide to preventive health assessments for Aboriginal and Torres Strait Islander children recommends a haemoglobin check at age 6–9 months with a repeat at 18 months, or every six months until the age of five years in conjunction with treatment if anaemia persists.48 In geographical areas where there is a high prevalence of anaemia and parasitic infection, government policies and health service guidelines may recommend haemoglobin as a standard check, with six-monthly testing as routine to five years of age, then at 10 and 15 years. Follow-up care for abnormal findings is likely to involve nutrition advice, iron treatment, and repeat haemoglobin measurements within two months.
A study of audit records from 2007 to 2013 (10,405 children’s records, 132 PHC centres) showed no clear evidence of change in the patterns of routine checking for anaemia, or in recording of anaemia, across year or audit cycles.
- A significant number of records did not include a recent record of haemoglobin monitoring and there was wide variation between PHC centres in the proportion of children with a recent record – lower than expected given what we know about the population incidence of anaemia (Figure 12.4).
- There was wide variation between PHC centres in the recording of follow-up action, and generally low levels of recording of systematic actions being taken for these children – including deworming, prescription of iron supplements, nutritional advice, and follow-up monitoring of haemoglobin (Figure 12.5).49
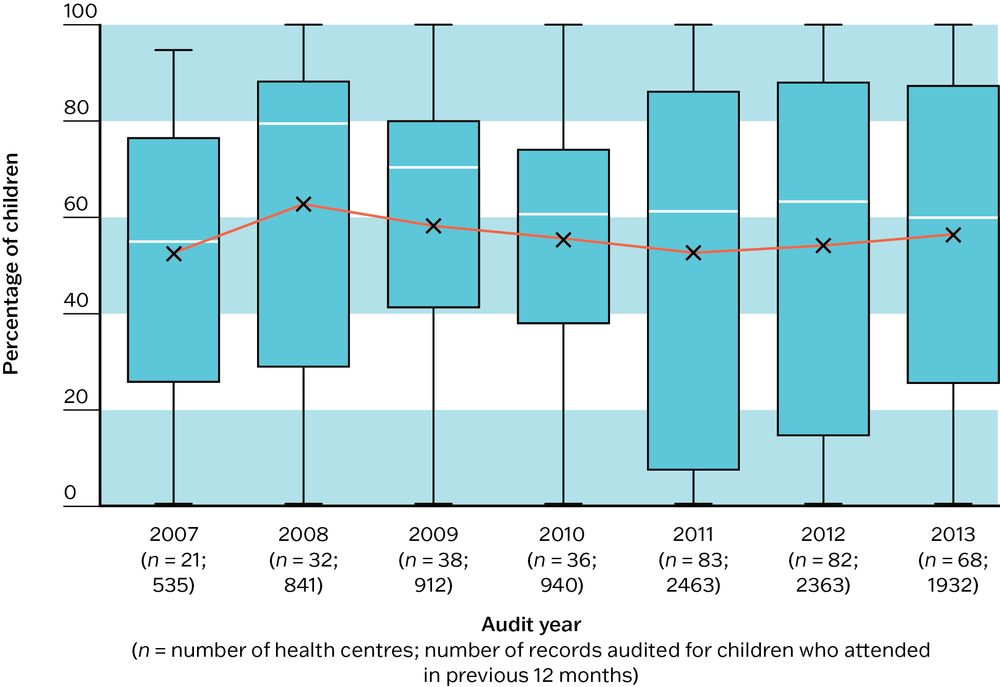
Figure 12.4 Mean percentage of children attending within the previous 12 months who had a haemoglobin check, by audit year. Source: R. Bailie, Matthews et al. 2014.
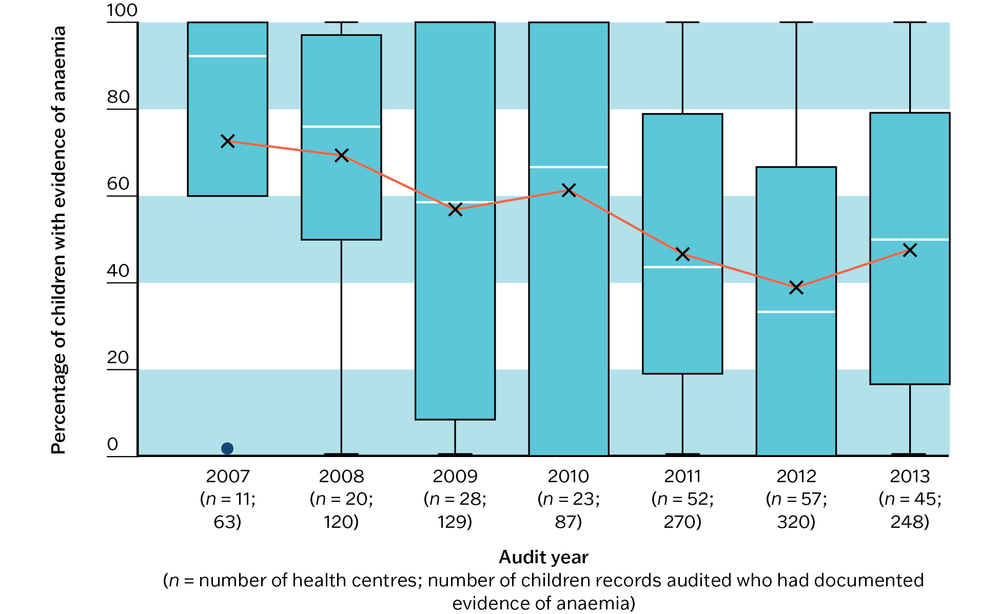
Figure 12.5a Mean percentage, by audit year, of children with anaemia who had documented evidence of deworming treatment. Source: R. Bailie, Matthews et al. 2014.
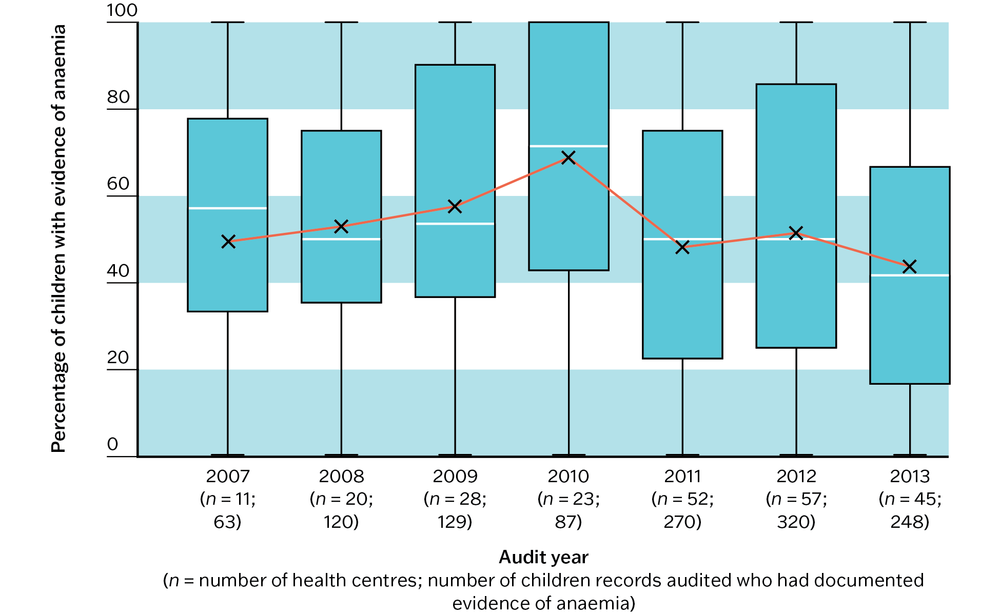
Figure 12.5b Mean percentage, by audit year, of children with anaemia who had documented evidence of a follow-up haemoglobin check. Source: R. Bailie, Matthews et al. 2014.
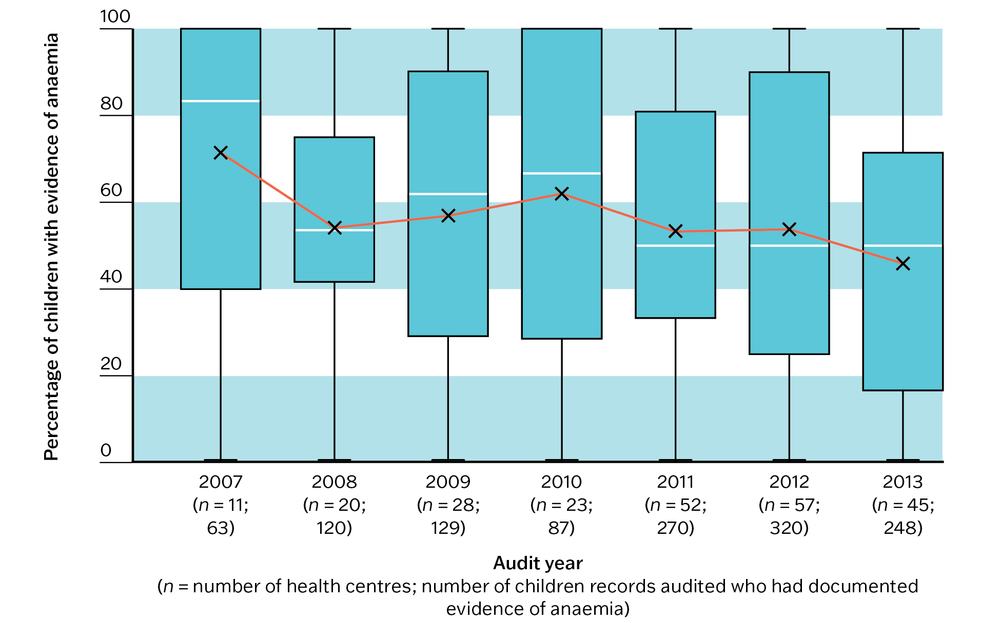
Figure 12.5c Mean percentage, by audit year, of children with anaemia who had documented evidence of an iron prescription. Source: R. Bailie, Matthews et al. 2014.
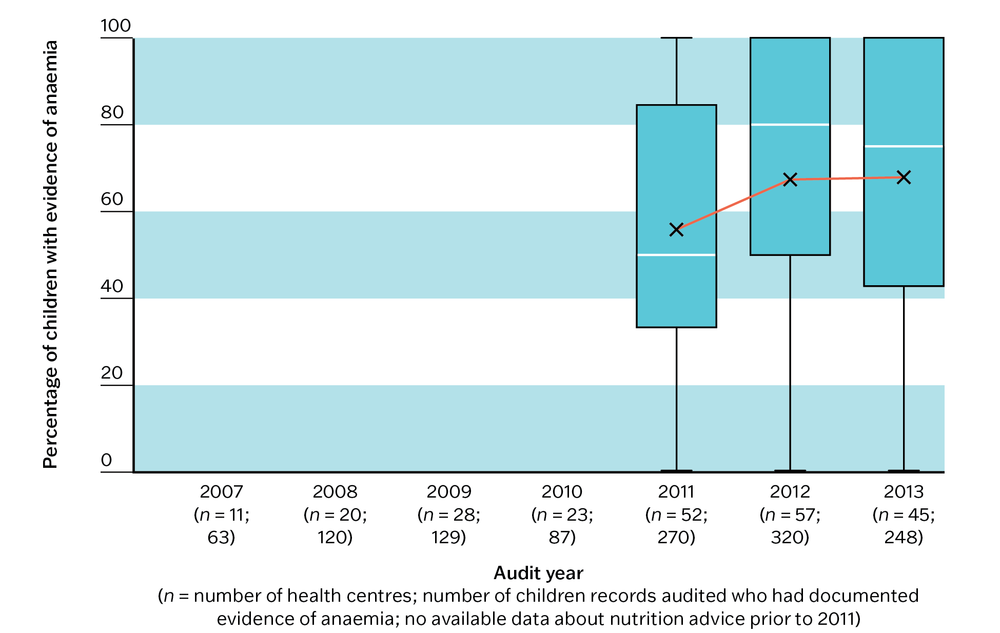
Figure 12.5d Mean percentage, by audit year, of children with anaemia who had documented evidence of nutrition advice. Source: R. Bailie, Matthews et al. 2014.
A separate 2012–14 study (2,287 children’s records, 109 PHC centres) had the following findings:
- both nutrition advice to carers about healthy foods and a haemoglobin measurement in the past 12 months had been completed for only 54 per cent of children
- children living in remote areas were more likely to receive both items of care than those attending PHC centres in rural and urban areas
- although abnormal haemoglobin measurements were higher in children aged 6 to 11 months, they were 71 per cent less likely to receive a haemoglobin check than children aged 1 to 5 years, and 52 per cent less likely to receive both items of care
- treatment and follow-up of children diagnosed with abnormal haemoglobin levels was low across age groups.50
There is a need to improve monitoring and recording of haemoglobin according to best-practice guidelines, including clear processes and/or access to guidelines, and systematic approaches to screening, nutrition advice, case finding and follow-up.
Anaemia health literacy
Anaemia health literacy of community members, and health practitioner’s knowledge of anaemia best-practice guidelines, was studied in a remote Indigenous community where English is not the first language. The research resulted in these findings:
- knowledge about anaemia in the community was good, but there was no evidence that this knowledge translated into improving the dietary intake of children, possibly due to food insecurity and poor knowledge about how iron-rich foods should be consumed
- community health practitioners’ knowledge of follow-up procedures for anaemia ranged from fair to excellent.51
These findings highlight the need for holistic approaches that address the social determinants of health, such as food security and health literacy, in addition to clinical care.
Social and emotional wellbeing
PHC services have the potential to improve social and emotional wellbeing and long-term neuro-developmental outcomes in vulnerable children.52 In Australia, there are specific guidelines for providing social and emotional wellbeing services in PHC centres. The guidelines include an assessment of the social determinants that may be affecting a child’s wellbeing.
A study of the social and emotional wellbeing services delivered to families of young Indigenous children attending services (2,466 client records, 109 PHC services) found that these services were not well delivered, with little difference in services provided in remote, rural and urban areas.
- All PHC services in the study included the age-specific national best-practice guidelines for social and emotional wellbeing care in their clinic protocols.
- Delivery of service items ranged from around 11 per cent (food security) to 75 per cent (assessment of parent–child interaction).
- Families of children younger than one year old were more likely to receive these services (for example, advice about social support, child stimulation) than families of older children, but many families were not receiving these items of care.
- Almost 25 per cent of families had no follow-up or referral for concerns about domestic environment, family support and financial situation, housing or food security.
- There is a need for better resourcing, supervision and training in the skills needed to provide these services, and better documentation of the services provided.53
Child protection
Protecting children from abuse, neglect and mistreatment is a major concern across the globe, with most Western countries confronting increasing numbers of children in need of support from child welfare services. In Australia, 174,700 children (1 in 32 children from birth to 17 years old) received child protection services in 2019–20.54 Aboriginal and Torres Strait Islander children are over-represented in the protection and out-of-home care system.55 Many issues affect the success of interventions: for example, cultural bias, inadequate prevention programs, cost and overburdened staff. Integration of services between different providers and continuity of engagement of parents over time can be challenging, particularly in remote areas.56
A review of the use of CQI in child protection systems found that strengths-based, solution-focused models of practice that were inclusive of the families engaged with child protection services consistently resulted in improved outcomes for children. Within agencies, the use of CQI had these results:
- the gathering of appropriate evidence for outcome measurement
- improvements in processes for working with children and families
- more consistent application of practice frameworks
- more positive and engaged staff.57
Key messages for improving the delivery of child health care
Although there are likely to be some important differences between specific settings, patterns of PHC delivery for Aboriginal and Torres Strait Islander children may reflect care delivery in many international settings. This CQI research identifies clear priorities and strategies for improving health care for children.
There are common evidence-to-practice gaps in child health care that call for system-wide and local attention:
- recording of all immunisations in children’s health records, and the delivery of immunisations scheduled for delivery at birth and at two years and older
- monitoring and recording of key measures, including weight, haemoglobin and developmental milestones, and follow-up action for faltering growth, anaemia, chronic ear infections, developmental delay, and risks related to domestic environment, financial situation, housing and food security
- recording of advice or brief interventions on child nutrition, passive smoking, infection prevention and hygiene, injury prevention, domestic or social and environmental conditions, and child development
- providing follow-up or referral to other agencies for concerns about domestic environment, family support and financial situation, housing and food security
- recording of inquiries made regarding the parents’ or carers’ use of alcohol, tobacco and other drugs, and discussion or advice or both provided on risks to the health of children
- developing systems for effective engagement between health centres and communities
- implementing systems that support regional health planning.
Focus on reducing barriers and strengthening enablers for providing best-practice child health care, through actions such as these:
- recruitment of PHC teams with the right mix of skills to provide child health services (for example, a child health nurse)
- staff training and development (for example, in areas of child health relevant to the evidence-practice gaps, in cultural safety)
- development of clinical information systems (for example, improve and make better use of clinical information systems including the sharing of electronic records across providers to assist follow-up, completeness of children’s records and efficient use of resources for providing care)
- promotion of parenting practices that protect children’s health and wellbeing (for example, encourage families to bring children to PHC services for child health checks and other scheduled services, and to seek support)
- community engagement, support and health literacy (for example, work with communities to build understanding of child health issues and priorities; involve community-based workers, community members and agencies in providing practical support for families and reducing risks to child health).
Aim for less siloed service delivery and better inter-agency coordination. Developing systems and opportunities for staff across agencies to share relevant knowledge about children and their families and carers will help to provide holistic, best-practice care.
Sustained participation in CQI activities can improve basic developmental care in PHC settings, and the overall delivery of child health care.
Sustained participation in CQI activities can improve basic developmental care in PHC settings, and the overall delivery of child health care.
Improving PHC for Aboriginal and Torres Strait Islander children
Improving the delivery of PHC for Aboriginal and Torres Strait Islander children is crucial for better health and wellbeing across the life span and for improving health equity for Aboriginal and Torres Strait Islander Australians.
Our research into the quality of care for Aboriginal and Torres Strait Islander children since 2007 highlights where significant improvements continue to be needed. Many aspects of child health care are being done well in many health centres, but common gaps and persistent wide variation in care delivery amongst health centres indicate broader system failures. Systems for delivering child health services need to be improved at local and at higher levels of the health system, including systems for coordinating service delivery across sectors (for example, child care, education, housing) and for ensuring the use of culturally appropriate resources.58 The onset of chronic conditions at earlier ages and the prevalence of diseases that are almost eradicated in most wealthy countries, but persist for Aboriginal and Torres Strait Islander children (for example, acute rheumatic fever) are evidence of the urgency of these improvements for enabling Aboriginal and Torres Strait Islander children to thrive and fulfil their potential.
Our studies found that children younger than two years were more likely to have a recorded assessment for social and emotional wellbeing, anaemia and development than children aged from two to five years, despite older children having a greater risk of developmental problems.59 While good care processes and organisational systems are important for improving delivery, it is imperative that parents and carers feel comfortable bringing children to PHC services. Cultural safety is essential so that PHC services can integrate high-quality clinical care with the promotion of protective factors that build children’s resilience and underpin wellbeing, such as connection to Country, family, community, culture and ancestry. This has implications for the proportion of Indigenous staff employed in PHC services, staff training and mentorship (particularly in cultural safety), links with other service providers and processes for engaging communities in the design, delivery and continuous improvement of PHC services for Aboriginal and Torres Strait Islander children.
Aboriginal and Torres Strait Islander PHC services are in a strong position to lead systems-level integration of services to tackle the determinants of children’s health and wellbeing by engaging community leaders and members in improving care; linking physical health and social and emotional wellbeing programs within PHC; linking with intersectoral service partners; and advocating at policy levels.60
Aboriginal and Torres Strait Islander PHC services are in a strong position to lead systems-level integration of services to tackle the determinants of children’s health and wellbeing.
Reporting on other indicators of quality primary health care for children
In this chapter, we have reported selected findings on the quality of child health care. The indicators were selected because they are important items of best-practice PHC for children and have been identified as priorities for improvement through our CQI research. In identifying these priorities, we drew on empirical data and the knowledge of PHC practitioners. Findings relating to other indicators are available. Table 12.2 lists all the child health indicators included in the ABCD child health audit tool, and the research papers that report results on each indicator.
|
Child health |
Research (full citations provided in reference list) |
|---|---|
|
Record systems | |
|
Immunisation record in child’s health file Child recorded in electronic recall system |
R. Bailie, Matthews et al. 2014; McAullay, McAuley et al. 2018 |
|
Record of child health check |
D’Aprano, Silburn et al. 2016; McAullay, McAuley et al. 2018 |
|
Scheduled immunisations |
R. Bailie, Matthews et al. 2014; R.S. Bailie, Si et al. 2009 |
|
Measurements | |
|
Weight |
R. Bailie, Matthews et al. 2014; R. Bailie, Si et al. 2008; McAullay, McAuley et al. 2018 |
|
Length or height |
R. Bailie, Si et al. 2008 |
|
Head circumference |
R. Bailie, Si et al. 2008 |
|
Body mass index* |
|
|
Growth chart |
R. Bailie, Si et al. 2008 |
|
Haemoglobin |
R. Bailie, Matthews et al. 2014; R. Bailie, Si et al. 2008; McAullay, McAuley et al. 2018; Strobel, McAuley et al. 2018 |
|
Urinalysis for proteinuria* |
|
|
Appearance | |
|
Hip examination |
R. Bailie, Si et al. 2008 |
|
Gait* |
|
|
Skin check |
McAullay, McAuley et al. 2018 |
|
Oral hygiene |
McAullay, McAuley et al. 2018 |
|
Testes check |
R. Bailie, Si et al. 2008 |
|
Examinations | |
|
Cardiac auscultation |
R. Bailie, Si et al. 2008 |
|
Respiratory examination* |
|
|
Ear examination |
R. Bailie, Si et al. 2008; McAullay, McAuley et al. 2018 |
|
Eye examination and vision test |
R. Bailie, Si et al. 2008; Burnett, Morse et al. 2016; Edmond, Tung et al. 2018 |
|
Trachoma |
Burnett, Morse et al. 2016 |
|
Child development | |
|
Developmental milestones |
R. Bailie, Matthews et al. 2014; R. Bailie, Si et al. 2008; D’Aprano, Silburn et al. 2016; Edmond, Tung et al. 2018; McAullay, McAuley et al. 2018; Strobel, McAuley et al. 2018 |
|
Concerns about vision |
R. Bailie, Si et al. 2008; Burnett, Morse et al. 2016; Edmond, Tung et al. 2018 |
|
Hearing |
R. Bailie, Si et al. 2008; Edmond, Tung et al. 2018; McAullay, McAuley et al. 2018; Strobel, McAuley et al. 2018 |
|
Parent–child interaction |
D’Aprano, Silburn et al. 2016; Edmond, McAuley et al. 2018; Edmond, Tung et al. 2018; McAullay, McAuley et al. 2018; Strobel, McAuley et al. 2018 |
|
Inquiry or brief intervention | |
|
Breastfeeding |
R. Bailie, Si et al. 2008; Gibson-Helm, J. Bailie et al. 2016; Gibson-Helm, J. Bailie et al. 2018; McAullay, McAuley et al. 2018 |
|
Nutrition |
R. Bailie, Matthews et al. 2014; R. Bailie, Si et al. 2008; McAullay, McAuley et al. 2018; Strobel, McAuley et al. 2018; |
|
SIDS (sudden infant death syndrome) or SUDI (sudden unexpected death in infancy) prevention |
R. Bailie, Si et al. 2008; Gibson-Helm, J. Bailie et al. 2016, 2018 |
|
Passive smoking risk |
R. Bailie, Matthews et al. 2014; R. Bailie, Si et al. 2008; Gibson-Helm, J. Bailie et al. 2016, 2018 |
|
Infection prevention and hygiene |
R. Bailie, Matthews et al. 2014; R. Bailie, Si et al. 2008 |
|
Oral health |
R. Bailie, Si et al. 2008; McAullay, McAuley et al. 2018 |
|
Injury prevention |
R. Bailie, Si et al. 2008 |
|
Domestic or social environment |
R. Bailie, Matthews et al. 2014; R. Bailie, Si et al. 2008; Edmond, McAuley et al. 2018; Strobel, McAuley et al. 2018 |
|
Social or family support |
R. Bailie, Si et al. 2008; Edmond, McAuley et al. 2018; Strobel, McAuley et al. 2018 |
|
Financial situation |
R. Bailie, Si et al. 2008; Edmond, McAuley et al. 2018 |
|
Housing condition |
R. Bailie, Si et al. 2008; Edmond, McAuley et al. 2018; Strobel, McAuley et al. 2018 |
|
Food security |
R. Bailie, Si et al. 2008; Edmond, McAuley et al. 2018 |
|
Physical and mental stimulation |
R. Bailie, Si et al. 2008; Edmond, McAuley et al. 2018; Edmond, Tung et al. 2018; Strobel, McAuley et al. 2018 |
|
Physical activity and rest |
Edmond, Tung et al. 2018 |
|
Education progress* |
|
|
Social and emotional wellbeing |
Edmond, McAuley et al. 2018; Strobel, McAuley et al. 2018 |
|
Sexual and reproductive health and safe sex advice* |
|
|
Risk factors: Smoking, alcohol use, drug or substance use |
R. Bailie, Matthews et al. 2014 |
|
Follow-up of abnormal clinical findings | |
|
Growth faltering or failure to thrive |
R. Bailie, Matthews et al. 2014; R. Bailie, Si et al. 2008; McAullay, McAuley et al. 2018 |
|
Evidence of overweight or obesity* |
|
|
Recurrent or chronic ear infections |
R. Bailie, Si et al. 2008; McAullay, McAuley et al. 2018 |
|
Evidence of anaemia |
R. Bailie, Si et al. 2008; McAullay, McAuley et al. 2018 |
|
Recurrent or chronic respiratory disease, number of respiratory infections |
R. Bailie, Si et al. 2008 |
|
Infected skin sores |
McAullay, McAuley et al. 2018 |
|
Scabies* |
|
|
Proteinuria* |
|
|
Developmental delay |
R. Bailie, Matthews et al. 2014; R. Bailie, Si et al. 2008; D’Aprano, Silburn et al. 2016; Edmond, Tung et al. 2018 |
|
Concern and follow-up: | |
|
Domestic environment |
R. Bailie, Si et al. 2008; Edmond, McAuley et al. 2018 |
|
Social or family support and financial situation |
R. Bailie, Si et al. 2008; Edmond, McAuley et al. 2018 |
|
Housing condition and food security |
R. Bailie, Si et al. 2008; Edmond, McAuley et al. 2018 |
|
* Results for these indicators have not been reported in publications to date. | |
Table 12.2 Child health indicators in the child health audit tool, and publications that report results for each.
References
Aquino, D., D. Leonard, N. Hadgraft and J. Marley (2018). High prevalence of early onset anaemia amongst Aboriginal and Torres Strait Islander infants in remote northern Australia. Australian Journal of Rural Health 26(4): 245–50. DOI: 10.1111/ajr.12403.
Australian Bureau of Statistics (2019). National Aboriginal and Torres Strait Islander health survey, 2018–19. ABS cat. no. 4715.0. Canberra: ABS.
Australian Bureau of Statistics (2017). National Aboriginal and Torres Strait Islander social survey, 2014–15. ABS cat. no. 4714.0. Canberra: ABS.
Australian Institute of Family Studies (2018). The growing over-representation of Aboriginal and Torres Strait Islander children in care. AIFS. https://aifs.gov.au/cfca/2018/05/07/growing-over-representation-aboriginal-and-torres-strait-islander-children-care.
Australian Institute of Health and Welfare (2023). Aboriginal and Torres Strait Islander Health Performance Framework summary report 2023. Canberra: AIHW.
Australian Institute of Health and Welfare (2021). Child protection Australia 2019–20. Canberra: Australian Government. https://www.aihw.gov.au/reports/child-protection/child-protection-australia-2019-20/summary.
Bailie R., V. Matthews, J. Bailie and A. Laycock (2014). Primary health care for Aboriginal and Torres Strait Islander children: priority evidence–practice gaps and stakeholder views on barriers and strategies for improvement. Final report. Brisbane: Menzies School of Health Research.
Bailie R., D. Si, M. Dowden, C. Connors, L. O’Donoghue, H. Liddle et al. (2008). Delivery of child health services in Indigenous communities: implications for the federal government’s emergency intervention in the Northern Territory. Medical Journal of Australia 188(10): 615–18. DOI: 10.5694/j.1326-5377.2008.tb01806.x
Bailie R., D. Si, M. Dowden, C. Selvey, C. Kennedy, R. Cox et al. (2009). A systems approach to improving timeliness of immunisation. Vaccine 27: 3669–74. DOI: 10.1016/j.vaccine.2009.02.068.
Barker, D., J. Eriksson, T. Forsén and C. Osmond (2002). Fetal origins of adult disease: strength of effects and biological basis. International Journal of Epidemiology 31(6): 1235–39. DOI: 10.1093/ije/31.6.1235.
Blair, M., and D. Hall (2006). From health surveillance to health promotion: the changing focus in preventive children’s services. Archives of Disease in Childhood 91(9): 730–5. DOI: 10.1136/adc.2004.065003.
Burnett, A., A. Morse, T. Naduvilath, A. Boudville, H. Taylor and R. Bailie (2016). Delivery of eye and vision services in Aboriginal and Torres Strait Islander primary health care centers. Frontiers in Public Health 4: 276. DOI: 10.3389/fpubh.2016.00276.
Chando, S., J. Craig, L. Burgess, S. Sherriff, A. Purcell, H. Gunasekera et al. (2020). Developmental risk among Aboriginal children living in urban areas in Australia: the study of environment on Aboriginal resilience and child health (SEARCH). BMC Pediatrics 20(1): 13. DOI: 10.1186/s12887-019-1902-z.
Closing the Gap (n.d.). https://www.closingthegap.gov.au/.
D’Aprano, A., S. Silburn, V. Johnston, R. Bailie, F. Mensah, F. Oberklaid et al. (2016). Challenges in monitoring the development of young children in remote Aboriginal health services: clinical audit findings and recommendations for improving practice. Rural and Remote Health 16(3852): 1–10. DOI: 10.22605/RRH3852.
Department of Health (2019). National immunisation strategy for Australia 2019 to 2024. Canberra: Australian Government.
Department of Health and Aged Care (2022). Annual health checks for Aboriginal and Torres Strait Islander people. https://www.health.gov.au/health-topics/aboriginal-and-torres-strait-islander-health/primary-care/annual-health-checks.
Edmond, K., K. McAuley, D. McAullay, V. Matthews, N. Strobel, R. Marriott et al. (2018). Quality of social and emotional wellbeing services for families of young Indigenous children attending primary care centers: a cross sectional analysis. BMC Health Services Research 18(1). DOI: 10.1186/s12913-018-2883-6.
Edmond, K., S. Tung, K. McAuley, N. Strobel and D. McAullay (2018). Improving developmental care in primary practice for disadvantaged children. Archives of Disease in Childhood 104: 372–80. DOI: 10.1136/archdischild-2018-315164.
Engle, P., L. Fernald, H. Alderman, J. Behrman, C. O’Gara, A. Yousafzai et al. (2011). Strategies for reducing inequalities and improving developmental outcomes for young children in low-income and middle-income countries. Lancet 378(9799): 1339–53. DOI: 10.1016/S0140-6736(11)60889-1.
Fremantle, E., Y. Zurynski, D. Mahajan, H. D’Antoine and E. Elliott (2008). Indigenous child health: urgent need for improved data to underpin better health outcomes. Medical Journal of Australia 188(10): 588–91. DOI: 10.5694/j.1326-5377.2008.tb01797.x.
Gibson-Helm, M., J. Bailie, V. Matthews, A. Laycock, J. Boyle and R. Bailie (2018). Identifying evidence–practice gaps and strategies for improvement in Aboriginal and Torres Strait Islander maternal health care. PLOS One 13(2): e0192262. DOI: 10.1371/journal.pone.0192262.
Gibson-Helm, M., J. Bailie, V. Matthews, A. Laycock, J. Boyle and R. Bailie (2016). Priority evidence-practice gaps in Aboriginal and Torres Strait Islander maternal health care final report: engaging stakeholders in identifying priority evidence–practice gaps and strategies for improvement in primary health care (ESP project). Brisbane: Menzies School of Health Research.
Grantham-McGregor, S. and C. Ani (2001). A review of studies on the effect of iron deficiency on cognitive development in children. Journal of Nutrition 131(2S–2): 649S–68S. DOI: 10.1093/jn/131.2.649S.
Grantham-McGregor, S., Y. Cheung, S. Cueto, P. Glewwe, L. Richter and B. Strupp (2007). Developmental potential in the first 5 years for children in developing countries. Lancet (British edition) 369(9555): 60–70. DOI: 10.1016/S0140-6736(07)60032-4.
Hertzman, C. and C. Power (2004). Child development as a determinant of health across the life course. Current Paediatrics 14(5): 438–43. DOI: 10.1016/j.cupe.2004.05.008.
Kearns, T., F. Ward, S. Puszka, R. Gundjirryirr, B. Moss and R. Bailie (2017). Anaemia health literacy of community members and health practitioners knowledge of best practice guidelines in a remote Australian Aboriginal community. Universal Journal of Public Health 5(1): 32–9. DOI: 10.13189/ujph.2017.050105.
McAullay, D., K. McAuley, R. Bailie, V. Mathews, P. Jacoby, K. Gardner et al. (2018). Sustained participation in annual continuous quality improvement activities improves quality of care for Aboriginal and Torres Strait Islander children. Journal of Paediatrics and Child Health 54(2): 132–40. DOI: 10.1111/jpc.13673.
McCalman, J., R. Bailie, R. Bainbridge, K. McPhail-Bell, N. Percival, D. Askew et al. (2018). Continuous quality improvement and comprehensive primary health care: a systems framework to improve service quality and health outcomes. Frontiers in Public Health 6: 76. DOI: 10.3389/fpubh.2018.00076.
McDonald, E., R. Bailie, A. Rumbold, P. Morris and B. Paterson (2008). Preventing growth faltering among Australian Indigenous children: implications for policy and practice. Medical Journal of Australia 188(8 Suppl): S84–6. DOI: 10.5694/j.1326-5377.2008.tb01753.x.
Menzies School of Health Research and One21seventy (2015). Child health clinical audit tool. Brisbane: Menzies School of Health Research.
Mitchinson, C., N. Strobel, D. McAullay, K. McAuley, R. Bailie and K. Edmond (2019). Anemia in disadvantaged children aged under five years; quality of care in primary practice. BMC Pediatrics 19(1): 178. DOI: 10.1186/s12887-019-1543-2.
National Aboriginal Community Controlled Health Organisation and Royal Australian College of General Practitioners (2024). National guide to a preventative health assessment for Aboriginal and Torres Strait Islander people, 4th edn. Melbourne: RACGP.
Newham, J. and F. Cunningham (2015). Continuous quality improvement success stories: identifying effective strategies for CQI in Aboriginal and Torres Strait Islander primary health care – study report. ABCD National Research Partnership. Brisbane: ABCD National Research Partnership, Menzies School of Health Research.
Priest, N., T. Mackean, E. Waters, E. Davis and E. Riggs (2009). Indigenous child health research: a critical analysis of Australian studies. Australian and New Zealand Journal of Public Health 33(1): 55–63. DOI: 10.1111/j.1753-6405.2009.00339.x.
Productivity Commission (2023). Closing the Gap: annual data compilation report July 2023. Canberra: Australian Government.
Productivity Commission (2020). Overcoming Indigenous disadvantage: key indicators 2020. Canberra: Australian Government. https://www.pc.gov.au/research/ongoing/overcoming-indigenous-disadvantage/2020.
Robinson, G., S. Mares and F. Arney (2017). Continuity, engagement and integration: early intervention in remote Australian Aboriginal communities. Australian Social Work 70(1): 116–24. DOI: 10.1080/0312407X.2016.1146315.
Sabanathan, S., B. Wills and M. Gladstone (2015). Child development assessment tools in low-income and middle-income countries: how can we use them more appropriately? Archives of Disease in Childhood 100(5): 482–8. DOI: 10.1136/archdischild-2014-308114.
Siddiqi, K. and J. Newell (2005). Putting evidence into practice in low-resource settings. Bulletin of the World Health Organization 83(12): 882.
Simpson, S., A. D’Aprano, C. Tayler, S. Toon Khoo and R. Highfold (2016). Validation of a culturally adapted developmental screening tool for Australian Aboriginal children: early findings and next steps. Early Human Development 103: 91–5. DOI: 10.1016/j.earlhumdev.2016.08.005.
Strobel, N., K. McAuley, V. Matthews, A. Richardson, J. Agostino, R. Bailie et al. (2018). Understanding the structure and processes of primary health care for young indigenous children. Journal of Primary Health Care 10(3): 267–78. DOI: 10.1071/HC18006.
Strong Kids, Strong Future (n.d.). ASQ-TRAK. https://www.strongkidsstrongfuture.com.au/asqtrak/.
Walker, S., T. Wachs, S. Grantham-McGregor, M. Black, C. Nelson, S. Huffman et al. (2011). Inequality in early childhood: risk and protective factors for early child development. Lancet 378(9799): 1325–38. DOI: 10.1016/S0140-6736(11)60555-2.
Williamson, A., C. D’Este, K. Clapham, S. Redman, T. Manton, S. Eades et al. (2016). What are the factors associated with good mental health among Aboriginal children in urban New South Wales, Australia? Phase I findings from the study of environment on Aboriginal resilience and child health (SEARCH). BMJ Open 6(7): e011182–e82. DOI: 10.1136/bmjopen-2016-011182.
World Health Organization (2020). Children: improving survival and well being. Fact sheets. https://www.who.int/en/news-room/fact-sheets/detail/children-reducing-mortality.
World Health Organization (2011). Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System, WHO/NMH/NHD/MNM/11.1. Geneva: World Health Organization.
Zuchowski, I., D. Miles, C. Woods and K. Tsey (2017). Continuous quality improvement processes in child protection: a systematic literature review. Research on Social Work Practice 19(4): 1–12. DOI: 10.1177/1049731517743337.
1 Barker, Eriksson et al. 2002.
2 Hertzman and Power 2004.
3 World Health Organization 2020.
4 Engle, Fernald et al. 2011; Grantham-McGregor, Cheung et al. 2007; Walker, Wachs et al. 2011.
5 Blair and Hall 2006; Sabanathan, Wills and Gladstone 2015.
6 Siddiqi and Newell 2005.
7 Productivity Commission 2020.
8 Australian Institute of Health and Welfare 2023.
9 Department of Health 2019.
10 Productivity Commission 2023.
11 Australian Institute of Health and Welfare 2023.
12 Productivity Commission 2023.
13 Australian Bureau of Statistics 2019.
14 Australian Bureau of Statistics 2017.
15 Priest, Mackean et al. 2009.
16 Aquino, Leonard et al. 2018.
17 Grantham-McGregor and Ani 2001.
18 McDonald, R. Bailie et al. 2008.
19 Australian Institute of Health and Welfare 2021.
20 Williamson, D’Este et al. 2016.
21 Chando, Craig et al. 2020.
22 See Closing the Gap n.d.
23 See Department of Health and Aged Care 2022.
24 Chando, Craig et al. 2020; McCalman, R. Bailie et al. 2018.
25 Menzies School of Health Research and One21seventy 2015.
26 McAullay, McAuley et al. 2018.
27 R. Bailie, Matthews et al. 2014.
28 R. Bailie, Matthews et al. 2014.
29 R. Bailie, Matthews et al. 2014.
30 R. Bailie, Matthews et al. 2014.
31 R. Bailie, Matthews et al. 2014.
32 National Aboriginal Community Controlled Health Organisation and Royal Australian College 2024.
33 National Aboriginal Community Controlled Health Organisation and Royal Australian College 2024.
34 Simpson, D’Aprano et al. 2016; Strong Kids, Strong Future n.d.
35 For example, Parents’ Evaluation of Developmental Status (PEDS) questionnaire.
36 R. Bailie, Matthews et al. 2014.
37 Edmond, Tung et al. 2018.
38 Edmond, Tung et al. 2018.
39 Edmond, Tung et al. 2018.
40 D’Aprano, Silburn et al. 2016.
41 R. Bailie, Matthews et al. 2014; D’Aprano, Silburn et al. 2016.
42 R. Bailie, Matthews et al. 2014.
43 R. Bailie, Matthews et al. 2014.
44 R. Bailie, Si et al. 2009.
45 R. Bailie, Matthews et al. 2014.
46 Newham and Cunningham 2015.
47 World Health Organization 2011.
48 National Aboriginal Community Controlled Health Organisation and Royal Australian College 2024.
49 R. Bailie, Matthews et al. 2014.
50 Mitchinson, Strobel et al. 2019.
51 Kearns, Ward et al. 2017.
52 Engle, Fernald et al. 2011; Fremantle, Zurynski et al. 2008.
53 Edmond, McAuley et al. 2018.
54 Australian Institute of Health and Welfare 2021.
55 Australian Institute of Family Studies 2018.
56 Robinson, Mares and Arney 2017.
57 Zuchowski, Miles et al. 2017.
58 R. Bailie, Matthews et al. 2014; D’Aprano, Silburn et al. 2016; Strobel, McAuley et al. 2018.
59 Edmond, Tung et al. 2018; Strobel, McAuley et al. 2018.
60 McCalman, R. Bailie et al. 2018.