16
Improving cardiovascular health care
Cardiovascular health care and disease
Cardiovascular diseases are a group of disorders of the heart and blood vessels. They include coronary heart disease, cerebrovascular disease, heart failure and rheumatic heart disease (see Chapter 17). Cardiovascular disease (CVD) is largely caused by the combined effect of risk factors that can be modified. Behavioural risk factors, such as smoking, unhealthy diet, physical inactivity and harmful use of alcohol may show up in individuals as raised blood pressure, raised blood glucose, raised blood lipids, and overweight and obesity.1 Having type 2 diabetes and associated kidney disease can also increase cardiovascular diseases risk,2 as can overcrowding and poor living conditions that contribute to chronic inflammation (see Chapters 10 and 17), and periodontal disease. The incidence of heart attack, stroke and CVD death rates increase with increasing socio-economic disadvantage.3 Poor social and emotional wellbeing is linked with higher risk of a CVD event4 and difficulty making changes to reduce health risks.5 In 2018–19, for example, two-thirds of Australian Aboriginal and Torres Strait Islander adults reported low or moderate levels of psychological distress and one-third experienced high levels.6 Most risk factors for cardiovascular disease can be measured in PHC services to show whether clients have an increased risk of heart attack, stroke, heart failure and other complications.7 Most are amenable to health service interventions.
CVDs are the leading cause of death globally. More than 80 per cent of the deaths are due to heart attacks and strokes, and one-third occur prematurely in people younger than 70 years of age. At least three-quarters of the world’s deaths from CVDs occur in low- and middle-income countries, where people have poor access to PHC and therefore less access to screening and disease management.8
PHC practitioners have an important role in the prevention and management of CVD through public health advocacy, and by providing timely access to CVD risk assessment and supporting behaviour modification and treatment to reduce the risk of a cardiovascular event. This is particularly important for clients with existing chronic conditions such as diabetes, chronic kidney disease and chronic inflammation. A holistic whole-of-lifespan approach is important to help people to reduce their risk through healthy eating, regular exercise, minimal use of alcohol and not smoking tobacco, and to monitor and address other risk factors, such as poor social and emotional wellbeing and depression. Public health policies that make healthy choices easy and affordable are essential for motivating people to adopt and sustain healthy behaviours. Broader policy measures are needed to improve living conditions and reduce poverty and healthcare inequity.
Cardiovascular health and Aboriginal and Torres Strait Islander peoples
Preventable heart-related conditions, such as coronary heart disease, heart failure and rheumatic heart disease contribute substantially to poor health and premature death among Aboriginal and Torres Strait Islander peoples, and are a leading cause of preventable illness and death.9 Large improvements in cardiovascular health have been made in the last two decades, but challenges remain. Since 1998 the mortality rate due to cardiac conditions has halved for Aboriginal and Torres Strait Islander peoples and the delivery of cardiac-related diagnostic services has increased, but those with suspected or confirmed cardiac disease are still less likely to be reviewed by a specialist than non-Indigenous Australians.10 It is encouraging that the proportion of Aboriginal and Torres Strait Islander peoples accessing Medicare-funded health assessments has increased from 3 per cent in 2004–05 to 29 per cent in 2019–20.11 Adult health assessments present opportunities to assess cardiovascular disease risk and provide appropriate care.
Emerging evidence shows that high cardiovascular disease risk starts earlier in Aboriginal and Torres Strait Islander peoples compared with non-Indigenous Australians.12 An estimated 75 per cent of adults younger than 35 years have one or more risk factors for CVD13 and almost 5 per cent of people aged 25–34 years are at high risk of a cardiovascular event in the next five years, with most under-treated.14 A study in the Northern Territory found that 30 per cent of Aboriginal and Torres Strait Islander adults with moderate or high risk were younger than 35 years.15
Findings: quality of cardiovascular health care
Cardiovascular preventive health care
Australian and international guidelines for best practice recommend assessing CVD risk in PHC.16 Risk assessment is based on the combined effects of multiple risk factors and can identify people who do not have symptoms but are at high risk of cardiovascular disease. The Framingham Risk Equation is widely used for predicting risk of a cardiovascular event over the next five years for people who do not have existing cardiovascular disease or are not already known to be at increased risk. The Framingham Equation is now known to overestimate risk in the general Australia population, and was replaced by the Australian CVD Risk Calculator in 2023. Guidelines recommend the following:
- a CVD risk assessment for all adults aged 45 to 7917
- for people with diabetes without known CVD, risk should be assessed from ages 35 to 79 years
- people younger than 30 who meet the clinically determined high risk criteria, people with moderate to severe chronic kidney disease who have high albumin levels, and people with a family history of raised cholesterol levels should be assessed as high risk
- reassessment at intervals according to the level of risk identified, or new or worsening risk factors.18
There are additional guidelines for Aboriginal and Torres Strait Islander peoples:
- screening for risk factors from the ages of 18 to 29
- people aged 18–29 years with any of the conditions listed for the general population should be considered at high risk
- annual or opportunistic risk assessment from age 30 years at the latest
- screening and assessment as part of an annual health check, opportunistically or at least every two years, with review according to the level of risk identified.19
An assessment of a person’s cardiovascular risk takes into account their age and sex, smoking status, blood pressure, serum lipids, diabetes status, CVD medicines, socio-economic situation, and history of atrial fibrillation. For people with diabetes, the indicators to be assessed include blood glucose levels, time since diagnosis of diabetes, urine for albumin and protein levels, kidney function, body mass index, and insulin use. Further factors considered when classifying the risk of cardiovascular disease are the coronary artery calcium score, nutrition and physical activity, alcohol use, mental health, social history including ethnicity and community CVD prevalence, and family history of premature cardiovascular disease.20
People already known to be at increased risk for cardiovascular disease (for example, due to type 2 diabetes, moderate to severe chronic kidney disease, markedly raised cholesterol levels or very high blood pressure) should have their conditions managed according to the relevant clinical guidelines.
Study 1: Healthy adults without chronic conditions
A cross-sectional analysis of clinical records for 2,052 people at 97 health centres (2012–2014) was carried out to investigate delivery of CVD risk assessments in Aboriginal and Torres Strait Islander adults. Clients were older than 20 years and had no recorded chronic disease diagnosis.
The study found wide variation in the delivery of CVD risk assessment between different Australian jurisdictions and between PHC services. While some services provided excellent levels of assessments, others provided low levels.21 Overall, audited records showed these results:
- approximately 23 per cent of eligible clients (n = 478) had a documented CVD risk assessment
- even in the jurisdiction where most CVD risk assessments were recorded, there was wide variation between health services in the proportion of clients with a documented assessment (median 38 per cent; range 0–86 per cent)
- 11 per cent of clients (n = 53) who received an assessment were found with moderate or high risk; almost one-third of these clients were younger than 35 years of age
- health service factors accounted for 48 per cent of the variation in delivery of risk assessments; services with integrated clinical decision support systems that enable automated assessment of risk from information in clients electronic health records were more likely to document CVD risk assessments
- documentation of follow-up varied with respect to the targeted risk factor; fewer than 30 per cent of people with abnormal blood lipid or glucose levels had follow-up management plans recorded.22
Study 2: Teenagers and young adults
Another CQI study focused on Aboriginal and Torres Strait Islander people aged 15–34, examining 1,986 client records from 93 PHC services in remote, rural and urban locations. Despite the young age of the survey population, those who received assessments were commonly found to have important CVD risk factors that could be modified.23
- Acute care was the main reason for attendance, rather than a preventive healthcare assessment.
- 85 per cent of eligible clients (n = 1,686) had a record of blood pressure, 63 per cent
(n = 1,244) had blood glucose recorded, 37 per cent (n = 743) had an assessment of body mass index, and 31 per cent (n = 625) had lipids recorded. Smoking status was recorded for 52 per cent of clients (n = 1,033) (see Figure 16.1). - Clients aged 25 to 34 years were much more likely to be assessed for risk factors than those aged 15 to 24 years, except for body mass index measurement.
- Women were more likely to have a record of their blood pressure, blood glucose level and smoking status recorded than men. More women than men were overweight or obese, and men were more likely to have high blood pressure.
- The presence of risk factors was high in those who had a record of assessment, with the exception of blood pressure (7 per cent of clients) (see Figure 16.1).
- Among those clients with abnormal findings, documented follow-up was infrequent except for current smokers (65 per cent) (see Figure 16.1). Brief interventions for smoking and overweight or obesity, and follow-up of abnormal lipid profile were more likely in urban areas than regional or remote areas.24
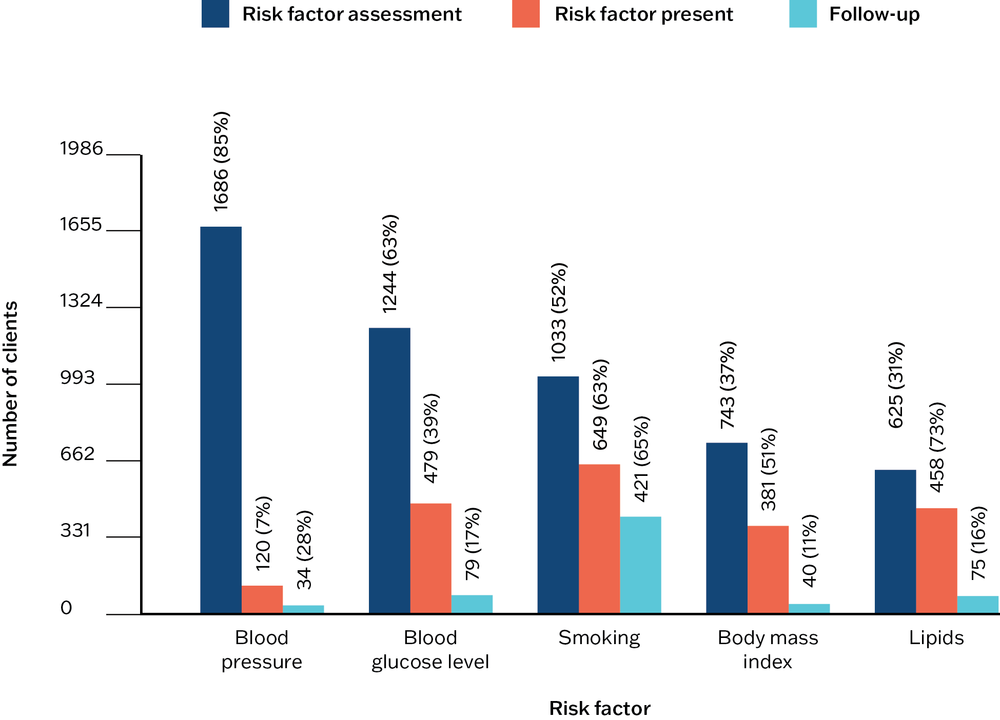
Figure 16.1 Number of clients with documented cardiovascular risk factor assessment and management. Source: Crinall, Boyle et al. 2017.
Study 3: Adults with diabetes
Many people with diabetes have an increased CVD risk. A study of clinical records for 1,728 clients with diabetes from 121 health centres (2012–14) in four jurisdictions quantified the extent to which health centre and client characteristics influenced variation in the delivery of CVD risk assessments.25
- 33 per cent of eligible clients had a documented risk assessment, with delivery ranging from 3 to 56 per cent between jurisdictions.
- There were gaps in the recording of CVD risk.
- Health centre characteristics accounted for 70 per cent of the variation in assessments.
- Access to decision support tools and a reporting process for the provision of assessments supported delivery of assessments.
- Women were more likely to have a CVD risk assessment than men – and generally accessed preventive health services more often than men.26
Health system factors that appeared to facilitate CVD risk assessments in these health centres were the inclusion of CVD risk assessments into routine adult health checks and standard treatment manuals, and access to a user-friendly electronic cardiovascular risk assessment calculator in clinical information systems.
Health system factors that appeared to facilitate CVD risk assessments were the inclusion of CVD risk assessments into routine adult health checks and standard treatment manuals, and access to a user-friendly electronic cardiovascular risk assessment calculator in clinical information systems.
Case study: strengthening cardiovascular disease prevention and management as part of holistic care
The CVD risk assessment strategies described above were among the outcomes of an earlier study by Burgess and colleagues, which informed a chronic disease strategy in one Australian jurisdiction (the Northern Territory).27 The strategy included staff education about the use of CVD risk assessments, outreach support by chronic care educators and CQI facilitators for implementing CVD risk assessments, and a reporting process for delivery of CVD risk assessments and follow-up care.28
The strategy was replaced in 2012 by a chronic conditions management model that feeds back actionable data to frontline PHC teams to support CQI.29 Client data are collected from the electronic health records and uploaded nightly to a centralised data warehouse. Data are then extracted, cleaned and turned into automated reports for the prevention and management of chronic conditions.30 Box 16.1 outlines the latest version of the model.
Box 16.1 The Northern Territory Department of Health Chronic Conditions Management Model
PHC centres receive the following information to feed into CQI activities and clinic meetings.
- Weekly “Recall List” for clinicians that identifies clients who are overdue for care in accordance with their care plans and risk factors.
- Weekly “Full Patient List” for clinicians detailing chronic conditions diagnoses, pathology results, key risk factors, examination findings and care plans. The ability to filter enables at-risk clients to be identified.
- Weekly community “Traffic Light Report” for clinicians and practice managers that compares service performance against chronic conditions program targets and chronic disease key performance indicators, including cardiovascular risk assessment and cardiovascular disease risk-management targets.
- Real-time dashboard (updated monthly) to track trends in regional and Northern Territory–wide service performance against Chronic Conditions Management Model program targets over the past three years. This allows clinicians and practice managers to identify problem areas or disseminate best-practice lessons.31
The functional reporting with embedded CQI has resulted in strong engagement from frontline PHC teams and improved delivery of CVD risk assessments. In the first two years of implementation of the chronic conditions management model, population coverage of CVD risk assessments increased from 23 per cent to 58.5 per cent for 7,266 clients. Functional reporting and decision support were also associated with a sustained proportion of high-risk clients achieving clinical targets for CVD risk reduction.32
The functional reporting with embedded CQI has resulted in strong engagement from frontline PHC teams and improved delivery of CVD risk assessments.
During the same period, guidelines for cardiovascular risk assessment were published in the standard treatment manual for PHC practitioners in remote and rural communities,33 and CQI research and development progressed through the Audit and Best Practice in Chronic Disease (ABCD) program.34 Clinical outcomes have been studied to identify improvements, trends over time and to inform policymaking and ongoing investment in both primary and secondary prevention.35
The Chronic Conditions Management Model and systems development, a comprehensive CQI strategy36 and increased workforce investment have been integral to the Northern Territory’s strategic and sustained approach to chronic conditions prevention and management.
Key messages for improving cardiovascular health care
This CQI research and other relevant studies identify clear priorities and strategies for improving cardiovascular risk assessment, follow-up and management in PHC. Patterns of cardiovascular care delivery in Aboriginal and Torres Strait Islander PHC communities may to some extent reflect care delivery in international settings.
For primary prevention of cardiovascular disease, these are the key actions to take:
- increase awareness of the risk factors for and understanding of cardiovascular disease in the community, including among teenagers and young adults
- link clients and families with health promotion programs that support health (for example, to support healthy eating, regular exercise, not smoking, and social and emotional wellbeing)
- encourage clients and their families to attend PHC centres for preventive health assessments, not just for acute care
- work with individual clients to reduce CVD risk (for example, by not smoking, by losing weight), and to manage identified risk factors (for example, high blood pressure, high cholesterol)
- promote the benefits of CVD risk assessments, particularly amongst groups who are least likely to access PHC (for example, young men)
- work with clients to manage diagnosed cardiac conditions, diabetes and chronic kidney disease.
PHC system changes that can improve cardiovascular care include:
- involving clients and families in CQI processes
- ensuring adequate data are collected about clients to calculate CVD risk
- strengthening systems to enhance follow-up treatment for clients with identified risk factors
- educating PHC teams on the importance of assessing CVD risk, including for young adults
- training PHC practitioners to assess CVD risk and providing appropriate decision-support tools (for example, automated calculators, support from CVD experts, functional reporting of CVD assessment and care)
- routinely calculating CVD risk to inform management plans rather than focusing treatment on individual risk factors
- training staff to provide interventions that support clients to make lifestyle, behaviour, physical activity and dietary changes to reduce their CVD risk, while respecting the person’s age, gender, cultural needs, ethnicity, social and economic circumstances and communication needs
- training and supporting PHC teams in using CQI processes to improve cardiovascular care.
There is also work that can be done at the policy level:
- advocate for policies and programs that support people to adopt and sustain healthy behaviours, such as nutritious food choices, increased physical activity, smoking cessation and reduced alcohol intake
- include cardiovascular risk assessment as a key performance indicator for PHC services
- provide transparent performance reporting to PHC teams and benchmark them against comparable services to lever internal motivation of clinical staff
- support the use of CQI in PHC services.
Improving cardiovascular care in Aboriginal and Torres Strait Islander PHC
Our studies show the need to improve the delivery of cardiovascular risk assessment for Aboriginal and Torres Strait Islander peoples. This is consistent with other research that shows under-treatment, with up to half of Aboriginal and Torres Strait Islander people found to be at high CVD risk not receiving recommended medication.37 Improved preventive care, CVD risk assessment and best-practice management need to come together to help reduce the CVD events and related deaths that currently occur in our Aboriginal and Torres Strait Islander population, on average, about 10–20 years earlier than in non-Indigenous Australians.38 Particular concerns are the risk of heart disease for young adults, poorer PHC access by men, and the need to ensure access to CVD risk factor screening and CVD risk assessments in line with best-practice clinical guidelines.
Recent developments are encouraging. Increased uptake of preventive health assessments by Aboriginal and Torres Strait Islander people has increased opportunities for early CVD risk assessment, prevention and management. The updated Australian guideline for assessing and managing cardiovascular disease risk 2023 recommends commencing risk factor screening and CVD risk assessment at an earlier age for Aboriginal and Torres Strait Islander peoples (as outlined above),39 and resources for supporting Aboriginal and Torres Strait Islander clients and communities to prevent and manage CVD risk can be found online. A consistent approach to risk assessment and management from an early age needs to be combined with increased health service capacity to deliver CVD prevention and care as part of holistic, culturally safe PHC. Use of CQI can support and sustain improvements in CVD care.
Within PHC services, practice infrastructure and systems need to be strengthened to increase follow-up care and self-management support for clients with identified CVD risk factors and diagnosed CVD.40 This may require overcoming barriers such as lack of staff time and capacity, inadequate numbers of Aboriginal and Torres Strait Islander staff to guide and deliver culturally appropriate care, and poor availability of culturally appropriate services for Aboriginal and Torres Strait Islander clients who need referral to other providers. Understanding of the competing cultural, family and personal responsibilities, and the logistical challenges that can delay clients accessing specialist and hospital care is crucial when planning referral and communicating with clients about their care needs.41
At a higher policy level, incentives designed to increase the delivery of preventive health assessments (for example, specific Medicare rebates) need to be complemented with increased resources for providing follow-up care and management, particularly growing self-management support capacity within Aboriginal and Torres Strait Islander PHC services .42
Practitioners working with Aboriginal and Torres Strait Islander clients need to take account of non-behavioural risk factors when calculating risk and planning CVD management. Having diabetes, chronic kidney disease or chronic inflammation may increase CVD risk. Poor social and emotional wellbeing, linked with a history of disempowerment, ongoing racism and hardship, and grieving also place many Aboriginal and Torres Strait Islander clients at higher risk of a cardiac event, or less able to make changes to reduce their CVD risks.43 Crowded housing and poor living conditions, linked to higher rates of infection, may affect CVD risk in some communities. Poor oral health, experienced by many Aboriginal and Torres Strait Islander people,44 is another risk factor.45 CVD risk scores are likely to underestimate real CVD risk for many Aboriginal and Torres Strait Islander people.46
Take account of non-behavioural risk factors when calculating risk and planning CVD management.
Prevention approaches that are community led and that take account of historical, cultural and socio-economic factors and community-identified health priorities are crucial,47 and require strong engagement between communities and PHC services. Within PHC teams, there is need to increase the Aboriginal and Torres Strait Islander clinical workforce, with emphasis on self-management support.48 At the higher system level, strategies are needed to address the social and cultural determinants of health – including racism,49 income and employment, education, housing and food security50 – in order to reduce the inequalities in cardiovascular health experienced by Aboriginal and Torres Strait Islander communities.
References
Agostino, J.W., D. Wong, E. Paige, V. Wade, C. Connell, M.E. Davey et al. (2020). Cardiovascular disease risk assessment for Aboriginal and Torres Strait Islander adults aged under 35 years: a consensus statement. Medical Journal of Australia 212(9): 422–7. DOI: 10.5694/mja2.50529.
Australian Bureau of Statistics (2019). National Aboriginal and Torres Strait Islander health survey, 2018–19. ABS cat. no. 4715.0. Canberra: ABS.
Australian Health Ministers’ Advisory Council (2017). Aboriginal and Torres Strait Islander Health Performance Framework 2017 report. Canberra: Australian Government.
Australian Institute of Health and Welfare (2022). Australia’s health 2022: data insights. Australia’s health series. Canberra: AIWH. DOI: 10.25816/vs-vr80.
Australian Institute of Health and Welfare (2021). Better cardiac care measures for Aboriginal and Torres Strait Islander people: sixth national report 2021. Cat. no. IHW 263. Canberra: AIWH.
Australian Institute of Health and Welfare (2019). Indicators of socioeconomic inequalities in cardiovascular disease, diabetes and chronic kidney disease. Cat. No. CDK 12. Canberra: AIHW.
Australian Institute of Health and Welfare (2015). Cardiovascular disease, diabetes and chronic kidney disease – Australian facts: Aboriginal and Torres Strait Islander people. Cardiovascular, diabetes and chronic kidney disease series no. 5. Cat. no. CDK 5. Canberra: AIHW.
Bailie, J., G. Schierhout, F. Cunningham, J. Yule, A. Laycock and R. Bailie (2014a). Quality of primary health care for Aboriginal and Torres Strait Islander People in Australia. Key research findings and messages for action from the ABCD National Research Partnership Project. Brisbane: Menzies School of Health Research.
Bailie, J., G. Schierhout, M. Kelaher, A. Laycock, N. Percival, L. O’Donoghue et al. (2014b). Follow-up of Indigenous-specific health assessments – a socioecological analysis. Medical Journal of Australia 200(11): 653–7. DOI: 10.5694/mja13.00256.
Barr, E., F. Barzi, A. Rohit, J. Cunningham, S. Tatipata, R. McDermott et al. (2020). Performance of cardiovascular risk prediction equations in Indigenous Australians. Heart 106(16): 1252. DOI: 10.1136/heartjnl-2019-315889.
Burgess, C., R. Bailie, C. Connors, R. Chenhall, R. McDermott, K. O’Dea et al. (2011). Early identification and preventive care for elevated cardiovascular disease risk within a remote Australian Aboriginal primary health care service. BMC Health Services Research 11: 24. DOI: 10.1186/1472-6963-11-24.
Burgess, C., G. Sinclair, M. Ramjan, P. Coffey, C. Connors and L. Katekar (2015). Strengthening cardiovascular disease prevention in remote Indigenous communities in Australia’s Northern Territory. Heart, Lung and Circulation 24(5): 450–7. DOI: 10.1016/j.hlc.2014.11.008.
Calabria, B., R. Korda, R. Lovett, P. Fernando, T. Martin, L. Malamoo et al. (2018). Absolute cardiovascular disease risk and lipid-lowering therapy among Aboriginal and Torres Strait Islander Australians. Medical Journal of Australia 209(1): 35–41. DOI: 10.5694/mja17.00897.
Coffey, C., Y. Zhao, J. Condon, S. Li and S. Guthridge (2020). Acute myocardial infarction incidence and survival in Aboriginal and non-Aboriginal populations: an observational study in the Northern Territory of Australia, 1992–2014. BMJ Open 10(10): e036979. DOI: 10.1136/bmjopen-2020-036979.
Commonwealth of Australia as represented by the Department of Health and Aged Care (2023). Australian guideline for assessing and managing cardiovascular disease risk 2023. Canberra: Department of Health and Aged Care.
Copley, K. and L. Patel (2021). The Northern Territory Continuous Quality Improvement Strategy. Darwin: Aboriginal Medical Service Alliance Northern Territory.
Crinall, B., J. Boyle, M. Gibson-Helm, D. Esler, S. Larkins and R. Bailie (2017). Cardiovascular disease risk in young Indigenous Australians: a snapshot of current preventive health care. Australian and New Zealand Journal of Public Health 41(5): 460–6. DOI: 10.1111/1753-6405.12547.
Humphrey, L., R. Fu, D. Buckley, M. Freeman and M. Helfand (2008). Periodontal disease and coronary heart disease incidence: a systematic review and meta-analysis. Journal of General Internal Medicine 23(12): 2079–86. DOI: 10.1007/s11606-008-0787-6.
Katzenellenbogen, J., E. Haynes, J. Woods, D. Bessarab., A. Durey, L. Dimer et al. (2015). Information for action: improving the heart health story for Aboriginal people in Western Australia (BAHHWA report). Perth: Western Australian Centre for Rural Health, University of Western Australia.
Matthews, V., C. Burgess, C. Connors, E. Moore, D. Peiris, D. Scrimgeour et al. (2017). Integrated clinical decision support systems promote absolute cardiovascular risk assessment: an important primary prevention measure in Aboriginal and Torres Strait Islander primary health care. Frontiers in Public Health 5: 233. DOI: 10.3389/fpubh.2017.00233.
Murray, J., C. Craigs, K. Hill, S. Honey and A. House (2012). A systematic review of patient reported factors associated with uptake and completion of cardiovascular lifestyle behaviour change. BMC Cardiovascular Disorders 12(1): 120. DOI: 10.1186/1471-2261-12-120.
National Institute for Health and Care Excellence 2023 (2014). Cardiovascular disease: risk assessment and reduction, including lipid modification CG181. London: NICE.
Paradies, Y., J. Ben, N. Denson, A. Elias, N. Priest, A. Pieterse et al. (2015). Racism as a determinant of health: a systematic review and meta-analysis. PLOS One 10(9): e0138511. DOI: 10.1371/journal.pone.0138511.
Productivity Commission (2021). Innovations in care for chronic health conditions. Productivity Reform case study. Canberra: Commonwealth of Australia.
Remote Primary Health Care Manuals, ed. (2022). CARPA standard treatment manual for remote and rural practice. Alice Springs, NT: Flinders University. https://www.remotephcmanuals.com.au/home.html.
Smith, G., R. Kirkham, C. Gunabarra, V. Bokmakarray and C. Burgess (2019). “We can work together, talk together”: an Aboriginal health care home. Australian Health Review 43(5): 486–91. DOI: 10.1071/AH18107.
Thompson, S., E. Haynes, J. Woods, D. Bessarab, L.A. Dimer, M. Wood et al. (2016). Improving cardiovascular outcomes among Aboriginal Australians: lessons from research for primary care. SAGE Open Medicine 4: 1–12. DOI: 10.1177/2050312116681224.
Vasant, B., V. Matthews, C. Burgess, C. Connors and R. Bailie (2016). Wide variation in absolute cardiovascular risk assessment in Aboriginal and Torres Strait Islander people with type 2 diabetes. Frontiers in Public Health 4: 37. DOI: 10.3389/fpubh.2016.00037.
Welsh, J., R. Korda, G. Joshy and E. Banks (2019). Primary absolute cardiovascular disease risk and prevention in relation to psychological distress in the Australian population: a nationally representative cross-sectional study. Frontiers in Public Health 7: 126. DOI: 10.3389/fpubh.2019.00126.
World Health Organization (2021). Cardiovascular diseases. https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1.
1 World Health Organization 2021.
2 Barr, Barzi et al. 2020.
3 Australian Institute of Health and Welfare 2019.
4 Welsh, Korda et al. 2019.
5 Murray, Craigs et al. 2012.
6 Australian Bureau of Statistics 2019.
7 World Health Organization 2021.
8 World Health Organization 2021.
9 Australian Institute of Health and Welfare 2021.
10 Australian Institute of Health and Welfare 2021, 2022.
11 Australian Institute of Health and Welfare 2021.
12 Agostino, Wong et al. 2020; Barr, Barzi et al. 2020.
13 Agostino, Wong et al. 2020.
14 Calabria, Korda et al. 2018.
15 Matthews, Burgess et al. 2017.
16 Commonwealth of Australia as represented by the Department of Health and Aged Care 2023; National Institute for Health and Care Excellence 2023 (2014).
17 Commonwealth of Australia as represented by the Department of Health and Aged Care 2023.
18 Commonwealth of Australia as represented by the Department of Health and Aged Care 2023.
19 Agostino, Wong et al. 2020; Barr, Barzi et al. 2020; Commonwealth of Australia as represented by the Department of Health and Aged Care 2023.
20 Commonwealth of Australia as represented by the Department of Health and Aged Care 2023.
21 Matthews, Burgess et al. 2017.
22 Matthews, Burgess et al. 2017.
23 Crinall, Boyle et al. 2017.
24 Crinall, Boyle et al. 2017.
25 Vasant, Matthews et al. 2016.
26 Vasant, Matthews et al. 2016.
27 Burgess, R. Bailie et al. 2011.
28 Vasant, Matthews et al. 2016.
29 Burgess, Sinclair et al. 2015.
30 Productivity Commission 2021.
31 Productivity Commission 2021.
32 Burgess, Sinclair et al. 2015.
33 Remote Primary Health Care Manuals 2022.
34 J. Bailie, Schierhout et al. 2014a.
35 Burgess, Sinclair et al. 2015; Coffey, Zhao et al. 2020; Matthews, Burgess et al. 2017.
36 Copley and Patel 2021.
37 Calabria, Korda et al. 2018.
38 Australian Institute of Health and Welfare 2015.
39 Commonwealth of Australia as represented by the Department of Health and Aged Care 2023; Agostino, Wong et al. 2020.
40 Thompson, Haynes et al. 2016.
41 Katzenellenbogen, Haynes et al. 2015.
42 J. Bailie, Schierhout et al. 2014b.
43 Australian Bureau of Statistics 2019.
44 Australian Health Ministers’ Advisory Council 2017.
45 Humphrey, Fu et al. 2008.
46 Agostino, Wong et al. 2020.
47 Katzenellenbogen, Haynes et al. 2015.
48 Smith, Kirkham et al. 2019.
49 Paradies, Ben et al. 2015.
50 Australian Institute of Health and Welfare 2019.