17
Improving care for acute rheumatic fever and rheumatic heart disease
Acute rheumatic fever and rheumatic heart disease
Acute rheumatic fever (ARF) and rheumatic heart disease (RHD) are preventable conditions associated globally with poverty, crowded housing and poor living conditions.1 ARF is caused by an autoimmune response to infection with streptococcal bacteria that are often found in skin sores and sore throats. It can cause inflammation of the heart, often resulting in permanent damage to the heart valves, usually because of recurrences. RHD is the long-term condition caused by permanent damage to one or more of the heart valves following ARF. The heart valve or valves may become narrowed, obstructing the flow of blood or failing to close properly or both. This can lead to heart failure and the need for cardiac surgery, or stroke, and often leads to premature death.
RHD is a serious public health problem in low- and middle-income countries and among marginalised communities in high-income countries, including Indigenous populations. In 2018, some 30 million people were thought to be affected by RHD globally. RHD disproportionately affects girls and women; where endemic, it is a significant cause of poor maternal health outcomes.2
People affected by ARF and RHD need to have ongoing active engagement with the healthcare system for many years. This means the role of PHC practitioners in the prevention, screening, diagnosis, management and referral for ARF and RHD is crucial. Where RHD control programs are in place, practitioners may also be responsible for ARF and RHD notifications.
ARF/RHD and recommended care for Aboriginal and Torres Strait Islander peoples
RHD data show one of the greatest inequities in disease rates between Indigenous and non-Indigenous Australians, with rates of ARF and RHD in some Aboriginal and Torres Strait Islander communities among the highest documented globally.3 A recent study found the age standardised ARF incidence (for people younger than 45 years) was 124 times higher and RHD prevalence (for those younger than 55 years) was 61 times higher among Aboriginal and Torres Strait Islander people compared with non-Indigenous Australians, with substantially higher rates in northern, remote Australian regions.4 The number and rate of ARF notifications increased between 2016 and 2022, and almost half (46 per cent) of diagnoses were children aged 5 to 14 years.5 These data provide compelling evidence of the need to improve living environments, disease awareness and management.
Recommended prevention and treatment
ARF can be prevented through improving living conditions and prompt antibiotic treatment for streptococcal infections. The recommended treatment of ARF and RHD is as follows:
- People diagnosed with ARF or RHD are assigned a RHD priority classification (1–4) based on disease severity. The classification guides recommended disease management.
- People who have had ARF need benzathine benzylpenicillin G injections every 4 weeks for a minimum of 5 years after the last episode or until age 21 (whichever occurs later), to avoid recurrences and prevent RHD progression.
- Continued secondary prevention (prophylaxis) to age 35 is recommended for moderate RHD and to age 40 or lifelong for severe cases, especially in people requiring heart valve surgery.
- Administration of more than 80 per cent of a client’s prescribed benzathine benzylpenicillin G injections substantially reduces the risk of ARF recurrence, thereby reducing the risk of early death from RHD.6
Comprehensive PHC advice, resources and clinical guidelines are available on the RHD Australia website.7 The World Heart Federation guidelines for diagnosis of RHD were updated in 2023.8
Findings: quality of acute rheumatic fever and rheumatic heart disease prevention and care
The data presented below on the quality of ARF/RHD care come mainly from six research papers and reports from the ABCD research program. The studies collectively analysed 5,209 client records from PHC centres, which were audited between 2008 and 2014. Most PHC centres were in geographically remote locations in northern Australia. Stakeholders participated in data interpretation to identify priority evidence-to-practice gaps and factors influencing improvement. Information on the application of CQI for ARF and RHD care and on clinical audit processes and audit findings are reported elsewhere.9 We provide a brief overview of key findings below.
Across the studies, patterns and priorities for improvement could be identified.
- Secondary prevention: the majority of clients did not receive levels of secondary prevention known to offer best protection from ARF recurrence. From 2008 to 2014, the proportion of clients receiving more than 80 per cent of their scheduled benzathine benzylpenicillin G injections did not improve. PHC centres with high scores for “systematic processes of follow-up” were significantly better at administering the injections at recommended levels.10
- Management plans and education: some 70 to 80 per cent of clients had a disease management plan in place. However, clients’ RHD priority classification, the provision of education about secondary prevention and follow-up action plans for clients with low rates of benzathine benzylpenicillin G injections were not consistently recorded. Only 12 per cent of clients with poor adherence to benzathine benzylpenicillin G injections had action plans. Provision of health education appeared low, even among people younger than 25 years, for whom secondary prevention has the most potential to improve outcomes. These findings indicate a need for better systems to translate secondary prevention guidelines into quality care.11
- Overall delivery of ARF/RHD prevention and care: there were improvements in overall service delivery. PHC centre mean delivery of care went from 42 per cent in 2008 to 66 per cent in 2012, but the upward trend was not sustained. There was large variation in service delivery between health centres, and this variation did not reduce over time, despite sustained CQI activities12 (see Figure 17.1)
- Client age: children younger than 15 years received a higher level of ARF/RHD care compared with adults in all age groups. Most clients younger than 25 years (88.5 per cent) had RHD (as opposed to ARF), and 20 per cent had RHD without a documented history of ARF, indicating earlier missed diagnosis or asymptomatic cases of ARF. Many older people were found to have been prescribed penicillin, in contradiction to guidelines.13
Figure 17.1 shows the trend over the audit years for service delivery for up to nine best-practice indicators for rheumatic heart disease care (present in the rheumatic heart disease audit tool): a record of the rheumatic heart disease classification in the health summary; a record of current and of complete acute rheumatic fever and rheumatic heart disease management plans; a record of planned frequency of injections (if the client had been prescribed injections); whether 80 per cent or more of injections had been received (if the client had been prescribed regular injections and there was a record of planned frequency); a record of active recall if less than 80 per cent of injections had been received; timely doctor and specialist review, and echocardiogram (according to recommended schedule based on the rheumatic heart disease classification); and record of client education (provided within the last 12 months).
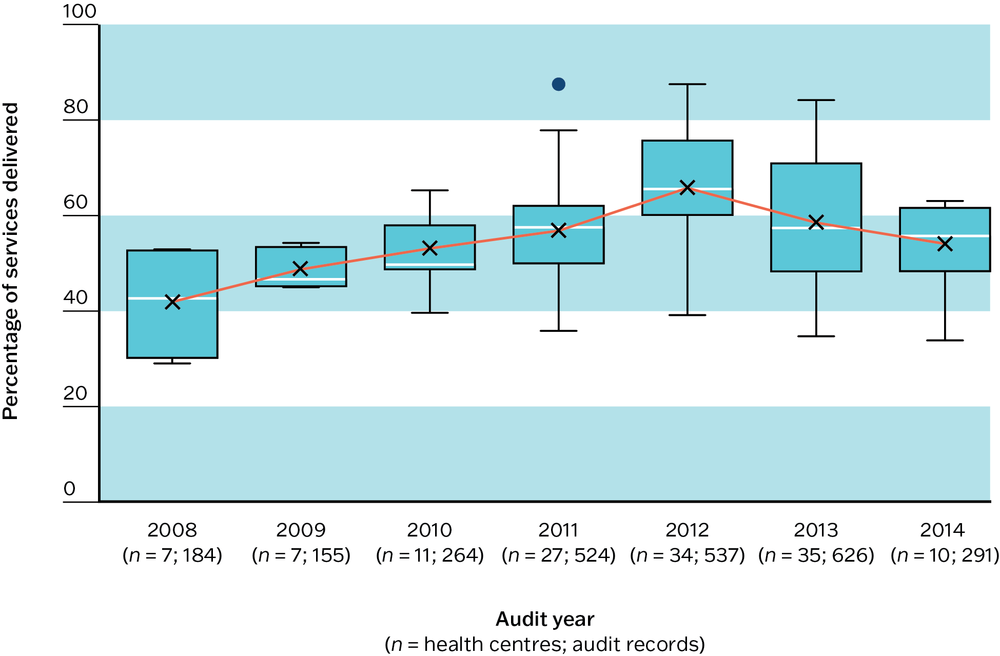
Figure 17.1 Trends in overall RHD care. Source: J. Bailie, Matthews et al. 2016.
Key messages for improving acute rheumatic fever and rheumatic heart disease care
This CQI research identifies clear priorities and strategies for improving PHC for ARF/RHD, and includes stakeholder interpretation of CQI data. Patterns of ARF/RHD care delivery in Aboriginal and Torres Strait Islander PHC communities are likely to reflect, at least to some extent, care delivery in international settings where ARF/RHD persist.
These are the messages for action:
- Educate PHC teams on the importance of the injection schedule to manage ARF/RHD, on best-practice guidelines and on use of client information systems. Clarify roles for RHD care, including RHD-related responsibilities for selected nursing staff.
- Aim to provide at least 80 per cent of planned benzathine benzylpenicillin G injections. This requires good follow-up systems and flexible options for delivery, such as outreach services. Pain management for reducing discomfort from injections should be considered.
- Accurately record ARF diagnosis, care and management plans in client records.
- Notify all cases as required by regional and national guidelines.
- Develop transition care to support children with ARF and RHD through adolescence, and develop strategies to engage young adults who are affected.
- Provide culturally appropriate client, family and community education to improve health literacy.
- Increase the focus on primary prevention (not included in audits), such as facilities for washing, wastewater and rubbish removal, reducing household crowding, improving nutrition and dust control, and strengthening school-based education and prevention measures.
- Use CQI to sustain and strengthen health promotion strategies and clinical care.
Improving ARF/RHD care in Aboriginal and Torres Strait Islander PHC
Our studies show that systems are inadequate to translate secondary prevention guidelines into quality care. In addition, the low number of clients with a recorded RHD priority classification (30 per cent of 1,081 audits in one study) suggests that this classification is rarely used to guide management.14
ARF and RHD occur mostly amongst people living in remote locations, where poor housing infrastructure and crowded living contribute to the transmission of infections.15 PHC centres are typically understaffed and have a high turnover of staff. A workforce study in the Northern Territory found that only 20 per cent of nurses and Aboriginal healthcare providers remained working at surveyed remote clinics 12 months after commencing. Half left within four months.16 Embedding change in care delivery systems, providing staff training and maintaining knowledge in ARF/RHD management and use of information systems is very challenging but even more critical under these circumstances.17 The trial of a multi-strategy RHD intervention in 10 remote communities found that long-term PHC system–strengthening strategies, with more linkages between PHC teams and communities, are essential to improve adherence to secondary prevention.18
Long-term PHC system–strengthening strategies, with more linkages between PHC teams and communities, are essential to improve adherence to secondary prevention.
Early prevention should include comprehensive skin and throat programs in high-risk communities.19 Transitioning children with ARF safely to adulthood without rheumatic heart damage requires tailored care. Engaging and valuing local navigators to address language and cultural barriers has been recommended as a sustainable alternative to transition coordinators in mainstream programs.20
Cultural competence of healthcare teams, including appropriate communication styles that empower clients and their families with knowledge about their health conditions and treatment,21 is critically important when tackling diseases of disparity such as RHD. Clinicians’ competency in communicating influences health outcomes for Aboriginal and Torres Strait Islander people,22 and multiple Australian studies of CQI in ARF and RHD care have highlighted the importance of communicating with clients in local languages and using culturally appropriate educational resources for improving RHD prevention and management.23 Culturally competent and well-prepared PHC teams, strong community engagement and Aboriginal and Torres Strait Islander leadership are key to improvement.24
References
ARF and RHD Guidelines (n.d.). Clinical guidelines. https://www.rhdaustralia.org.au/.
Australian Institute of Health and Welfare (2022). Acute rheumatic fever and rheumatic heart disease in Australia 2016–2020. Cat. no. CVD 95. Canberra: AIHW, Australian Government.
Bailie, J., V. Matthews, A. Laycock and R. Bailie. (2016). Aboriginal and Torres Strait Islander acute rheumatic fever and rheumatic heart disease care: final report. ESP Project. Brisbane: Menzies School of Health Research.
Coffey, P., A. Ralph and V. Krause (2018). The role of social determinants of health in the risk and prevention of group A streptococcal infection, acute rheumatic fever and rheumatic heart disease: a systematic review. PLOS Neglected Tropical Diseases 12(6): e0006577–e77. DOI: 10.1371/journal.pntd.0006577.
Haynes, E., M. Marawili, B. Marika, A. Mitchell, J. Phillips, D. Bessarab et al. (2019). Community-based participatory action research on rheumatic heart disease in an Australian Aboriginal homeland: evaluation of the “On track watch” project. Evaluation and Program Planning 74: 38–53. DOI: 10.1016/j.evalprogplan.2019.02.010.
Katzenellenbogen, J., D. Bond-Smith, A. Ralph, M. Wilmot, J. Marsh, R. Bailie et al. (2020a). Priorities for improved management of acute rheumatic fever and rheumatic heart disease: analysis of cross-sectional continuous quality improvement data in Aboriginal primary health care centres in Australia. Australian Health Review 44(2): 212–21. DOI: 10.1071/AH19132.
Katzenellenbogen, J., D. Bond-Smith, R. Seth, K. Dempsey, J. Cannon, I. Stacey et al. (2020b). Contemporary incidence and prevalence of rheumatic fever and rheumatic heart disease in Australia using linked data: the case for policy change. Journal of the American Heart Association 9(19): e016851–e51. DOI: 10.1161/JAHA.120.016851.
McDonald, E., R. Bailie, J. Grace and D. Brewster (2009). A case study of physical and social barriers to hygiene and child growth in remote Australian Aboriginal communities. BMC Public Health 9(1): 346. DOI: 10.1186/1471-2458-9-346.
Mitchell, A., S. Belton, V. Johnston, W. Gondarra and A. Ralph (2019). “That heart sickness”: young Aboriginal people’s understanding of rheumatic fever. Medical Anthropology 38(1): 1–14. DOI: 10.1080/ 01459740.2018.1482549.
Mitchell, A., S. Belton, V. Johnston and A. Ralph (2018). Transition to adult care for Aboriginal children with rheumatic fever: a review informed by a focussed ethnography in northern Australia. Australian Journal of Primary Health 24(1): 9–13. DOI: 10.1071/PY17069.
Quinn, E., S. Girgis, J. Van Buskirk, V. Matthews and J. Ward (2019). Clinic factors associated with better delivery of secondary prophylaxis in acute rheumatic fever management. Australian Journal of General Practice 48(12): 859–65. DOI: 10.31128/ajgp-07-19-4987.
Ralph, A., J. de Dassel, A. Kirby, C. Read, A. Mitchell, G. Maguire et al. (2018). Improving delivery of secondary prophylaxis for rheumatic heart disease in a high-burden setting: outcome of a stepped-wedge, community, randomized trial. Journal of the American Heart Association 7(14): e009308. DOI: 10.1161/jaha.118.009308.
Ralph, A., M. Fittock, R. Schultz, D. Thompson, M. Dowden, T. Clemens et al. (2013). Improvement in rheumatic fever and rheumatic heart disease management and prevention using a health centre-based continuous quality improvement approach. BMC Health Services Research 13: 525. DOI: 10.1186/1472-6963-13-525.
Read, C., A. Mitchell, J. de Dassel, C. Scrine, D. Hendrickx, R. Bailie et al. (2018). Qualitative evaluation of a complex intervention to improve rheumatic heart disease secondary prophylaxis. Journal of the American Heart Association 7(14): e009376. DOI: 10.1161/JAHA.118.009376.
RHDAustralia (ARF/RHD writing group) (2020). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease, 3rd edn. Darwin: Menzies School of Health Research.
Russell, D., Y. Zhao, S. Guthridge, M. Ramjan, M. Jones, J.S. Humphreys et al. (2017). Patterns of resident health workforce turnover and retention in remote communities of the Northern Territory of Australia, 2013–2015. Human Resources for Health 15(1): 52. DOI: 10.1186/s12960-017-0229-9.
Rwebembera, J., J. Marangou, J. Mwita, A. Mocumbi, C. Mota, E. Okello et al. (2024). 2023 World Heart Federation guidelines for the echocardiographic diagnosis of rheumatic heart disease. Nature Reviews Cardiology 21(4): 250–63. DOI: 10.1038/s41569-023-00940-9.
The Kids Research Institute Australia (2024). RHD endgame strategy. https://endrhd.telethonkids.org.au/RHD-Endgame-Strategy/.
World Health Organization (2018). Seventy-first World Health Assembly, rheumatic fever and rheumatic heart disease: report by the Director-General. Geneva, Switzerland: World Health Organization.
Wyber R., K. Noonan, C. Halkon, S. Enkel, A. Ralph, A. Bowen et al. (2020). RHD endgame strategy: the blueprint to eliminate rheumatic heart disease in Australia by 2031. END RHD Centre of Research Excellence. Perth: Telethon Kids Institute. https://endrhd.telethonkids.org.au/RHD-Endgame-Strategy/.
1 Coffey, Ralph and Krause 2018.
2 World Health Organization 2018.
3 Ralph, de Dassel et al. 2018.
4 Katzenellenbogen, Bond-Smith et al. 2020b.
5 Australian Institute of Health and Welfare 2022.
6 RHDAustralia (ARF/RHD writing group) 2020.
7 Download guidelines from ARF and RHD Guidelines n.d.
8 Rwebembera, Marangou et al. 2024.
9 J. Bailie, Matthews et al. 2016; Katzenellenbogen, Bond-Smith et al. 2020a; Quinn, Girgis et al. 2019; Ralph, Fittock et al. 2013.
10 Quinn, Girgis et al. 2019.
11 J. Bailie, Matthews et al. 2016; Katzenellenbogen, Bond-Smith et al. 2020a; Quinn, Girgis et al. 2019.
12 J. Bailie, Matthews et al. 2016; Ralph, Fittock et al. 2013.
13 Katzenellenbogen, Bond-Smith et al. 2020a.
14 Katzenellenbogen, Bond-Smith et al. 2020a.
15 McDonald, R. Bailie et al. 2009.
16 Russell, Zhao et al. 2017.
17 Read, Mitchell et al. 2018.
18 Ralph, de Dassel et al. 2018.
19 Wyber, Noonan et al. 2020.
20 Mitchell, Belton et al. 2018.
21 Mitchell, Belton et al. 2019.
22 Mitchell, Belton et al. 2019.
23 J. Bailie, Matthews et al. 2016; Haynes, Marawili et al. 2019; Katzenellenbogen, Bond-Smith
et al. 2020a; Mitchell, Belton et al. 2019; Ralph, de Dassel et al. 2018; Read, Mitchell et al. 2018.
24 Wyber, Noonan et al. 2020, Haynes, Marawili et al. 2019, download resources from The Kids Research Institute Australia 2024.