19
Improving eye health care
Eye health care
In primary health care (PHC), best practice for eye care is part of a client-centred, holistic approach to child health, preventive care and the management of chronic conditions such as diabetes. When linked with eye care referral processes and appropriate and accessible treatment, regular eye examinations and vision assessments can help to identify and refer eye problems earlier, preventing vision loss.
Poorer people suffer far more blindness and visual impairment than wealthier populations. This is partly due to untreated diseases, such as corneal infections, and to the persistence of infectious diseases linked to poor living conditions, such as trachoma.1 Trachoma is generally found in dry and dusty environments, where transmission of the infecting organism – Chlamydia trachomatis – is enabled by household crowding, limited access to and use of water, and poor waste disposal systems. It is a major cause of preventable blindness globally and is endemic in 44 countries, with children having more frequent and longer lasting episodes of infection than adults.2 Multiple trachoma infections can lead to an eyelid abnormality called trichiasis. While the underlying causes of trachoma and associated blindness are socio-economic and environmental, a related cause of visual impairment from trachoma and other causes is lack of access to ophthalmic services that can help to prevent or treat a variety of conditions that can lead to blindness. In low-income countries, only a small fraction of those who need eye care services get them.3
PHC practitioners have an important role in vision screening, referral to eye care services and case management. They support and coordinate clients’ timely access to comprehensive eye examinations and specialist eye care, particularly for clients with chronic conditions such as diabetes. The critical nature of this role is more apparent in rural and remote locations where specialist eye health services are typically provided by visiting practitioners, and where a shortage of optometric and ophthalmic services often results in lower rates of eye examinations.4
Aboriginal and Torres Strait Islander peoples
Aboriginal and Torres Strait Islander people, as a population, face higher rates of vision loss than other Australians.5 Many cases of vision loss (94 per cent) are avoidable, preventable or treatable.6 Over the past decade and more, the gap in eye health and vision for Aboriginal and Torres Strait Islander people has halved through the collective efforts of individuals, organisations and governments. However, too many Aboriginal and Torres Strait Islander people still experience avoidable vision loss and blindness, and those who have lost vision often find it difficult to access the support and services they need.7
The factors that contribute to eye health are complex. They may include past eye health, access to eye health services, the complexity of the health system and continuity of care, and medical factors (for example, low birth weight, diabetes, high blood pressure). Having diabetes can lead to diabetic retinopathy and accelerate the development of cataracts. Living conditions (for example, housing and sanitation facilities), environmental conditions (for example, dust, access to water, assess to good food), health behaviours (for example, diet, alcohol and tobacco use), education and income are also linked with eye health.8
Aboriginal and Torres Strait Islander adults older than 40 years with diabetes form 72 per cent of those requiring an eye examination in any year.9 In addition, Australia is the only high-income country in the world where trachoma is endemic. Trachoma currently occurs in remote and very remote communities in the Northern Territory, South Australia and Western Australia. In 2014, jurisdictions identified 160 communities as being at risk or potentially at risk of trachoma; 115 communities were identified as being at risk in 2019;10 and 92 in 2021.11 While the risk and prevalence of trachoma have declined, elimination will be difficult unless living conditions are improved.
The national guide on eye and vision assessments for Aboriginal and Torres Strait Islander peoples12 makes these recommendations:
- People with diabetes should have a recorded annual visual acuity assessment with a dilated eye examination or retinal photograph. This includes the use of retinal photography by trained PHC staff combined with review by an ophthalmologist.13
- Adults aged over 40 years with no diagnosed major chronic disease should have a recorded visual acuity assessment, and, for those who lived in trachoma endemic areas as children, a trichiasis assessment every two years.
- Infants and children should have these checks:
- a general eye examination before 3 months of age and again between 3 and 6 months of age
- screening for visual acuity as part of a routine health assessment at or before starting school, for children aged 3–5 years
- a record of any parental concern around vision, and an eye examination and visual acuity assessment every one to two years, as part of a routine health check
- a recorded annual trachoma examination if living in at-risk regions for trachoma; this is part of the annual health check and annual screening done by public health teams for children living in endemic areas.14
Findings: quality of eye health care
Three standardised audit tools were used to collect data about the delivery of eye and vision services: those for type 2 diabetes, preventive health and child health. Information on the application of CQI for these aspects of PHC are reported and cited in Chapters 10–12. Our research on the quality of eye care analysed data from 124 PHC centres and 15,175 client records audited between 2005 and 2012.15
The research found that the delivery of recommended eye and vision assessments varied widely between PHC centres and between different aspects of eye care (see Figure 19.1). While some centres provided excellent levels of assessments, others provided low levels. Overall, audited records across three client groups (total n = 7,320 clients) showed routine eye and vision assessments for adults and children were not being recorded at the recommended levels:
- Adults with diabetes: 46 per cent had a visual acuity assessment and 33 per cent had received a retinal examination within the previous 12 months.
- Adults with no diagnosed major chronic disease: 31 per cent of 759 clients had had a visual acuity assessment recorded within the last two years. Only 13 per cent of 2,829 records examined showed that clients had received an examination for trichiasis; it was unknown how many had lived in areas where trachoma was endemic when they were children.
- Children: 49 per cent of 4,909 children had a vision assessment recorded within the past 12 months; 45 per cent had had an eye examination and 25 per cent of 893 of children in affected areas had had a recorded examination for trachoma.16
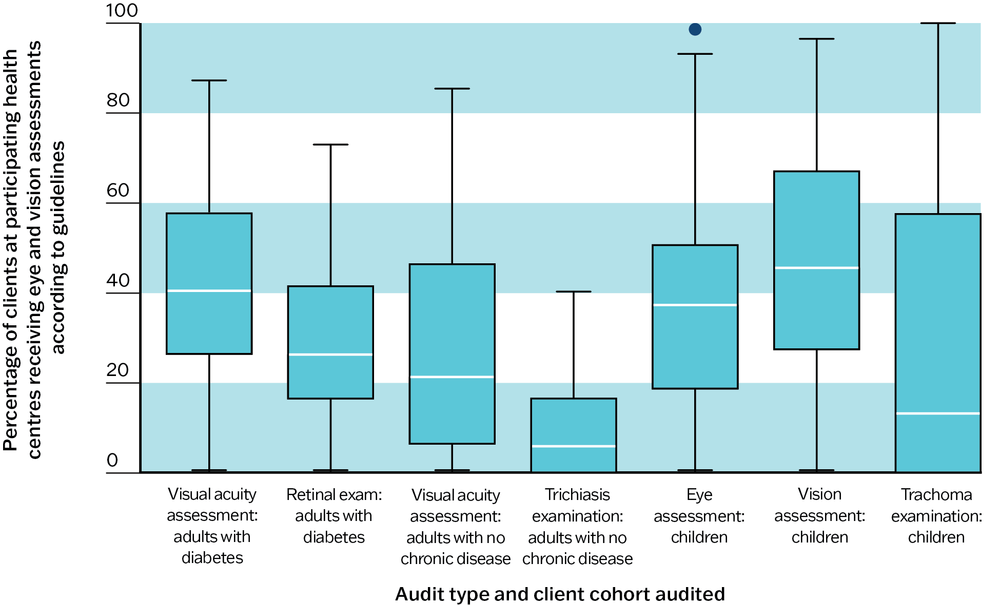
Figure 19.1 Variation in delivery of eye and vision assessments to Aboriginal and Torres Strait Islander clients across participating health centres. Source: Burnett, Morse et al. 2016.
Key messages for improving the delivery of eye care in PHC
A shared challenge for many PHC teams and for populations worldwide is that specialist eye health services are not delivered by local staff. Trachoma screening is generally provided by visiting public health teams, while retinal examinations are often done by visiting or off-site eye practitioners, particularly in under-served rural and remote areas.17
The patterns of eye care delivery in Aboriginal and Torres Strait Islander PHC communities are likely to be consistent with eye care delivery in other settings internationally, and in populations that experience a high burden of chronic illness. This CQI research identifies priorities for improvement and offers messages for improving the delivery of eye care in PHC:
- eye health and vision loss screening should be done in PHC services when resources are available (for example, retinal cameras and trained PHC staff)
- systems need to be in place to support coordination between external or visiting eye care services and programs and PHC centres:
- when possible, integrate specialist eye health services (such as retinal examinations) provided by visiting or off-site eye practitioners around routine PHC delivery
- ensure that examinations conducted by external providers and specialised programs, such as trachoma screening, are recorded in client files
- client records need to include accurate recording of the delivery of eye care; this is important for supporting coordinated and holistic care, and for providing data for CQI with the aim of improving client care
- PHC practitioners require knowledge about the risk of vision loss for patients with diabetes and in trachoma affected areas, and skills to conduct and record visual acuity assessments and eye examinations
- clients’ chronic disease management plans should include regular visual acuity assessment and eye examinations
- clients with diabetes, their carers and families need to be aware of the increased risk of vision loss, and clients should be encouraged to access eye care services and to report vision issues.
Improving eye health care in Aboriginal and Torres Strait Islander PHC
Overall, routine eye and vision assessments for Aboriginal and Torres Strait Islander adults and children attending PHC centres are not generally being recorded at the recommended levels, with considerable variation between health centres. There is continuing need to significantly increase the percentage of Aboriginal and Torres Strait Islander people with diabetes who receive the recommended eye examinations, and to increase eye health and vision loss screening generally. Good vision is important in its own right, but people with diabetes need good vision to look after medications, check their blood glucose levels and feet, and to attend healthcare appointments unassisted.18 Around 60 per cent of vision loss amongst Aboriginal and Torres Strait Islander people can be addressed through access to affordable glasses, and those with vision loss due to cataract or diabetic eye disease require culturally sensitive treatment pathways.19
The higher likelihood of clients with diabetes to have a visual acuity assessment recorded (46 per cent) than adults with no diagnosed major chronic disease (31 per cent)20 may be due to several factors. It may reflect stricter adherence to routine screening and regular monitoring for clients with diabetes through their chronic disease management plans, or practitioners’ knowledge of the risk of vision loss for clients with diabetes. Higher rates of testing for people with diabetes may be because annual visual acuity assessments are recommended for people with diabetes, whereas for other adults the recommended frequency for eye examinations may be every two years or less often. It could be that clients with diabetes report issues with their vision or have a higher level of engagement in their health care. Action needs to be taken by PHC teams based on interpretation of local CQI data, while recognising the need to increase delivery of eye health services across all at-risk groups.
Action needs to be taken by PHC teams based on interpretation of local CQI data, while recognising the need to increase delivery of eye health services across all at-risk groups.
Until recently, retinal examinations largely relied on services being provided by visiting or off-site eye practitioners. A Medical Benefits Scheme item enabling visual acuity testing and retinal photography to be done by PHC practitioners as part of a health assessment (MBS 715) was introduced in 2016.21 Use of retinal photo-screening integrated with primary care, image grading, and reporting systems has improved screening outcomes among other Australians who have diabetes.22 This strategy is expected to increase rates of examinations in Aboriginal and Torres Strait Islander PHC centres.
The low level of recording of trachoma examinations in this research – 40 per cent of children from the Northern Territory and fewer than 10 per cent of children in other at-risk areas – is not consistent with the screening rates of 63 to 92 per cent recorded by the National Trachoma Surveillance and Reporting Unit in 2014,23 or more recent screening rates (for example, 95 per cent overall in at-risk communities in 2021).24 Not all remote communities are at risk, which complicates comparisons. Nonetheless, these earlier CQI results indicate a failure to record the trachoma examinations conducted by the jurisdictional trachoma screening programs in children’s clinical records held by PHC services, rather than a failure to screen. This suggests a need for better coordination and communication between external service providers and PHC teams. The living conditions that underly trachoma transmission in remote communities must also be addressed through a reliable and easily accessible clean water supply to households alongside raised community awareness, better supply of housing, and training of PHC staff to screen for trachoma and trichiasis.
Since this CQI research was undertaken, considerable progress has been made. Mandatory inclusion of vision tests is now included in adult health assessments. A five-year plan for Aboriginal and Torres Strait Islander eye health and vision (2019–2024) is being implemented. The plan has four action areas: enhanced service delivery through service expansion and flexible and community-led models; strengthened regional partnerships and local supports; embedded eye health in Indigenous community-controlled health services and other PHC organisations; a multifaceted strategy to eliminate trachoma.25
As in other areas of PHC, a priority is equitable outcomes and access to high-quality eye health and vision care services for Aboriginal and Torres Strait Islander peoples. Aboriginal and Torres Strait Islander peoples should be empowered to shape and lead how they receive services. Ongoing CQI research will examine whether policy support and increased resources for eye health and vision screening have had a significant effect on rates of recorded eye assessments and eye health.
References
Askew, D., P. Schluter, G. Spurling, C. Maher, P. Cranstoun, C. Kennedy et al. (2009). Diabetic retinopathy screening in general practice: a pilot study. Australian Family Physician 38(8): 650–6.
Australian Institute of Health and Welfare (2020). Indigenous eye health measures 2020. Cat. no. IHW 231. Canberra: AIHW.
Burnett, A., A. Morse, T. Naduvilath, A. Boudville, H.R. Taylor and R. Bailie (2016). Delivery of eye and vision services in Aboriginal and Torres Strait Islander primary health care centers. Frontiers in Public Health 4: 276. DOI: 10.3389/fpubh.2016.00276.
Crossland, L., D. Askew, R. Ware, P. Cranstoun, P. Mitchell, A. Bryett et al. (2016). Diabetic retinopathy screening and monitoring of early stage disease in Australian general practice: tackling preventable blindness within a chronic care model. Journal of Diabetes Research 8405395. DOI: 10.1155/2016/ 8405395.
Kelaher, M., A. Ferdinand and H. Taylor (2012). Access to eye health services among indigenous Australians: an area level analysis. BMC Ophthalmology 12(1): 51. DOI: 10.1186/1471-2415-12-51.
National Aboriginal Community Controlled Health Organisation and Royal Australian College of General Practitioners (2024). National guide to a preventative health assessment for Aboriginal and Torres Strait Islander People, 4th edn. Melbourne: RACGP.
National Health and Medical Research Council (2008). Guidelines for the management of diabetic retinopathy. Canberra: Australian Diabetes Society for the Department of Health and Ageing.
Sommer, A., H. Taylor, T. Ravilla, S. West, T. Lietman, J. Keenan et al. (2014). Challenges of ophthalmic care in the developing world. JAMA Ophthalmology 132(5): 640–4. DOI: 10.1001/jamaophthalmol.2014.84.
Tapp, R., A. Boudville, M. Abouzeid, M. Anjou and H. Taylor (2015). Impact of diabetes on eye care service needs: the National Indigenous Eye Health Survey. Clinical and Experimental Ophthalmology 43(6): 540–3. DOI: 10.1111/ceo.12499.
Taylor, H. (2017). A game changer for eye care for diabetes. Medical Journal of Australia 206(1): 8–9. DOI: 10.5694/mja16.00647.
Taylor, H., M. Anjou, A. Boudville and R. McNeil (2012). The roadmap to close the gap for vision: full report. Melbourne: Indigenous Eye Health Unit, Melbourne School of Population Health.
Taylor, H., J. Keeffe, A. Arnold, R. Dunn, S. Fox, N. Goujon et al. (2009). National Indigenous Eye Health Survey, minum barreng (tracking eyes). Melbourne: School of Population Health, University of Melbourne.
Taylor, H. and E. Stanford (2010). Provision of Indigenous eye health services. Melbourne: School of Population Health Indigenous Eye Health Unit, University of Melbourne.
The Kirby Institute (2020). Australian Trachoma Surveillance Report 2019. Sydney: University of New South Wales.
The Kirby Institute (2015). Australian Trachoma Surveillance Report 2014. Sydney: University of New South Wales.
The Kirby Institute and WHO Collaborating Centre in Neglected Tropical Diseases (2022). Australian Trachoma Surveillance Report 2021. Sydney: University of New South Wales.
Vision 2020 Australia (2019). Strong eyes, strong communities: a five year plan for Aboriginal and Torres Strait Islander eye health and vision 2019–2024. Melbourne: Vision 2020. https://www.vision2020australia.org.au/resources/strong-eyes-strong-communities/.
World Health Organization (2022). Trachoma. Fact sheets. https://www.who.int/news-room/fact-sheets/detail/trachoma.
1 Sommer, Taylor et al. 2014.
2 World Health Organization 2022.
3 Sommer, Taylor et al. 2014.
4 Kelaher, Ferdinand and Taylor 2012; Taylor and Stanford 2010.
5 Taylor and Stanford 2010.
6 Taylor, Keeffe et al. 2009.
7 Vision 2020 Australia 2019.
8 Australian Institute of Health and Welfare 2020; Taylor, Anjou et al. 2012.
9 Tapp, Boudville et al. 2015.
10 The Kirby Institute 2015, 2020.
11 The Kirby Institute and WHO Collaborating Centre in Neglected Tropical Diseases 2022.
12 National Aboriginal Community Controlled Health Organisation and Royal Australian College 2024.
13 National Health and Medical Research Council 2008.
14 National Aboriginal Community Controlled Health Organisation and Royal Australian College 2024.
15 Burnett, Morse et al. 2016.
16 Burnett, Morse et al. 2016.
17 Sommer, Taylor et al. 2014.
18 Taylor 2017.
19 Vision 2020 Australia 2019.
20 Burnett, Morse et al. 2016.
21 Taylor 2017.
22 Askew, Schluter et al. 2009; Crossland, Askew et al. 2016.
23 The Kirby Institute 2015.
24 The Kirby Institute and WHO Collaborating Centre in Neglected Tropical Diseases 2022.
25 Vision 2020 Australia 2019.