18
Improving the quality of care for sexually transmissible infections
Sexual health and sexually transmissible infections
Best practice for sexual and reproductive health in primary health care (PHC) is part of a client-centred, holistic approach to health and human rights. It includes contraception services and maternal care, and covers unsafe abortion, sexually transmissible infections and cancers related to reproduction, sexual violence, and the sexual and reproductive health needs of adolescents.1 This chapter is about improving services for the prevention and control of sexually transmissible infections (STIs).
More than 1 million STIs are acquired every day worldwide, and the majority are asymptomatic. Each year, there are an estimated 374 million new infections with one of four curable STIs: chlamydia, gonorrhoea, syphilis and trichomoniasis.2 More than 500 million people are estimated to have genital infection with herpes simplex virus, while an estimated 300 million women have a human papillomavirus (HPV) infection: the primary cause of cervical cancer and preventable with vaccination.3 STIs are associated with significant morbidity in both women and men (for example, tubal infertility, pelvic inflammatory disease, ectopic pregnancy)4 and also increase the risk of HIV transmission and acquisition.5 STIs can have other serious consequences beyond the direct effect of the infection, such as mother-to-child transmission resulting in stillbirth, neonatal death, low birth weight and prematurity, sepsis and inherited abnormalities.6
Preventive care for STIs includes counselling and behavioural interventions: education, pre- and post-test counselling, condom promotion, and interventions that target high-risk groups (for example, sex workers, men who have sex with men, people who inject drugs) and young people.7
Chlamydia, gonorrhoea, syphilis and trichomoniasis are generally curable with a single course of antibiotics, while antivirals can slow the effects of herpes, HIV and hepatitis B.
In low- and middle-income countries, diagnostic tests are often unavailable or are too expensive (except for rapid testing for syphilis and HIV). As a result, diagnosis and management are often based on recognisable signs and symptoms. This commonly leads to over-treatment and missed treatment (as a majority of STIs have no symptoms). Screening strategies are important. Treatment for the sexual partners of people with STIs is essential.8 PHC should aim to raise public awareness and reduce stigma around STIs and to prevent, diagnose and treat STIs effectively. Training PHC workers to provide these interventions is key.
Improving STI care for Aboriginal and Torres Strait Islander peoples
Chlamydia, gonorrhoea and syphilis are readily treatable STIs that continue to occur at high rates in Australia. They are notifiable STIs in Australia, along with donovanosis. High rates of STIs within Aboriginal and Torres Strait Islander communities are influenced by the social and structural determinants of health, which include access to high-quality PHC that, by definition, is culturally appropriate.9 The notification rates for chlamydia are nearly three times higher among Aboriginal and Torres Strait Islander peoples compared to non-Indigenous Australians; comparative infection rates for gonorrhoea and syphilis are higher again.10 Young people aged 15–29 years are the most affected group, with the highest incidence among 15- to 19-year-olds.11 Identified risk factors for STIs are living in a community with high STI rates; age (being sexually active when younger than 35 years old, especially younger than 25 years); having an STI within the past year, having a new sexual partner; or having more than one partner in the past six months. Drug or alcohol use can be a risk factor for multiple sexual partners or unsafe sex.12
Aboriginal and Torres Strait Islander peoples living in remote and very remote areas experience much higher rates of STIs compared to those in urban and regional areas.13 A decade-long infectious syphilis epidemic has affected almost 4,000 mainly rural young Indigenous people in Queensland, Northern Territory, Western Australia and South Australia.14 Despite remote communities experiencing endemic rates of STIs for well over two decades,15 relatively recent estimates put annual STI testing coverage in remote communities at only 20 per cent, with lower rates in men than in women.16
The National Aboriginal Community Controlled Health Organisation and the Royal Australian College of General Practitioners guidelines for preventive health recommend annual testing for chlamydia (15- to 29-year-old age group) and gonorrhoea (15- to 39-year-old age group) among Aboriginal and Torres Strait Islander clients attending primary healthcare centres.17 Clinical guidelines for communities in the Northern Territory and central Australia recommend at least annual STI testing, prompt treatment, partner notification and testing, repeat testing after a positive result and treatment, education and positive health messages, particularly for those younger than 35 years.18
The CARPA standard treatment manual recommends two standard STI tests a year for men and women, and for sexually active young people (with consent). Testing can be done at these times:
- as part of another consultation (opportunistic), if the client is between 15 and 35 years old
- as part of an adult health check
- as part of community-wide screening
- if symptoms and risk factors suggest STI
- if requested by the client – even if it has not been long since the last check.
Doing STI work in a culturally sensitive way is crucial. Experienced and respected Aboriginal and Torres Strait Islander health practitioners, health councils, and respected community members are important sources of help for non-Indigenous staff.19
Findings: quality of STI care
Preventive health audits of 16,086 client records were conducted at 137 Aboriginal and Torres Strait Islander PHC centres between 2005–06 and 2014 (see Chapter 11). The audits involved government- and community-controlled, urban, regional and remote health centres. Testing and counselling data for sexually transmissible infections were analysed, looking for the levels of variation in testing for chlamydia, syphilis and gonorrhoea, and in discussions about sexual health. Overall, the audited preventive health records showed that there were several areas of STI care where improvement is needed:
- 68 per cent of clients had attended the PHC centres in the last six months, 49 per cent for acute care and only 8 per cent specifically for sexual health
- clients aged 20–24 and 25–29 years were more than three times more likely to be tested than clients in other age groups
- women received higher levels of testing for sexually transmitted infections compared with men (a 45 per cent greater chance of being tested)
- women having a Pap smear test were more than four times more likely to have STI testing and counselling than women attending for other types of care.20
Recent surveillance reports about STIs indicate that these findings about the quality of preventive care for sexual health are still relevant for focusing improvement efforts.21
The CQI research found that adherence to clinical guidelines for sexual health testing and counselling varied widely between PHC centres, ranging from 0 per cent to 100 per cent in some years or cycles. Overall, service delivery for sexual health testing and counselling services improved over time, from a median of 27 per cent in 2005/06 to 54 per cent in 2014 (see Figure 18.1). There were several factors accounting for the variation:
- whether or not adult health checks were provided by the PHC centre: individuals undergoing an adult health check were three times more likely to be tested for STIs
- whether or not the centre had participated in one to two CQI cycles compared with just conducting a baseline audit (see Figure 18.1b)
- whether or not there was policy support and infrastructure for CQI. There were higher levels of service delivery in the two jurisdictions that had regional CQI facilitator networks and statewide CQI planning and governance committees.22
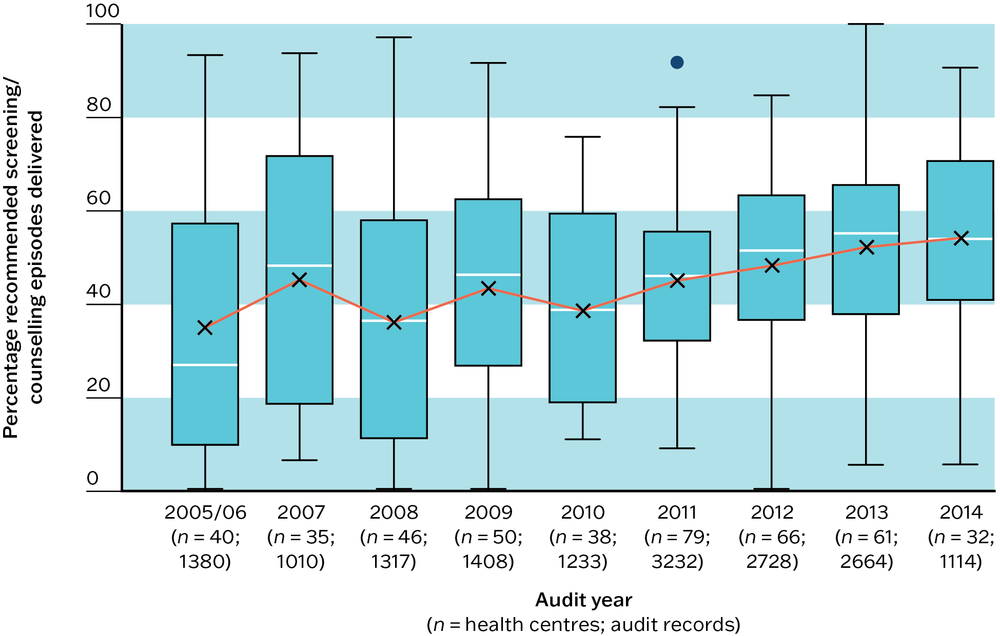
Figure 18.1a Sexual health–related service delivery over time (including nucleic acid amplification tests for gonorrhoea and chlamydia, syphilis screen and reproductive health discussion): mean percentage of STI testing and counselling delivered, by audit year. Source: Nattabi, Matthews et al. 2017.
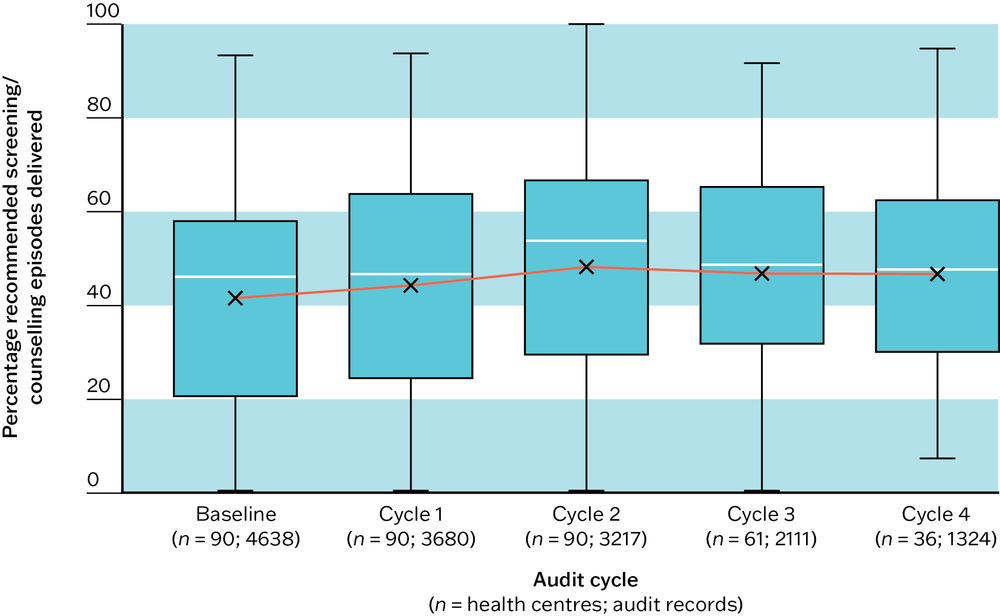
Figure 18.1b Sexual health–related service delivery over time (including nucleic acid amplification tests for gonorrhoea and chlamydia, syphilis screen and reproductive health discussion): mean percentage of STI testing and counselling delivered, by audit cycle. Source: Nattabi, Matthews et al. 2017.
In the context of a syphilis outbreak among Aboriginal and Torres Strait Islander peoples in Northern Australia, CQI data from 77 PHC services (2012–14) were analysed to examine associations between PHC health centre (or clinic) factors and syphilis-testing performance.23 The study provided insights to help PHC managers respond to the syphilis outbreak, as follows:
- neither accreditation status nor governance model were associated with syphilis-testing performance
- with respect to Systems Assessment Tool24 component scores, “Delivery system design” (which refers to the design of the clinic’s infrastructure, staffing profile, allocation of roles and responsibilities, client flow and care processes) was significantly associated with syphilis-testing performance in all clinics
- within “Delivery system design”, three items were significantly associated: “Continuity of care”, “Team structure and function” and “Care planning”
- “Information systems and design support” was also linked with syphilis-testing performance.25
The STRIVE trial
The “STIs in Remote communities, ImproVed and Enhanced primary care” (STRIVE) trial was a stepped wedge cluster-randomised trial with CQI as an intervention. STRIVE was the first large-scale investigation of clinical CQI strategies for the control of STIs in remote Aboriginal community settings. The trial was conducted over three years from 2010 in 67 remote communities in three Australian jurisdictions (Northern Territory, Queensland and Western Australia).26
STRIVE established evidence-based tools and processes to drive CQI and showed that a clinic-level sexual health CQI program supported by regional sexual health coordinators could improve care systems and STI testing rates. The trial found that simple but reproducible actions increased testing and retesting for STIs.
“Now that sexual health is integrated into the adult health check, through the men’s and women’s checks, that has been the single most [important change]. Putting in recalls for sexual health in the [client care information system] has actually improved it. Making sure that I’m auditing so that we know if somebody’s not being followed up. Then we ask the hard questions why and follow that through.” – sexual health coordinator A27
“There’s things like putting recalls on for test for reinfection, using the STI template which is embedded in [the electronic client information system] and things like that, as a prompt to help better sexual health delivery.” – sexual health coordinator B28
Context-specific CQI tools and audit reports helped teams to use data for improvement.
“I’ve done the stats, my system assessments tools … that’s a very powerful tool because the clinic [team] will sit back and go, ‘oh, wow’ … They’ll look at the spider graphs and they really get into that visual stuff to find out their strengths and weaknesses and how they can improve.” – sexual health coordinator C.29
Over the trial period, testing coverage improved by almost 40 per cent overall, and aspects of the CQI program became normalised in clinical practice. There was no change in prevalence of STIs over the three-year time frame. This was mainly because baseline testing was so low.30
Sexual health (STI/BBV) clinical audit tool
The above findings about quality of care for STI testing resulted from the use a preventive health audit tool. A sexual health audit tool31 was developed, piloted and refined by service providers in four Australian jurisdictions. Released by Menzies School of Health Research in 2014, the tool is intended to be used in conjunction with the Systems Assessment Tool and the preventive health and youth health audit tools (see Chapters 5, 11 and 14).
The purpose of the sexual health audit is to determine the management of a sexually transmissible infection (STI) or bloodborne virus (BBV) episode from the time the client first presents to the health centre for assessment of symptoms and diagnosis through to laboratory investigations, treatment and follow-up care.
Key messages for improving the delivery of STI care in PHC
The patterns of sexual healthcare delivery for STIs in Aboriginal and Torres Strait Islander PHC communities are likely to have similarities with care delivery in other settings internationally, and in populations that experience a high burden of STIs. This CQI research identifies priorities for improvement and offers messages for improving the delivery of sexual health care in PHC.
At the health centre and community level, these actions can be undertaken for improvement:
- integrate STI testing into routine care and community screening (for example, cervical screening, contraception and adult healthcare checks)
- set up clinical information systems to flag clients for follow-up treatment, and to recall clients for retesting
- increase STI testing efforts for groups with high incidence rates (for example, young people 15–19 years old) and groups with lower testing rates (for example, men); this may require tackling barriers to accessing sexual health care for these groups
- record the delivery of sexual health care accurately in client records to ensure effective screening and treatment for clients and their partners, and to provide data for CQI
- put STI notification systems in place and train staff to keep STI notifications up to date
- adapt CQI tools and reports as needed to support improvement in STI testing and care; CQI tools should be adaptable for responding to the local context, to a risk environment such as a syphilis outbreak, or to an update to clinical guidelines
- encourage ownership of, and management support for, CQI processes for sexual health care.
At the regional or area level, these activities can support improvement efforts:
- coordinate sexual health care and CQI support across communities and PHC centres
- encourage compliance with STI notifications and other high-level information systems for improving STI care
- promote CQI as a tool to identify and act on areas for improvement in sexual health services
- encourage local ownership of, and management support for, CQI processes for sexual health care (this is relevant at regional and local levels)
- invest in CQI infrastructure and support.
Improving STI care in Aboriginal and Torres Strait Islander PHC
Improving knowledge and awareness of STIs among communities and health professionals is essential for improving sexual health care and reducing the rate and consequences of STIs. While common STIs are easily detected and easily treated, a high proportion of STIs are asymptomatic. Therefore, diagnosis rates depend on testing that mainly occurs in PHC services.32 This requires PHC staff to be aware of the STI risk factors and the current guidelines on testing and treatment, and skilled in communicating with clients and providing culturally safe care. This in turn highlights the need for these elements:
- a stable workforce that includes Aboriginal and Torres Strait Islander practitioners
- training in cultural safety for non-Indigenous staff
- a team mix that enables culturally appropriate care (for example, male practitioners providing care for men)
- measures that ensure privacy and confidentiality, particularly in smaller communities (for example, family members may work in the health centre).33
Our findings showed that a high proportion of the variation in quality of care was explained by health centre factors rather than client factors, suggesting that structural and organisational developments are needed to provide high-quality sexual health care. In addition to the measure suggested above, organisational-level strategies such as multidisciplinary clinical teams, refined professional roles and structural changes (for example, changes in clinic hours, outreach services) could increase the capacity of PHC staff to provide high-quality care and ensure that STI prevention and management services are always available. Barriers such as workload pressures and competing work priorities should also be considered.34
A high proportion of the variation in quality of care was explained by health centre factors rather than client factors.
There have been a number of interventions to improve the quality of sexual health care for Aboriginal and Torres Strait Islander clients attending PHC services. In addition to the ABCD program (the source of our audit findings) and the STRIVE project they include, for example, the Sexual Health Quality Improvement program (SHIMMER) in New South Wales.35 Across these interventions, the use of CQI was shown to increase STI testing rates. Findings supported the integration of STI testing into general medical consultations and adult health checks, and health promotion programs that encourage people to present more frequently to PHC services and request STI testing.36
Community health promotion for STIs should include knowledge of risk factors and the important role of condoms, the need for timely testing and treatment, and the potential long-term consequences of STIs. Client and community approaches must be culturally safe, and gender and age appropriate. This may involve, for example, peer-based approaches and outreach services in places where young people meet. Resources should present an Aboriginal and Torres Strait Islander perspective and any approach used should aim to counter shame and STI-related stigma. Resources for PHC staff doing STI work with different groups are available through the Australian Indigenous HealthInfoNet.37
Approaches must be culturally safe, and gender and age appropriate.
CQI research findings about the positive association between cervical screening test and STI testing in female clients highlights the value of integrating STI testing and counselling with other aspects of care. Cervical screening among Aboriginal and Torres Strait Islander women is important given that the incidence of and mortality from cervical cancer is higher compared to non-Aboriginal women,38 but also because cervical screening provides an opportunity for STI testing.39 From 2017, CQI activities have needed to monitor the possible effect of changes in Australia’s cervical cancer screening program on STI testing rates among women, as the introduction of a primary human papillomavirus (HPV) test every five years has replaced the requirement for Pap tests every two years.40
A national surveillance and research network for STIs and bloodborne viruses in Aboriginal and Torres Strait Islander PHC services (ATLAS) has been established to augment the Australian National Notifiable Diseases Surveillance System. The ATLAS network analyses de-identified client records to help improve understanding of patterns of infection, testing and care, risk and protective behaviours, and returns data to participating health services every six months for use in CQI processes.41
References
Australian Indigenous HealthInfoNet (n.d.). Edith Cowan University. https://healthinfonet.ecu.edu.au/.
Bowden, F., M. Currie, H. Toyne, C. McGuiness, L. Lim, J. Butler et al. (2008). Screening for Chlamydia trachomatis at the time of routine Pap smear in general practice: a cluster randomised controlled trial. Medical Journal of Australia 188(2): 76–80. DOI: 10.5694/j.1326-5377.2008.tb01526.x.
Bradley, C., B. Hengel, K. Crawford, S. Elliott, B. Donovan, D. Mak et al. (2020). Establishment of a sentinel surveillance network for sexually transmissible infections and blood borne viruses in Aboriginal primary care services across Australia: the ATLAS project. BMC Health Services Research 20(1): 769. DOI: 10.1186/s12913-020-05388-y.
Communicable Diseases Network of Australia (2021). Multijurisdictional syphilis outbreak surveillance report: February 2021. Canberra: Department of Health.
Condon, J., X. Zhang, P. Baade, K. Griffiths, J. Cunningham, D. Roder et al. (2014). Cancer survival for Aboriginal and Torres Strait Islander Australians: a national study of survival rates and excess mortality. Population Health Metrics 12(1): 1. DOI: 10.1186/1478-7954-12-1.
de Sanjosé, S., M. Diaz, X. Castellsagué, G. Clifford, L. Bruni, N. Muñoz et al. (2007). Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: a meta-analysis. Lancet Infectious Diseases 7(7): 453–9. DOI: 10.1016/S1473-3099(07)70158-5.
Graham, S., R. Guy, H. Wand, J. Kaldor, B. Donovan, J. Knox et al. (2015). A sexual health quality improvement program (SHIMMER) triples chlamydia and gonorrhoea testing rates among young people attending Aboriginal primary health care services in Australia. BMC Infectious Diseases 15(1): 370. DOI: 10.1186/s12879-015-1107-5.
Gunaratnam, P., G. Schierhout, J. Brands, L. Maher, R. Bailie, J. Ward et al. (2019). Qualitative perspectives on the sustainability of sexual health continuous quality improvement in clinics serving remote Aboriginal communities in Australia. BMJ Open 9(e026679). DOI: 10.1136/bmjopen-2018-026679.
Hengel, B., S. Bell, L. Garton, J. Ward, A. Rumbold, D. Taylor-Thomson et al. (2018). Perspectives of primary health care staff on the implementation of a sexual health quality improvement program: a qualitative study in remote Aboriginal communities in Australia. BMC Health Services Research 18(1): 230. DOI: 10.1186/s12913-018-3024-y.
Hengel, B., H. Wand, J. Ward, A. Rumbold, L. Garton, D. Taylor-Thomson et al. (2017). Patient, staffing and health centre factors associated with annual testing for sexually transmissible infections in remote primary health centres. Sexual Health 14(3): 274–81. DOI: 10.1071/SH16123.
Menzies School of Health Research and One21seventy (2014). Sexual health (STI/BBV) clinical audit tool. Brisbane: Menzies School of Health Research. https://www.menzies.edu.au/page/Resources/.
Menzies School of Health Research and One21seventy (2012). Systems assessment tool – all client groups. Darwin: Menzies School of Health Research.
National Aboriginal Community Controlled Health Organisation and Royal Australian College of General Practitioners (2024). National guide to a preventative health assessment for Aboriginal and Torres Strait Islander people, 4th edn. Melbourne: RACGP.
Nattabi, B., S. Girgis, V. Matthews, R. Bailie and J. Ward (2018). Clinic predictors of better syphilis testing in Aboriginal primary health care: a promising opportunity for primary health care service managers. Australian Journal of Primary Health 24(4): 350–8. DOI: 10.1071/PY17148.
Nattabi, B., V. Matthews, J. Bailie, A. Rumbold, D. Scrimgeour, J. Ward et al. (2017). Wide variation in sexually transmitted infection testing and counselling at Aboriginal primary health care centres in Australia: analysis of longitudinal continuous quality improvement data. BMC Infectious Diseases 17(1). DOI: 10.1186/s12879-017-2241-z.
Northern Territory Department of Health (2019). NT Guidelines for the management of sexually transmitted infections in the primary health care setting, 5th edn. Darwin: Northern Territory Government.
Remote Primary Health Care Manuals (2022). CARPA standard treatment manual for remote and rural practice. Alice Springs, NT: Flinders University. https://remotephcmanuals.com.au/document/35499.html.
Rowley, J., S. Vander Hoorn, E. Korenromp, N. Low, M. Unemo, L. Abu-Raddad et al. (2019). Chlamydia, gonorrhoea, trichomoniasis and syphilis: global prevalence and incidence estimates, 2016. Bulletin of the World Health Organization 97(8): 548–62P. DOI: 10.2471/BLT.18.228486.
Silver, B., R. Guy, H. Wand, J. Ward, A. Rumbold, C. Fairley et al. (2015). Incidence of curable sexually transmissible infections among adolescents and young adults in remote Australian Aboriginal communities: analysis of longitudinal clinical service data. Sexually Transmitted Infections 91(2): 135–41. DOI: 10.1136/sextrans-2014-051617.
Temmerman, M., R. Khosla and L. Say (2014). Sexual and reproductive health and rights: a global development, health, and human rights priority. Lancet 384(9941): e30–e31. DOI: 10.1016/S0140-6736(14)61190-9.
The Kirby Institute (2022). Blood borne viral and sexually transmissible infections in Aboriginal and/or Torres Strait Islander peoples 2021. Sydney: University of New South Wales.
The Kirby Institute (2020). National update on HIV, viral hepatitis and sexually transmissible infections in Australia: 2009–2018. Sydney: University of New South Wales.
The Kirby Institute (2018). Bloodborne viral and sexually transmissible infections in Aboriginal and Torres Strait Islander people: annual surveillance report 2018. Sydney: University of New South Wales.
Ward, H. and M. Rönn (2010). Contribution of sexually transmitted infections to the sexual transmission of HIV. Current Opinion in HIV & AIDS 5(4): 305–10. DOI: 10.1097/COH.0b013e32833a8844.
Ward, J., L. Crooks and D. Russell (2016). High level summit on rising HIV, sexually transmissible infections (STI) and viral hepatitis in Aboriginal and Torres Strait Islander communities – final report 2016. Adelaide: South Australian Health and Medical Research Institute.
Ward, J., R. Guy, A. Rumbold, S. McGregor, H. Wand, H. McManus et al. (2019). Strategies to improve control of sexually transmissible infections in remote Australian Aboriginal communities: a stepped-wedge, cluster-randomised trial. Lancet Global Health 7(11): e1553–e63. DOI: 10.1016/S2214-109X(19)30411-5.
Ward, J., B. Hengel, D. Ah Chee, O. Havnen and J. Boffa (2020). Setting the record straight: sexually transmissible infections and sexual abuse in Aboriginal and Torres Strait Islander communities. Medical Journal of Australia 212(5): 205–7.e1. DOI: 10.5694/mja2.50492.
Ward, J., S. McGregor, R. Guy, A. Rumbold, L. Garton, B. Silver et al. (2013). STI in remote communities: improved and enhanced primary health care (STRIVE) study protocol: a cluster randomised controlled trial comparing “usual practice” STI care to enhanced care in remote primary health care services in Australia. BMC Infectious Diseases 13(1): 425. DOI: 10.1186/1471-2334-13-425.
World Health Organization (2024, 21 May). Sexually transmitted infections (STIs): Key facts. https://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis).
World Health Organization (2018). Report on global sexually transmitted infection surveillance, 2018. Geneva, Switzerland: WHO.
1 Temmerman, Khosla and Say 2014.
2 Rowley, Vander Hoorn et al. 2019; World Health Organization 2018.
3 de Sanjosé, Diaz et al. 2007; World Health Organization 2023.
4 World Health Organization 2023.
5 Ward and Rönn 2010.
6 World Health Organization 2024.
7 World Health Organization 2024.
8 World Health Organization 2024.
9 Ward, Crooks and Russell 2016.
10 The Kirby Institute 2020.
11 Silver, Guy et al. 2015; The Kirby Institute 2022.
12 Remote Primary Health Care Manuals 2022.
13 Nattabi, Matthews et al. 2017; The Kirby Institute 2018.
14 Communicable Diseases Network of Australia 2021.
15 Ward, Hengel et al. 2020.
16 Hengel, Wand et al. 2017.
17 National Aboriginal Community Controlled Health Organisation and Royal Australian College 2024.
18 Northern Territory Department of Health 2019; Remote Primary Health Care Manuals 2022.
19 Remote Primary Health Care Manuals 2022.
20 Nattabi, Matthews et al. 2017.
21 The Kirby Institute 2020, 2022.
22 Nattabi, Matthews et al. 2017.
23 Nattabi, Girgis et al. 2018.
24 Menzies School of Health Research and One21seventy 2012.
25 Nattabi, Girgis et al. 2018.
26 Ward, McGregor et al. 2013.
27 Gunaratnam, Schierhout et al. 2019, 3.
28 Gunaratnam, Schierhout et al. 2019, 4.
29 Gunaratnam, Schierhout et al. 2019, 3.
30 Hengel, Bell et al. 2018; Ward, Guy et al. 2019.
31 Menzies School of Health Research and One21 seventy 2014. Download from https://www.menzies.edu.au/page/Resources/.
32 Ward, Hengel et al. 2020.
33 Nattabi, Matthews et al. 2017.
34 Nattabi, Matthews et al. 2017.
35 Graham, Guy et al. 2015.
36 Graham, Guy et al. 2015.
37 Australian Indigenous HealthInfoNet. n.d. https://healthinfonet.ecu.edu.au/.
38 Condon, Zhang et al. 2014.
39 Bowden, Currie et al. 2008.
40 Nattabi, Matthews et al. 2017.
41 Bradley, Hengel et al. 2020.