13
Improving maternal health care
Maternal care in PHC
Primary healthcare (PHC) services have a vital role in providing integrated pre-conception, pregnancy and postnatal care, and in many places, care during childbirth. High-quality maternal care lays foundations for babies to have the best possible start in life and includes these key elements:
- identifying risks to health
- preventing and managing pregnancy-related complications, illnesses, or concurrent diseases
- supporting the transition to birthing and motherhood
- health education and health promotion.
There have been significant gains in maternal outcomes in recent decades. Between 2000 and 2017, the number of maternal deaths per 100,000 live births dropped by about 38 per cent worldwide. The infant mortality rate more than halved from an estimated 65 deaths per 1,000 live births in 1990, to 29 deaths per 1,000 live births in 2017. However, inequalities persist. Low-income countries reported 462 maternal deaths per 100,000 live births compared with 11 per 100,000 live births in high-income countries, and risk of infant mortality was highest in the World Health Organization African Region.1 These statistics reflect poor access to good-quality health services (for example, lack of skilled health workers or local birthing facilities) and other underlying determinants of health and health care. Poverty, lack of information, and poor integration of cultural practices into health services may also prevent women from seeking or receiving care from health professionals during pregnancy and childbirth.2 Parental capacity to provide nurturing care is linked to social determinants of health and to experiences of health inequity and poverty.3
Global improvement in maternal outcomes has shifted the focus from survival to maximising maternal health and wellbeing through best-practice women-centred care. Good antenatal care aims for a positive pregnancy experience and supports women to make informed choices about their care and childbirth. It includes effective communication, emotional support, respect and dignity, medical care, and relevant and timely information.4 Access to appropriate care and counselling for diseases (for example, tuberculosis, HIV, malaria), and chronic conditions such as diabetes, kidney disease and heart disease are important components of antenatal care.
Good antenatal care aims for a positive pregnancy experience and supports women to make informed choices about their care and childbirth.
Postnatal care (usually provided for 6–8 weeks after birth) should be a continuation of the care provided through pregnancy, labour and childbirth. It focuses on clinical care needs (for example, preventing and treating postpartum complications), rest and nutrition, baby feeding, parent–baby attachment, social and emotional support, contraception and, often, cervical screening. The complexity of providing holistic woman-centred care is one of the reasons that CQI has such positive potential in maternal health care.
Health of Aboriginal and Torres Strait Islander mothers and their babies
Aboriginal and Torres Strait Islander mothers account for around 5 per cent of women who give birth in Australia. In recent years, improvements in outcomes have included an increase in the percentage of Aboriginal and Torres Strait Islander mothers who seek early and regular antenatal care. In 2021, 72 per cent of Aboriginal and Torres Strait Islander mothers attended an antenatal visit in the first trimester compared with 50 per cent in 2012, and 88 per cent of those who sought antenatal care attended five or more pregnancy care visits. Over a similar period, the proportion of women who smoked during pregnancy and the proportion of babies with a low birth weight born to Aboriginal and Torres Strait Islander mothers decreased.5 These improvements have been achieved despite system barriers such as variability in culturally safe care, some expectations that women in rural areas transfer to bigger cities for birthing, and staff shortages (particularly in rural and remote areas). The proportion of babies with a healthy birth weight still needs to increase to reach the Closing the Gap target of 91 per cent by 2031,6 and the significant reduction in sudden unexpected death in infancy in Australia since the early 1990s has not been experienced among Aboriginal and Torres Strait Islander communities.7
Many Aboriginal and Torres Strait Islander women experience medical, behavioural, environmental, economic, and social and emotional wellbeing risk.8 For example the incidence of diabetes, including gestational diabetes, is higher among Aboriginal and Torres Strait Islander peoples, and people living in lower socio-economic areas and remote areas.9 Gestational diabetes is a strong predictor of future type 2 diabetes10 and children exposed to hyperglycaemia (high blood glucose) in utero are at risk of developing diabetes at an early age.11 Low birth weight also increases the risk of children developing chronic illnesses in later life.12 Risk factors for chronic illnesses are relatively common among young Indigenous women,13 and many of the risk factors (for example, infections, smoking, high-risk alcohol use, being obese or underweight) are associated with poor pregnancy outcomes.14 High levels of psychological distress and stressors during pregnancy may also be associated with low birth weight and preterm birth.15
The relatively high levels of risk are a legacy of government policies that ruptured family and cultural connections and removed many Aboriginal and Torres Strait Islander children from their families. The positive counter effects of extended kinship and community care for parents, spiritual connection to Country and active cultural practices are vitally important for protecting the health and wellbeing of many Aboriginal and Torres Strait Islander mothers and their families. These protective factors need to be supported through culturally safe PHC that builds on community and cultural strengths.
High-quality preventive and pre-conception care, and best-practice care during and after pregnancy and birthing, is crucial for closing the gap in maternal health outcomes between Aboriginal and Torres Strait Islander and non-Indigenous women in Australia.
Recommended maternal care
High-quality maternal care includes emotional support and advice, clinical care, and relevant and timely information.
The World Health Organization recommends that all pregnant women have a minimum of eight contacts with a health provider. Antenatal care should include nutrition interventions (for example, advice about healthy eating and exercise, iron supplements); maternal and foetal assessment (for early detection of pregnancy complications, and identification of women at risk of complications during birthing); interventions for smoking, alcohol and other drug use; disease testing and care (for example, for gestational diabetes); preventive health measures (for example, tetanus vaccination); and interventions for common physiological symptoms (for example, nausea). Women-held case notes, midwife-led continuity of care, and sharing of care across a range of providers are also recommended.16 National guidelines outline context- and population-specific interventions, and routine and targeted maternal health tests during different stages of pregnancy.
Recommended postnatal care includes at least four postnatal assessments in the 6 weeks following delivery (and delivery-related care for the mother and newborn). These visits should include clinical assessment and care, breastfeeding support, emotional wellbeing and other risk assessment (for example, food security, safety, housing, smoking, alcohol and other drug use), contraception advice and psychosocial support.17
Findings: quality of maternal health care
The data presented below on the quality of maternal care come mainly from nine research papers and key reports published by the Audit and Best Practice for Chronic Disease Continuous Quality Improvement Research research program between 2010 and 2018. Studies analysed more than 4,402 records of Aboriginal and Torres Strait Islander mothers with infants aged between 2 and 14 months, and 242 systems assessments completed by PHC teams. Audit data were collected from 91 health centres serving Aboriginal and Torres Strait Islander populations between 2007 and 2014; these are the most recent audit data available for analysis. Stakeholders participated in data interpretation to identify priority evidence–practice gaps and factors influencing improvement.
Comprehensive maternal primary health care
The maternal health clinical audit tool and protocol18 were used to collect data about the delivery of pregnancy and postnatal services. The data were analysed to assess how well the services reflected best-practice guidelines for maternal care. In general, pregnancy care was delivered at higher levels than postnatal care and there was also less variation between health centres in the delivery of antenatal care compared with postnatal care, indicating a need for increased emphasis on improving postnatal care as part of our efforts to improve maternal PHC in general.
Overall pregnancy care
The results for delivery of antenatal care brought together audit data for the recording of pregnancy risk factors, routine antenatal checks, laboratory investigations and brief interventions and counselling. (The audit tool contained these 26 best-practice indicators: seven or more antenatal visits; estimated gestational age is 13 weeks or less at the first antenatal visit; blood pressure recorded (in the first, second and third trimesters); urinalysis undertaken (in the first and second trimesters); body mass index recorded (in the first trimester); fundal height recorded (second and third trimesters); foetal movements recorded (third trimester); blood glucose level recorded (second trimester); blood group recorded; antibody, rubella and hepatitis B status recorded; mid-stream urine test; full blood examination; syphilis serology; PCR test for HIV; smoking and drinking (alcohol) status recorded (first and third trimesters); social risk and emotional wellbeing assessments conducted; plans for care and birthing discussed; nutrition discussed; domestic, social environment and cultural considerations discussed.)
These were the observations for PHC centres that completed maternal health audit cycles between 2007 and 2014:
- the average level of overall delivery of pregnancy care ranged between 60 and 80 per cent. This means that, on average, 60–80 per cent of mothers received all 26 best-practice indicators (items of antenatal care) during their pregnancy
- the average level of overall service delivery improved
- variation in the quality of antenatal care between health centres persisted (Figure 13.1).19
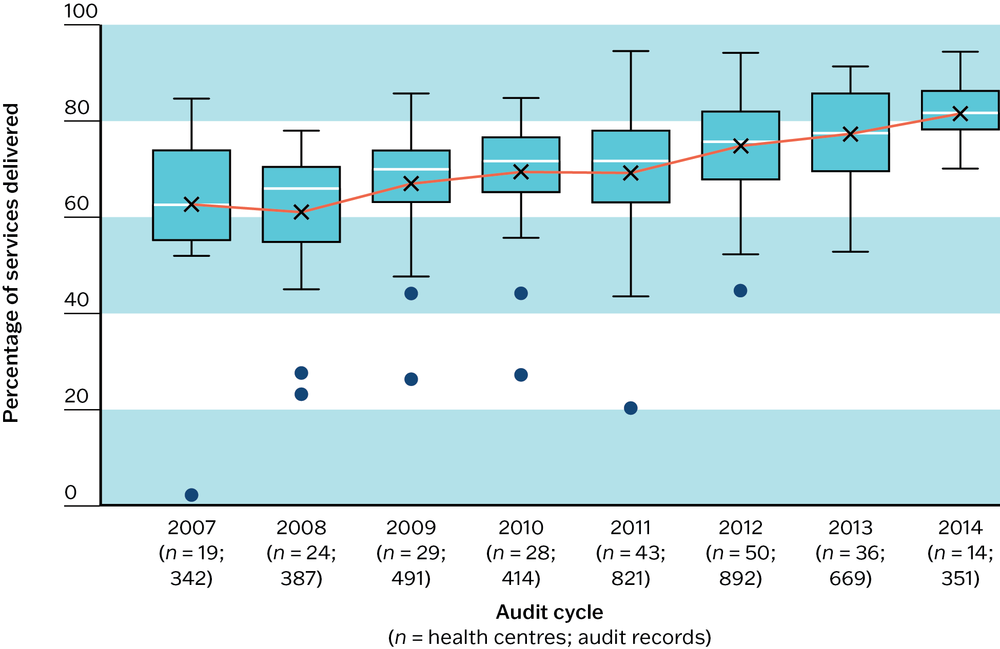
Figure 13.1 Trends in overall pregnancy care. Source: Gibson-Helm, J. Bailie et al. 2016.
Postnatal brief interventions and counselling
The results for delivery of postnatal care focused on the recording of brief interventions and counselling for a range of health risk factors: smoking; nutrition; breastfeeding; infection prevention; injury prevention; sudden infant death syndrome (SIDS) prevention; alcohol and other substance abuse; physical activity; mood (depression); contraception; domestic and social environment; social and family support; financial support; housing condition; and food security.
These were the observations for PHC centres that completed maternal health audit cycles between 2007 and 2014:
- the average level of overall delivery of postnatal care for brief interventions and counselling ranged between 20 and 45 per cent (this means that, on average, 20–45 per cent of mothers received all 15 best-practice indicators for brief interventions and counselling in postnatal care)
- the average level of overall delivery of brief interventions and counselling improved
- wide variation between health centres in the delivery of brief interventions and counselling did not reduce across audit cycles (Figure 13.2).20
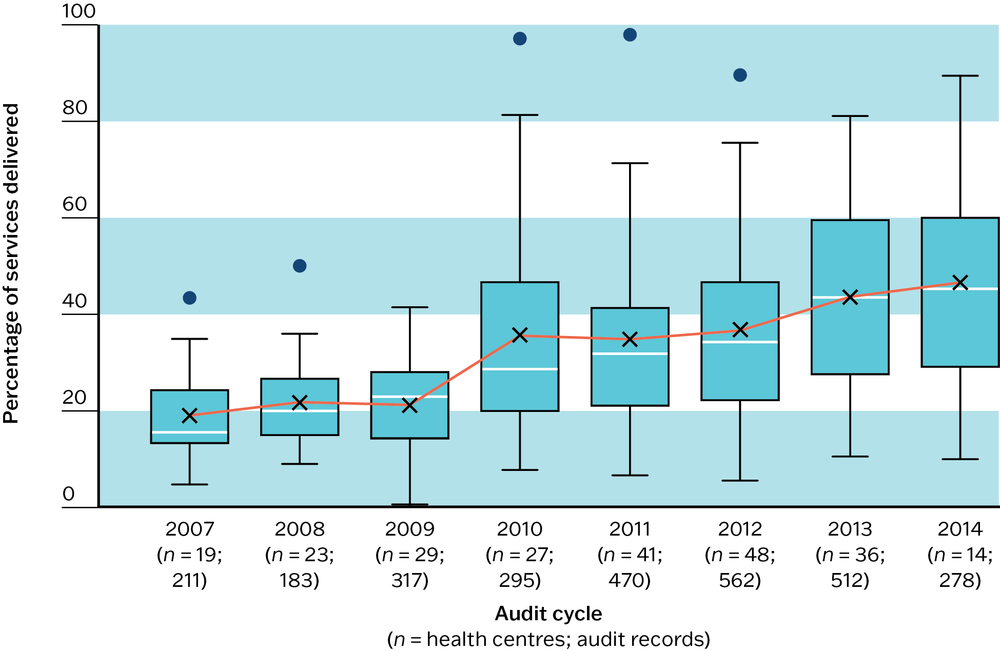
Figure 13.2 Trends in overall postnatal care. Source: Gibson-Helm, J. Bailie et al 2016.
The average level of overall service delivery improved over audit cycles for antenatal and postnatal care.
Routine pregnancy care
Audit data from 65 PHC centres (1,091 patient records, from 2012 to 2014) were analysed in four areas: antenatal visits and care plans; risk factors and brief interventions; laboratory investigations; and routine antenatal checks and abnormal findings.
The findings for antenatal visits and care plans indicated a need to improve care leading up to and during the first months of pregnancy, and to improve communication between hospitals and PHC centres:
- most records (average of 90 per cent, range of 77–100 per cent) contained a pregnancy care plan and a delivery summary from the hospital where the mother gave birth; delivery summaries were less likely to be complete than pregnancy care plans (average of 80 per cent, range of 35–100 per cent)
- there was wide variation in quality of care between health centres for first trimester visits (average of 60 per cent, range of 15–85 per cent), with less variation in quality of care for second and third trimester visits
- recording of folate prescription before pregnancy was low at all health centres (average of 6 per cent, range of 0–25 per cent), suggesting a need to raise community and staff awareness of pre-conception health and pre-conception care.21
For risk factors and brief interventions, the data showed considerable scope for improvement in follow-up for social risk factors and social and physical wellbeing. The findings suggest a need to train and support the workforce to have sensitive conversations with women about social and emotional wellbeing, and to increase options for referral to appropriate local services:
- smoking status, alcohol use, and social and medical risk factors were generally recorded
- follow-up, brief interventions or counselling for physical and social wellbeing were often not provided
- brief interventions for smoking were documented for most women who reported smoking tobacco (almost 85 per cent on average), with lower rates of brief interventions for alcohol use or illicit drug use
- despite very high levels of social and medical risk factor assessments, and follow-up for medical risk factors, follow-up for social risk factors varied greatly. Brief interventions or counselling about maternal wellbeing during pregnancy was not provided in many cases (for example, financial situation, food security, housing environment, cultural considerations). 22
The analysis of data for laboratory investigations had mixed outcomes, with some very good results and some highlighting of areas where improvements can be made:
- levels of laboratory investigations were very high (nearly all over 80 per cent average)
- across PHC centres fewer than 60 per cent of women were offered foetal anomaly screening. This may relate to local availability and accessibility of screening, staff time constraints, communication difficulties caused by language differences (for example, difficulty explaining the concept of risk of foetal abnormalities and testing).23
- the average level of delivery of glucose challenge tests and glucose tolerance tests was high (70–80 per cent), although there was wide variation between health centres (0–100 per cent)24
- follow-up actions for anaemia and abnormal glucose challenge and tolerance tests were generally well done
- follow-up for anti-D injections, during pregnancy and post-birth, and post-birth rubella immunisations was generally not well done.25
As with the other categories of data, the changes here revealed some areas where care provision was widely of a high quality, and other items where quality of care can be substantially improved.
- Most women who attended during the first trimester were weighed (average of 90 per cent; range of 60–100 per cent) (Figure 13.3).
- The recording of body mass index (BMI) varied. On average, it was approximately 60 per cent with a range of 0–100 per cent (Figure 13.3). Many women with an abnormal BMI (average of 30 per cent; range 0–100 per cent), did not have a BMI management plan in their client record (average of 40 per cent; range of 0–100 per cent). The recording of both BMI and BMI management plans varied between PHC centres (Figure 13.3).26
- Most women had their blood pressure measured during antenatal visits at all stages of pregnancy, with a record of follow-up testing if blood pressure was abnormal.27
- Urine sample analysis was provided at relatively high levels at all stages, but there was wide variation in subsequent mid-stream urine tests following abnormal urinalysis results and this is important for the prevention of preterm labour.28
- Nearly all women received fundal height, foetal heart rate and foetal movement checks, but women with a record of abnormal foetal movement had little or no record of follow-up use of kick charts. Cardiotocograph monitoring or referral to a specialist service varied widely, possibly due to lack of access to equipment or specialist.29
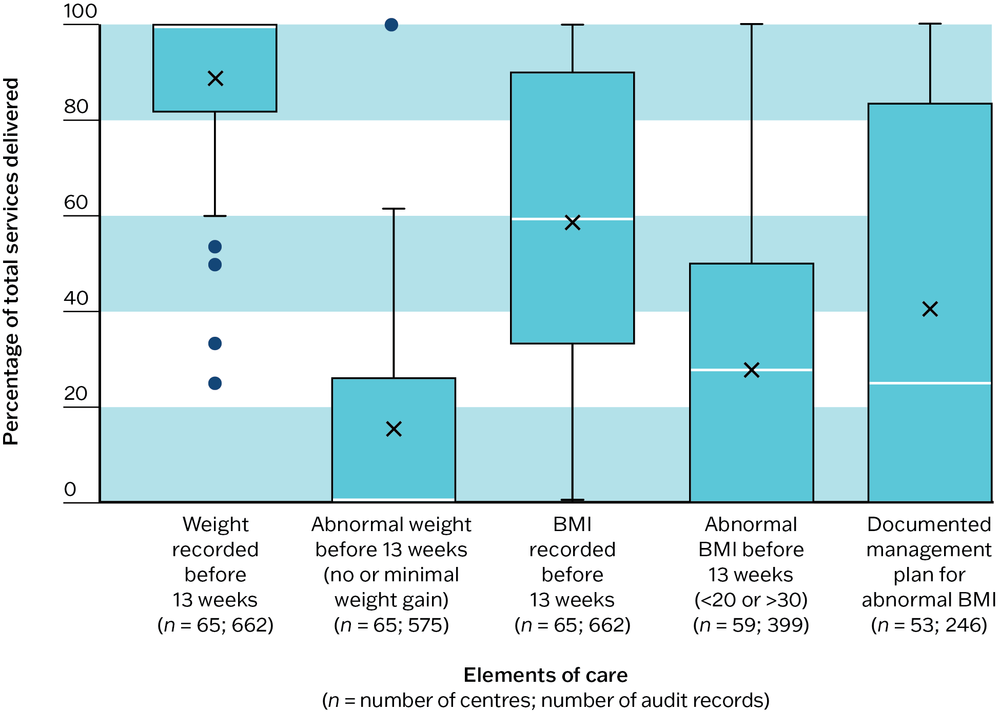
Figure 13.3 Record of scheduled maternal care services received by Indigenous women at Indigenous primary health care centres, 2012–2014. Source: J. Bailie, Boyle and R. Bailie 2018.
Routine postnatal care
Analysis of audit data from 65 PHC centres (1,091 patient records, 2012–14) revealed a need to improve discussion and brief interventions for social and physical risk factors as part of routine postnatal care:
- the majority of women had a recorded postnatal visit
- breastfeeding and contraception were usually discussed and recorded in the client’s file
- there was wide variation in discussing and providing brief intervention for nutrition, infection prevention, mood, domestic and social environment, and social and family support
- smoking, injury prevention for the infant, prevention of sudden unexpected death in infancy, the woman’s financial situation, housing and food security were infrequently raised and discussed by PHC staff.30
Social and emotional wellbeing of pregnant women and mothers
The CQI research identified the need to improve social and emotional wellbeing care for pregnant women and mothers, as part of antenatal and postnatal care. This improvement priority was identified from the analysis of maternal health audit data from 65 PHC centres (1,091 audit records; 58 systems assessments; 2012–14) and input from people providing PHC services. The quality of social and emotional wellbeing care was then tracked from 2010 to 2014 to assess trends in care quality.
- Risk of social and emotional distress was associated with factors such as use of alcohol and other drugs.31
- Women attending urban and regional health centres were more likely to be at risk of distress than those attending remote health centres.32
- From 2010 to 2014, the delivery of screening for emotional wellbeing using standard screening tools (for example, PHQ and aPHQ-9) improved steadily.33 Records showed an average of 15 per cent in 2010, when the audit item was introduced, which increased to 60 per cent in 2014 (Figure 13.4a).34
- There was wide and persistent variation between PHC centres in the delivery of screening for emotional wellbeing, ranging from 0 to 100 per cent (Figure 13.4a).35
- Follow-up for women identified as “at risk”, based on assessment of emotional wellbeing during pregnancy, improved. In 2014, follow-up ranged from around 75 to 100 per cent (average of 90 per cent) across PHC centres (Figure 13.4b).36
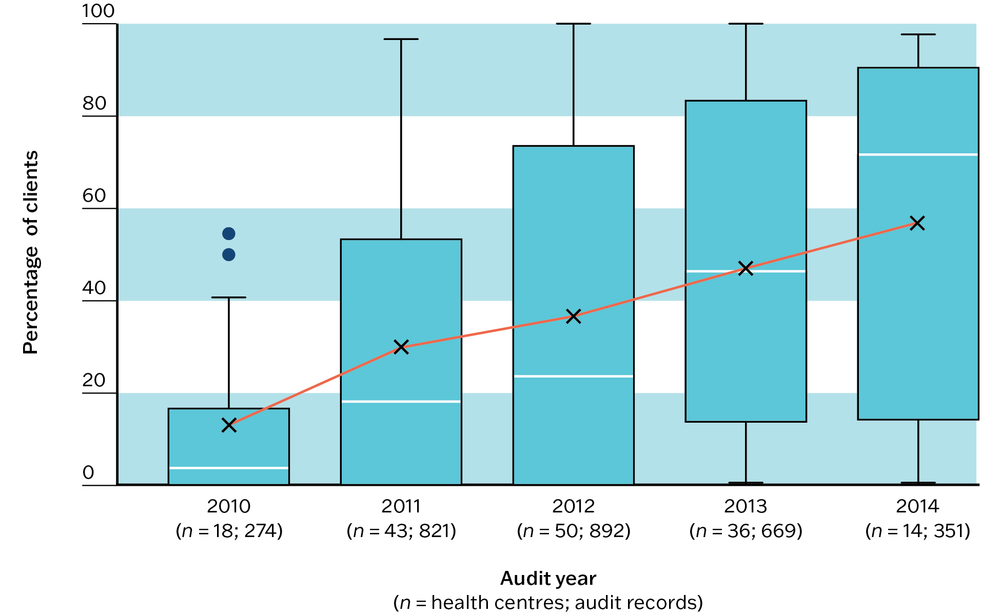
Figure 13.4a Screening for maternal social and emotional wellbeing.
Source: Gibson-Helm, J. Bailie et al. 2018.
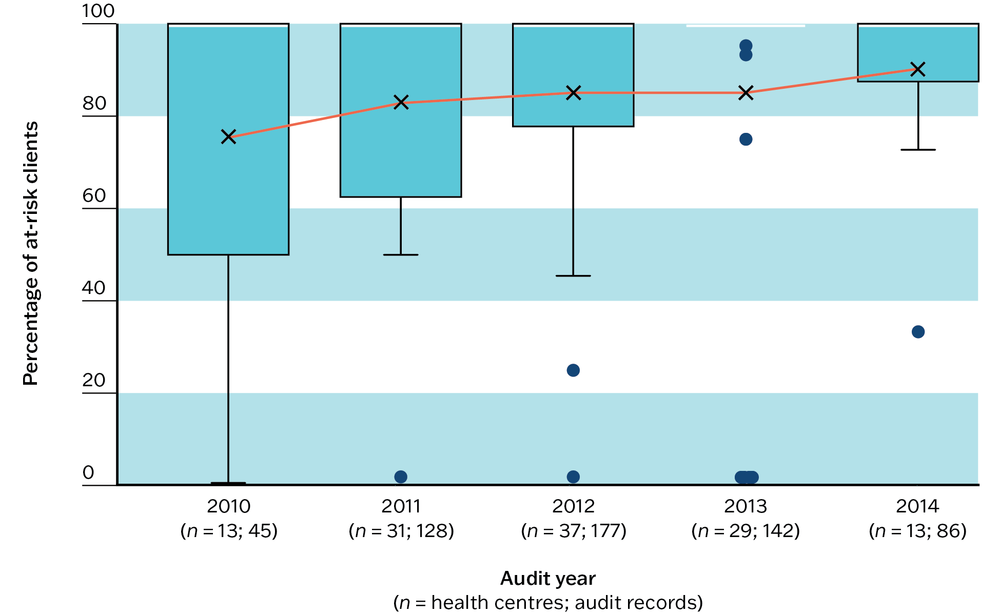
Figure 13.4b Follow-up action for clients identified at risk for social and emotional wellbeing. Source: Gibson-Helm, J. Bailie et al. 2018.
Did using CQI improve maternal care?
Our research found that women who attended a PHC centre that conducted audits for maternal care were more likely to receive recommended screening and brief interventions for lifestyle-related risk factors than women attending centres that did not use CQI.37 Even one cycle of CQI improved screening for BMI, blood pressure and diabetes.38
PHC teams that completed three or more systems assessments for maternal health noted improvements over time in how systems worked to deliver maternal care.39 (For information about the ABCD systems assessment tool, see Chapter 5.)
Women who attended a PHC centre that conducted audits for maternal care were more likely to receive recommended screening and brief interventions for lifestyle-related risk factors than women attending centres that did not use CQI.
Key messages for improving maternal health care in PHC
Common evidence-to-practice gaps in maternal care affect the health of both women and babies. This CQI research identifies clear priorities and strategies for improving maternal health care and includes stakeholder interpretation of CQI data. Patterns of PHC delivery for Aboriginal and Torres Strait Islander maternal care are likely to reflect, at least to some extent, care delivery in international settings.
PHC teams should focus on improving aspects of pregnancy and postnatal care in which there are system-wide evidence-to-practice gaps in delivery. This means improving systems to support best-practice care before, during and after pregnancy:
- Before pregnancy, these activities should be undertaken:
- raising community and staff awareness of pre-conception health and pre-conception care
- offering health promotion and prevention activities (for example, to stop smoking, to support social and emotional wellbeing).
- In pregnancy, as part of routine maternal care, these items of care should be included:
- asking women about smoking and drinking alcohol and providing brief counselling
- assessing social risk factors and emotional wellbeing and taking the appropriate follow-up action.
- At the postnatal visit, these areas should be discussed:
- how a smoking environment increases the risk of sudden unexpected death in infancy
- how to protect babies from harm
- how diet and nutrition are important for the mother and baby.
In addition, follow-up or referral to programs and services as needed should be provided at the postnatal visit.
Encourage women to share decision-making and have an active role in their health care (for example, to make choices about foetal anomaly screening), and develop community-based programs that increase health literacy and raise community expectations of receiving best-practice woman-centred maternal health care.
Health systems should ensure that all PHC providers are empowered and equipped with the necessary skills and resources to deliver continuity of maternal care, including the following:
- systems to coordinate team care (wraparound care) before, during and after pregnancy
- systems to recruit, train and support adequate staff to provide maternal care through a mix of roles (for example, midwives, doctors, medical specialists, community and mental health workers)
- systems and training to support culturally safe care
- training and support for staff to confidently provide best-practice care relating to sensitive issues (for example, conversations about family violence, social and emotional wellbeing)
- clear pathways for referral to local and appropriate services
- appropriate awareness-raising and education resources, and partnering with communities on health promotion and prevention projects and resource development
- partnership with participatory women’s groups and other community groups that connect and support women and their families.
Participate in CQI. Sustained commitment to CQI can improve the quality of maternal health care.
Improving maternal care for Aboriginal and Torres Strait Islander women
Research into the quality of maternal care since 2010 highlights many aspects of care that are being done well by PHC centres serving Aboriginal and Torres Strait Islander communities. It also highlights a need to enhance the delivery of recommended services.40 Despite generally high levels of attendance for antenatal care, an early study across multiple PHC centres found that only one in five Aboriginal and Torres Strait Islander women was screened for depression in pregnancy using a standard screening tool.41 Delivery of this service item has improved, but not sufficiently and not consistently across PHC centres. The development and uptake of place-based screening tools (for example, Kimberley Mum’s Mood Scale42) could help to improve delivery.
There are many examples of variation in service delivery for routine items of maternal care. These common and persistent gaps in care indicate broader system weaknesses and a need to focus on the functioning of organisational systems and the root causes of gaps in care (rather than on isolated issues or staff roles). Establishing systems to train and support PHC staff to use standard screening tools and provide brief interventions and referrals, for example, can improve care for a range of health risk factors and client groups, as long as appropriate referral options are available.
Sustained commitment to CQI can improve the quality of maternal health care.
Australian governments are investing in culturally responsive maternity care, but limited availability of birthing services outside urban centres means that many women who live in remote communities are still separated from family, community and PHC services during the final weeks of their pregnancies and while giving birth. The separation can be a significant stress. The connectedness of Aboriginal and Torres Strait Islander families and communities is a strength and a source of learning and support for mothers. Community-based maternal care, including family-focused programs that enable women to pass on cultural birthing and parenting practices, have potential for improving outcomes. Studies highlight the importance of the relationships established between healthcare teams and mothers, access to Aboriginal and Torres Strait Islander practitioners and other community-based workers, and culturally safe care.43 An evaluation of the Strong Women, Strong Babies, Strong Culture program in the Northern Territory identified several features required for program success, with transferrable lessons for other maternal care initiatives:
- respect for Aboriginal knowledge and practice as a vital component of health care
- organisational commitment for a high level of community participation and control
- competence in intercultural collaborative practice of staff.44
Continuity of care and carer are highly valued by Aboriginal and Torres Strait Islander mothers and present many opportunities for reducing health risks.45 PHC services need to connect well with young women to provide culturally safe preventive care, and to deliver best-practice, woman-centred maternal care before, during and after pregnancy. Good documentation and coordination between hospital and PHC teams is important for reducing health risks for mothers and babies following delivery,46 while continuity of care through an infant’s early years provides further opportunities to improve outcomes.47 In summary, collaboration between health professionals is needed in all phases and women should expect to be provided with information to make informed choices about their care.48
Collaboration between health professionals is needed in all phases and women should expect to be provided with information to make informed choices about their care.
The translation of evidence into policy and clinical practice is a common challenge. Mechanisms and funding support provided through the Closing the Gap and other government programs can increase workforce investment and strengthen systems for effective, culturally appropriate maternal care at higher levels of the system. CQI initiatives within PHC services are key to strengthening systems for high-quality maternal care at the community level, as part of comprehensive, holistic and culturally safe PHC.49
References
Abell, S., A. Nankervis, K. Khan and H. Teede (2016). Type 1 and type 2 diabetes preconception and in pregnancy: health impacts, influence of obesity and lifestyle, and principles of management. Seminars in Reproductive Medicine 34(2): 110–20. DOI: 10.1055/s-0035-1571196.
Australian Institute of Health and Welfare (2024). Diabetes: Australian facts – gestational diabetes. Canberra: Australian Government.
Australian Institute of Health and Welfare (2023). Australia’s mothers and babies. First Nations mothers and babies. Canberra: AIHW.
Australian Institute of Health and Welfare (2021). Australia’s mothers and babies. Canberra: AIHW. https://www.aihw.gov.au/reports/mothers-babies/australias-mothers-babies/contents/about.
Bailie, J., J. Boyle and R. Bailie (2018). Population attributable fractions of perinatal outcomes for nulliparous women associated with overweight and obesity, 1990–2014. Medical Journal of Australia 208(11): 505–6. DOI: 10.5694/mja18.00263.
Bar-Zeev, S., L. Barclay, C. Farrington and S. Kildea (2012). From hospital to home: the quality and safety of a postnatal discharge system used for remote dwelling Aboriginal mothers and infants in the top end of Australia. Midwifery 28(3): 366–73. DOI: 10.1016/j.midw.2011.04.010.
Chamberlain, C., B. Oldenburg, A. Wilson, S. Eades, K. O’Dea, J. Oats et al. (2016). Type 2 diabetes after gestational diabetes: greater than fourfold risk among Indigenous compared with non-Indigenous Australian women. Diabetes/Metabolism Research and Reviews 32(2): 217–27. DOI: 10.1002/dmrr.2715.
Crinall, B., J. Boyle, M. Gibson-Helm, D. Esler, S. Larkins and R. Bailie (2017). Cardiovascular disease risk in young Indigenous Australians: a snapshot of current preventive health care. Australian and New Zealand Journal of Public Health 41(5): 460–6. DOI: 10.1111/1753-6405.12547.
Cunningham, J. and Y. Paradies (2012). Socio-demographic factors and psychological distress in Indigenous and non-Indigenous Australian adults aged 18–64 years: analysis of national survey data. BMC Public Health 12(1 Feb 2012): 95. DOI: 10.1186/1471-2458-12-95.
Dabelea, D. (2007). The predisposition to obesity and diabetes in offspring of diabetic mothers. Diabetes Care 30(Supplement_2): S169–S74. DOI: 10.2337/dc07-s211.
Ding, X., Y. Wu, S. Xu, R. Zhu, X. Jia, S. Zhang et al. (2014). Maternal anxiety during pregnancy and adverse birth outcomes: a systematic review and meta-analysis of prospective cohort studies. Journal of Affective Disorders 159: 103–10. DOI: 10.1016/j.jad.2014.02.027.
Freemantle, J. and L. Ellis (2018). An Australian perspective. In J.R. Duncan and R.W. Byard (eds), SIDS sudden infant and early childhood death: the past, the present and the future. Adelaide: University of Adelaide Press. https://www.ncbi.nlm.nih.gov/books/NBK513382/.
Gausia, K., S. Thompson, T. Nagel, A. Rumbold, C. Connors, V. Matthews et al. (2013). Antenatal emotional wellbeing screening in Aboriginal and Torres Strait Islander primary health care services in Australia. Contemporary Nurse: A Journal for the Australian Nursing Profession 46(1): 73–82. DOI: 10.5172/conu.2013.46.1.73.
Gausia, K., S.C. Thompson, T. Nagel, G. Schierhout, V. Matthews and R. Bailie (2015). Risk of antenatal psychosocial distress in indigenous women and its management at primary health care centres in Australia. General Hospital Psychiatry 37(4): 335–9. DOI: 10.1016/j.genhosppsych.2015.04.005.
Gibson-Helm, M., J. Bailie, V. Matthews, A. Laycock, J. Boyle and R. Bailie (2018). Identifying evidence–practice gaps and strategies for improvement in Aboriginal and Torres Strait Islander maternal health care. PLOS One 13(2): e0192262. DOI: 10.1371/journal.pone.0192262.
Gibson-Helm, M., J. Bailie, V. Matthews, A. Laycock, J. Boyle and R. Bailie (2016). Priority evidence–practice gaps in Aboriginal and Torres Strait Islander maternal health care final report: engaging stakeholders in identifying priority evidence–practice gaps and strategies for improvement in primary health care (ESP project). Brisbane: Menzies School of Health Research.
Gibson-Helm, M., A. Rumbold, H. Teede, S. Ranasinha, R. Bailie and J. Boyle (2016). Improving the provision of pregnancy care for Aboriginal and Torres Strait Islander women: a continuous quality improvement initiative. BMC Pregnancy and Childbirth 16(118). DOI: 10.1186/s12884-016-0892-1.
Gibson-Helm, M., H. Teede, A. Rumbold, S. Ranasinha, R. Bailie and J. Boyle (2015). Continuous quality improvement and metabolic screening during pregnancy at primary health centres attended by Aboriginal and Torres Strait Islander women. Medical Journal of Australia 203(9): 369.e1–69.e7. DOI: 10.5694/mja14.01660.
Harfield, S., C. Davy, A. McArthur, Z. Munn, A. Brown and N. Brown (2018). Characteristics of Indigenous primary health care service delivery models: a systematic scoping review. Globalization Health 14(1): 12. DOI: 10.1186/s12992-018-0332-2.
Heazell, A. (2020). Need to ensure that improvements in stillbirth rates are also achieved in high-risk groups. Paediatric and Perinatal Epidemiology 34(1): 1–2. DOI: https://doi.org/10.1111/ppe.12609.
Kildea, S., S. Hickey, C. Nelson, J. Currie, A. Carson, M. Reynolds et al. (2018). Birthing on Country (in our community): a case study of engaging stakeholders and developing a best-practice Indigenous maternity service in an urban setting. Australian Health Review 42(2): 230–8. DOI: 10.1071/AH16218.
Kildea, S., H. Stapleton, R. Murphy, N.B. Low and K. Gibbons (2012). The Murri clinic: a comparative retrospective study of an antenatal clinic developed for Aboriginal and Torres Strait Islander women. BMC Pregnancy and Childbirth 12(1): 159. DOI: 10.1186/1471-2393-12-159.
Lee, A., R. Hiscock, P. Wein, S. Walker and M. Permezel (2007). Gestational diabetes mellitus: clinical predictors and long-term risk of developing type 2 diabetes: a retrospective cohort study using survival analysis. Diabetes Care 30(4): 878–83. DOI: 10.2337/dc06-1816.
Lowell, A., S. Kildea, M. Liddle, B. Cox and B. Paterson (2015). Supporting Aboriginal knowledge and practice in health care: lessons from a qualitative evaluation of the Strong Women, Strong Babies, Strong Culture program. BMC Pregnancy and Childbirth 15(1): 19. DOI: 10.1186/s12884-015-0433-3.
MacKay, D., R. Kirkham, N. Freeman, K. Murtha, P. Van Dokkum, J. Boyle et al. (2020). Improving systems of care during and after a pregnancy complicated by hyperglycaemia: a protocol for a complex health systems intervention. BMC Health Services Research 20(1): 814. DOI: 10.1186/s12913-020-05680-x.
Marley, J., J. Kotz, C. Engelke, M. Williams, D. Stephen, S. Coutinho et al. (2017). Validity and acceptability of Kimberley Mum’s Mood Scale to screen for perinatal anxiety and depression in remote Aboriginal health care settings. PLOS One 12(1): e0168969. DOI: 10.1371/journal.pone.0168969.
Marmot, M., P. Goldblatt, J. Allen, et al. Fair society, healthy lives (The Marmot Review). London: Institute of Health Equity.
McCalman, J. (2014). Evaluating the Baby Basket program in north Queensland. Lowitja Institute. https://www.lowitja.org.au/projects/baby-basket/.
McMillen, I. and J. Robinson (2005). Developmental origins of the metabolic syndrome: prediction, plasticity, and programming. Physiological Reviews 85(2): 571–633. DOI: 10.1152/physrev.00053.2003.
Menzies School of Health Research and One21seventy (2014). Maternal health clinical audit tool. One21seventy. Brisbane: Menzies School of Health Research.
Royal Australian and New Zealand College of Obstetricians and Gynaecologists (2017). Maternity care in Australia: a framework for a healthy new generation of Australians. https://ranzcog.edu.au/wp-content/uploads/2022/01/Maternity-Care-in-Australia-Web.pdf.
Rumbold, A., R. Bailie, D. Si, M. Dowden, C. Kennedy, R. Cox et al. (2011). Delivery of maternal health care in Indigenous primary care services: baseline data for an ongoing quality improvement initiative. BMC Pregnancy and Childbirth 11(1): 16. DOI: 10.1186/1471-2393-11-16.
Rumbold, A., K. Wild, E. Maypilama, S. Kildea, L. Barclay, E. Wallace et al. (2015). Challenges to providing fetal anomaly testing in a cross-cultural environment: experiences of practitioners caring for Aboriginal women. Birth (Berkeley, Calif.) 42(4): 362–8. DOI: 10.1111/birt.12182.
Saigal, S. and L. Doyle (2008). An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 371(9608): 261–9. DOI: 10.1016/S0140-6736(08)60136-1.
Sivertsen, N., O. Anikeeva, J. Deverix and J. Grant (2020). Aboriginal and Torres Strait Islander family access to continuity of health care services in the first 1000 days of life: a systematic review of the literature. BMC Health Services Research 20(1): 829. DOI: 10.1186/s12913-020-05673-w.
White Ribbon Alliance (2011). The respectful maternity care charter: the universal rights of childbearing women. Washington: White Ribbon Alliance. http://www.healthpolicyproject.com/index.cfm?ID=publications&get=pubID&pubID=46.
World Health Organization (2020). Global Health Observatory (GHO) data. Infant mortality: situations and trends. Geneva, Switzerland: WHO.
World Health Organization (2019). Maternal mortality. Fact sheets. https://www.who.int/news-room/fact-sheets/detail/maternal-mortality.
World Health Organization (2016). WHO recommendations on antenatal care for a positive pregnancy experience. https://www.who.int/reproductivehealth/publications/maternal_perinatal_health/anc-positive-pregnancy-experience/en/.
World Health Organization (2015). Postnatal care for mothers and newborns: highlights from the World Health Organization 2013 guidelines. Geneva, Switzerland: WHO.
1 World Health Organization 2020.
2 World Health Organization 2019.
3 Marmot, M., P. Goldblatt, J. Allen, et al. 2010.
4 White Ribbon Alliance 2011; World Health Organization 2016.
5 Australian Institute of Health and Welfare 2023.
6 Australian Institute of Health and Welfare 2021.
7 Freemantle and Ellis 2018; Heazell 2020.
8 Marmot, M., P. Goldblatt, J. Allen, et al. 2010.
9 Australian Institute of Health and Welfare 2024.
10 Chamberlain, Oldenburg et al. 2016.
11 Dabelea 2007; MacKay, Kirkham et al. 2020.
12 McMillen and Robinson 2005; Saigal and Doyle 2008.
13 Crinall, Boyle et al. 2017.
14 Abell, Nankervis et al. 2016; Lee, Hiscock et al. 2007.
15 Cunningham and Paradies 2012; Ding, Wu et al. 2014.
16 World Health Organization 2016.
17 World Health Organization 2015.
18 Menzies School of Health Research and One21seventy 2014.
19 Gibson-Helm, J. Bailie et al. 2016.
20 Gibson-Helm, J. Bailie et al. 2016.
21 Gibson-Helm, J. Bailie et al. 2016, data supplement.
22 Gibson-Helm, J. Bailie et al. 2016, Gibson-Helm, Teede et al. 2015.
23 Gibson-Helm, J. Bailie et al. 2016, data supplement; Rumbold, Wild et al. 2015.
24 Note that screening for diabetes has changed since these data were collected.
25 Gibson-Helm, J. Bailie et al. 2016, data supplement.
26 J. Bailie, Boyle and R. Bailie 2018.
27 Gibson-Helm, J. Bailie et al. 2016.
28 Gibson-Helm, J.Bailie et al. 2016.
29 Gibson-Helm, J. Bailie et al. 2016.
30 Gibson-Helm, J. Bailie et al. 2016.
31 Gausia, Thompson et al. 2015.
32 Gausia, Thompson et al. 2015.
33 For culture-specific screening tools, see Chapters 11 and 15.
34 Gibson-Helm, J. Bailie et al. 2016, 2018.
35 Gibson-Helm, J. Bailie et al. 2016, 2018.
36 Gibson-Helm, J. Bailie et al. 2016, 2018.
37 J. Bailie, Boyle and R. Bailie 2018; Gibson-Helm, Rumbold et al. 2016; Gibson Helm, J. Bailie et al. 2018.
38 Gibson-Helm, Teede et al. 2015.
39 Gibson-Helm, Teede et al. 2015.
40 Gibson-Helm, Rumbold et al. 2016; Gibson-Helm, Teede et al. 2015; Rumbold, R. Bailie et al. 2011.
41 Gausia, Thompson et al. 2013.
42 Marley, Kotz et al. 2017.
43 Gibson-Helm, J. Bailie et al. 2016, 2018; Kildea, Hickey et al. 2018; Kildea, Stapleton et al. 2012; McCalman 2014.
44 Lowell, Kildea et al. 2015.
45 Sivertsen, Anikeeva et al. 2020.
46 Bar-Zeev, Barclay et al. 2012.
47 Sivertsen, Anikeeva et al. 2020.
48 Royal Australian and New Zealand College of Obstetricians and Gynaecologists 2017.
49 Harfield, Davy et al. 2018.