15
Improving mental health and wellbeing care
Mental health and wellbeing
Mental health is “an integral and essential component of health . . . a state of wellbeing in which an individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and is able to make a contribution to his or her community”.1 The diminishment of mental health can affect people of almost any age, and mental health disorders affect hundreds of millions of people globally. In 2019, mental health disorders caused approximately 5 per cent of the global burden of disease and 16 per cent of all years lived with disability.2 In Australia, mental health and substance use disorders accounted for 13 per cent of the total disease burden in 2018, the fourth-highest cause after cancer, cardiovascular diseases and musculoskeletal conditions, and almost half of all Australians will experience a mental health disorder at some stage in their lives.3 Youth is a particularly important life stage for prevention and early intervention, since 75 per cent of global mental illness starts by age 24.4 By 2030, depression is likely to be the second-highest cause of the global disease burden (second to HIV-AIDS) and the highest single contributor in high-income countries.5 People are more likely to have depression when they have physical illnesses (for example, diabetes, cancer)6 and may be more vulnerable to depression at particular life phases. A recent review found that 21 per cent of women worldwide experienced depression during pregnancy.7
Around the world, health systems are slow to respond effectively to the increasing burden of mental health disorders. In low- and middle-income countries, between 76 and 85 per cent of people with mental health disorders receive no treatment.8 In wealthy countries, insensitivity to client preferences, context and culture when treating mental disorders has led to waste and harm. The United States mental health system, for example, fails to reach more than half of people with the most serious mental health disorders.9
Integrating mental health services into PHC across the life course is a viable way of closing the treatment gap and increasing access to appropriate support.10 PHC has been found to deliver better care and clinical outcomes than psychiatric hospitals for common mental health disorders, such as depression, anxiety and substance disorders, and for less acute or severe mental illness.11 There are several likely reasons. For example, PHC staff with mental health training can provide a holistic and coordinated approach to care for people who experience mental illness in combination with physical health problems. Stigma for clients with mental illness may be reduced when seeking care at a PHC service (compared with using a stand-alone mental health service), making care more acceptable. Family life and employment, and client recovery, are less disrupted when treatment can occur closer to home.12 PHC also provides more scope for non-medicalised approaches, family and community involvement in mental health care, and care models that take account of social, political and cultural environments.13
Best-practice PHC for mental health includes prevention strategies, and screening, diagnosis and treatment for people with mental health disorders and mental health issues that affect wellbeing and physical health.14 Evidence has shown that with adequate training and support, PHC workers can screen clients for mental health and wellbeing issues, recognise psychological distress and mental health disorders, treat common problems such as anxiety and depression, and provide brief interventions for the management of hazardous substance use.15 But, traditionally, attempts to integrate mental health in PHC have been fraught with systems, resource and organisational challenges.16
The integration of mental health services into PHC requires multidisciplinary and collaborative care models supported by effective policy and systems.17 Complementary services are needed, particularly secondary care facilities and specialist mental health professionals to whom PHC practitioners can turn for referrals, support and supervision. Care tasks should be limited and doable by staff, and clients must have access to essential psychotropic medications. Good service coordination, and collaboration with non-health sectors such as education, social and spiritual welfare, justice or employment are required to support recovery and social and emotional wellbeing.18
Mental health and social and emotional wellbeing of Aboriginal and Torres Strait Islander peoples
Social and emotional wellbeing (SEWB) is a term preferred by many First Nations people because it includes, but extends beyond, conventional understandings of mental health and mental disorder.19 For Aboriginal and Torres Strait Islander Australians, SEWB is based on a holistic concept of health and culturally informed practices, “shaped by connections to body, mind and emotions, family and kinship, community, culture, land and spirituality”20 and by a range of social, historical, political and cultural influences (see Figure 15.1). People’s understanding of social and emotional wellbeing varies between different cultural groups and individuals, and may change across the life course (for example, factors important to a child’s SEWB compared with factors important to Elders).21
The domains of SEWB, as illustrated in Figure 15.1, can be seen as protective factors for Aboriginal and Torres Strait Islander mental health across the life course. For many people, good mental health comes through a collective sense of self and belonging, strong cultural identity, positive relationships and understanding of social roles, and connection to other aspects of life that are a source of strength and resilience. Conversely, poor mental health can be influenced by stressors such as grief and trauma, forced removal from family and Country, racism and discrimination, incarceration, displacement from culture, intergenerational trauma and economic exclusion22 – ongoing legacies of colonisation. Exposure to adverse experiences or stressful life events are risk factors for mental health disorders23 and “Western” mental health approaches that do not incorporate Aboriginal and Torres Strait Islander knowledge systems have contributed to poor access and treatment outcomes for many Aboriginal and Torres Strait Islander people.24
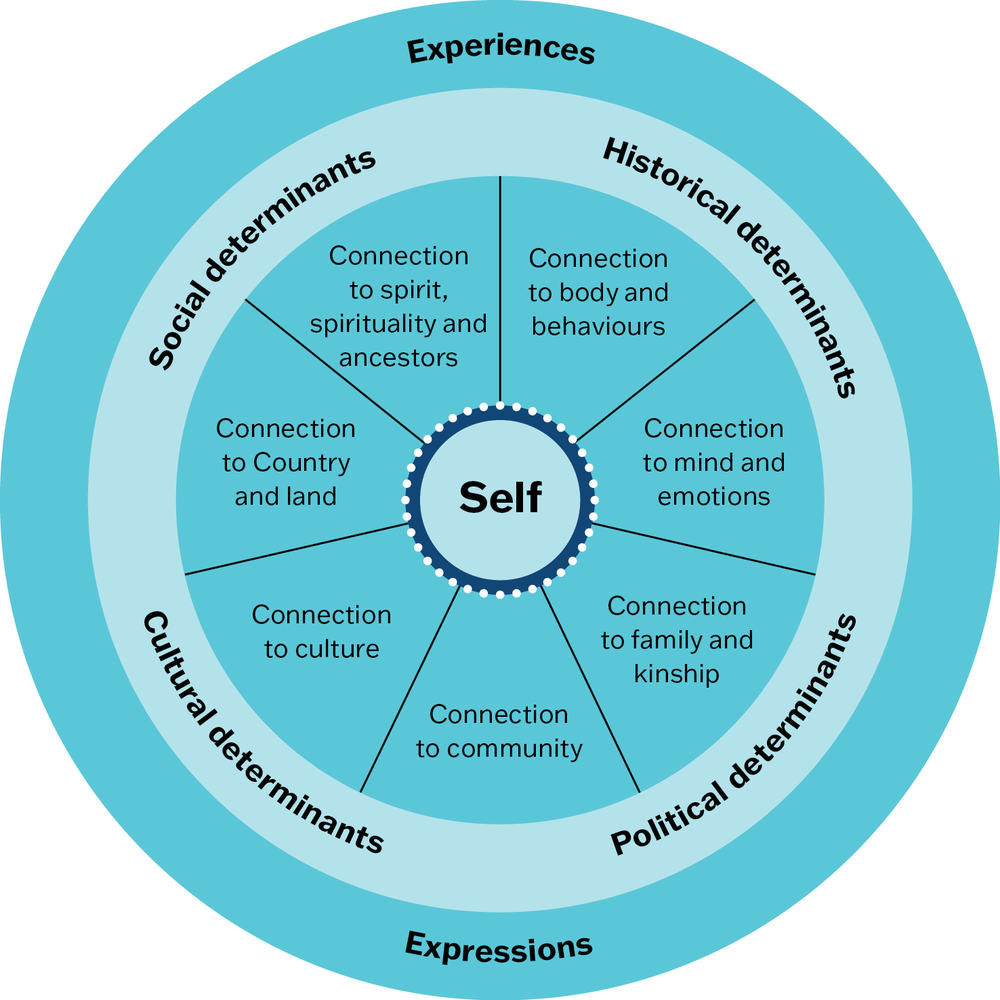
Figure 15.1 Social and emotional wellbeing (SEWB) from an Aboriginal and Torres Strait Islander perspective. Source: Adapted from Gee, Dudgeon et al. 2014.
Mental health and substance use disorders are a leading contributor (19 per cent) to the illness experienced by Aboriginal and Torres Strait Islander people.25 In 2018–19, an estimated 24 per cent (187,500) of those surveyed reported a mental health or behavioural condition, with a higher rate among men than women. Anxiety was most reported (17 per cent), followed by depression (13 per cent). Sixty-six per cent of adults reported “low or moderate” levels of psychological distress and 31 per cent reported “high or very high” levels.26 Lower access to primary mental health care according to need has resulted in over-representation of First Nations clients in other parts of the health and mental health system. Hospitalisation rates for mental health, behavioural disorders and alcohol-related conditions are disproportionally high and suicide rates are especially concerning.27
As discussed in Chapter 14, Aboriginal and Torres Strait Islander young people are deeply concerned about mental health. The Mission Australia 202228 youth survey found that, while 28 per cent of Aboriginal and Torres Strait Islander young people (aged 15–19) rated their mental health as excellent or very good, over one third (34 per cent) reported feeling high psychological distress. Forty per cent didn’t know where to go for help and only 62 per cent of those who sought help consulted a health professional. Accessible culturally safe treatment pathways that can cater for the complex sociocultural factors faced by Aboriginal and Torres Strait Islander children and young people are essential for healthy futures.
Improving the mental health and wellbeing of Aboriginal and Torres Strait Islander families and communities requires systemic and transformative change,29 deep respect for Indigenous perspectives on wellbeing, Indigenous-led responses and a workforce skilled in trauma-informed care. Current policies refer to the importance of strengthening the cultural – as well as social and biomedical – determinants of health through languages, relationships, customs and community networks.30 Across Australia, Aboriginal and Torres Strait Islander communities have developed programs to strengthen Indigenous identity, resilience, wellbeing and empowerment. These programs, like the Family Wellbeing Program (see Box 15.1), focus on strengths while also reducing social and emotional wellbeing stressors (risks) and improving the capacity of communities and services to cope with these.31 They are an important part of comprehensive primary health care for Aboriginal and Torres Strait Islander people.
Box 15.1 The Family Wellbeing Program
The Family Wellbeing Program is a learning and empowerment program based on Aboriginal and Torres Strait Islander cultural knowledge and frameworks, while incorporating Western knowledge. Completion of all five stages of the program provides participants with a nationally accredited qualification in counselling.32
“The Family Wellbeing Program involves teaching participants about social and emotional needs in a way that allows them to go on and share this learning with others … It teaches problem-solving skills that help us to build resilience and deal with managing relationships, conflicts, addiction and violence. We then use this empowerment to … bring community members together to take action on larger social issues that matter to us.”
– Leslie Baird, National Centre for Family Wellbeing.
Since the Family Wellbeing Program was developed in 1993, by and for Aboriginal people, the program has been adapted and delivered in at least 60 locations. It has helped Aboriginal and Torres Strait Islander participants to take control over the conditions affecting their lives and target critical issues like suicide using community-based solutions. Quality improvement processes have been used to adapt the program to local communities.33
There is further potential to use CQI to systematically strengthen links between program activities and clinical PHC, and to capture and build on community wellbeing stories.
Recommended mental health and social and emotional wellbeing care in clinical PHC
Stresses on social and emotional wellbeing exist for all populations and all age groups. Therefore, screening and care for social and emotional wellbeing is relevant across the life course and as part of the management of many health conditions. It can prevent mental health and wellbeing issues from developing into more serious disorders and supports early intervention. High-quality PHC supports children and adults living with mental illness – and those who care for and support them – with effective clinical and non-clinical services.
These are among the essential clinical services in PHC:
- mental health and social and emotional wellbeing promotion and prevention services
- screening for social and emotional wellbeing
- brief interventions or referral when people are assessed as at risk for social and emotional wellbeing challenges
- screening, brief interventions and referral for substance misuse
- early identification and treatment of mental health disorders
- management of stable psychiatric clients
- counselling for common mental health disorders
- referral to other services when required.
PHC practitioners should provide client-centred care within their expertise and capabilities, and coordinate clients’ access to other care providers (for example, psychologists, social workers, occupational therapists) and appropriate agencies. These might be government, private or community-based services, cultural healers, community Elders or religious leaders, community or family members.
Some clients experience multiple social and emotional wellbeing and mental health issues in addition to the negative effects of social determinants such as poverty, racism and housing issues. In these circumstances, it may be appropriate to begin with case management and problem-solving approaches to tackle these issues, and to support clients to establish safety, security and stability before focusing on other healing processes.34 Individualised mental health care plans can provide a framework for coordination and continuity of care. A well-designed care plan, reviewed on a regular basis, promotes communication across disciplines and client engagement.
Clinical practice guidelines are available for the prevention and management of mental health disorders. They include guidelines for managing specific conditions, such as depression, complex trauma and post-traumatic stress, and guidelines for working with specific groups, such as refugees or First Nations people. We recommend searching reliable online sources for guidelines and resources that are relevant for your PHC context and clients’ needs.
Findings: quality of mental health care
The data presented below come mainly from six research papers and a key report published by the ABCD CQI research program between 2011 and 2019. A mental health audit tool35 and the systems assessment tool36 were used to collect data about the delivery of mental health care from 21 PHC centres between 2009 and 2014. These are the most recent audit data available. Analysis was conducted on 975 records for Aboriginal and Torres Strait Islander clients with a diagnosed mental health disorder to assess how well care reflected best-practice guidelines for mental health and wellbeing care. Stakeholders participated in data interpretation to identify priority evidence–practice gaps and factors influencing improvement.
Routine items of mental health care
Risk factors and brief interventions
Analysis of 314 client records in 17 services (2012–2014) found that, in the 12 months before the audit, the recording of risk factors and brief interventions varied between PHC centres and risk factors:
- 80 per cent of mental health clients had their alcohol use recorded; 70 per cent of high-risk alcohol users received brief interventions or counselling for alcohol use
- 85 per cent had their tobacco use recorded; 55 per cent of smokers received brief interventions or counselling for smoking
- 75 per cent (range 30–100 per cent) of clients who had drug misuse noted received brief intervention or counselling for drug misuse
- 33 per cent (range 0–80 per cent) of clients with a body mass index of more than 25 had a record of brief intervention or counselling for overweight or obesity
- the recording of mental health risk factors and interventions varied widely across PHC centres.37
Follow-up if mental health deteriorated
The research also examined whether follow-up action was recorded for clients who experienced worsening or deteriorating symptoms and behaviours related to a mental health disorder. These concerns included sleep patterns and mood, hallucinations, psychotic symptoms, medication side effects, aggressive behaviour, social withdrawal or deterioration in self-care. When worsening symptoms were recorded in client records:
- an average of 70 per cent of clients (range 30–100 per cent) were referred to another health professional, and 75 per cent received psychosocial or culturally appropriate interventions
- 70 per cent of clients had their medication reviewed; 40 per cent of these clients had their medication adjusted.38
Mental health care plans and shared care arrangements
- On average, only 50 per cent of mental health clients had a mental health care plan.
- Where care plans were recorded, most included both clinical goals and self-management or recovery goals (average of 90 per cent and 83 per cent respectively). There was more variation in the recording of self-management or recovery goals than clinical goals.
- Review of goals in the three months before the audit varied widely across PHC centres (average of 65 per cent; range 0–100 per cent) (see Figure 15.2).39
- Shared care arrangements and referrals were not well documented (median 55 per cent, range 0–100 per cent).40
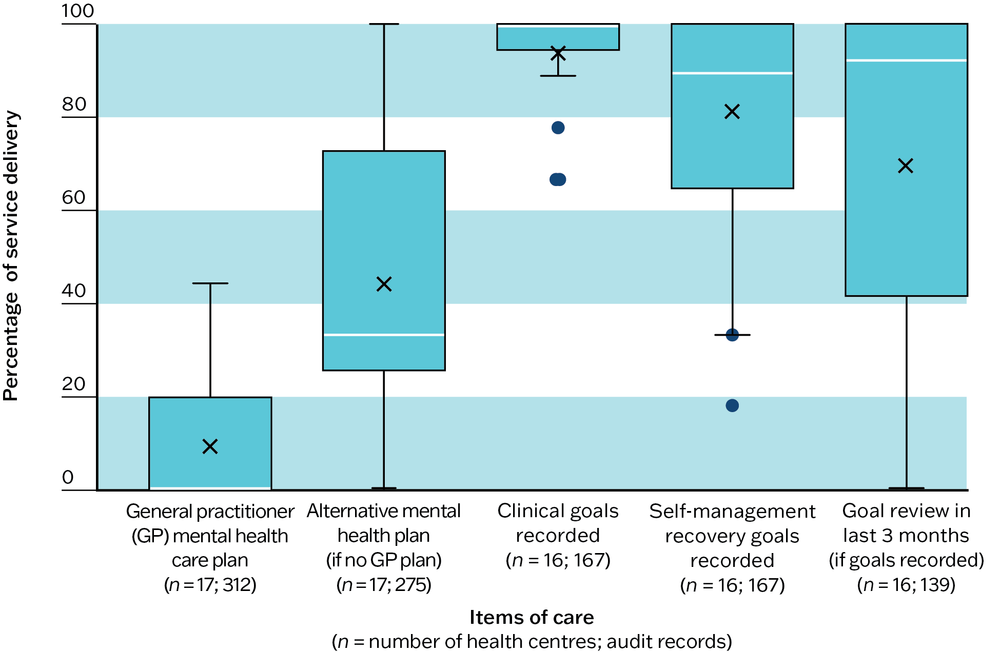
Figure 15.2 Mean percentage of health centre clients with a care plan and associated goals in their medical records. Source: Matthews, J. Bailie et al. 2016.
Overall mental health care
We analysed mental health audit data from PHC centres over three years (2011–2013). While overall levels of service delivery for mental health care were steady, lower performing health centres had improved care for clients diagnosed with mental health conditions.
- There was no clear improvement in the overall service delivery of mental health and wellbeing care. The mean and median level of care delivery was about 60 per cent over the three years (see Figure 15.3).
- There was less variation in quality of care between PHC centres, mainly because lower performing PHC centres improved their delivery of mental health services.
- Based on 12 best-practice indicators for mental health care, the lower performing PHC centres improved their overall delivery of mental health care, from 30 per cent in 2011 to around 50 per cent in 2012 and 201341 (see Figure 15.3).
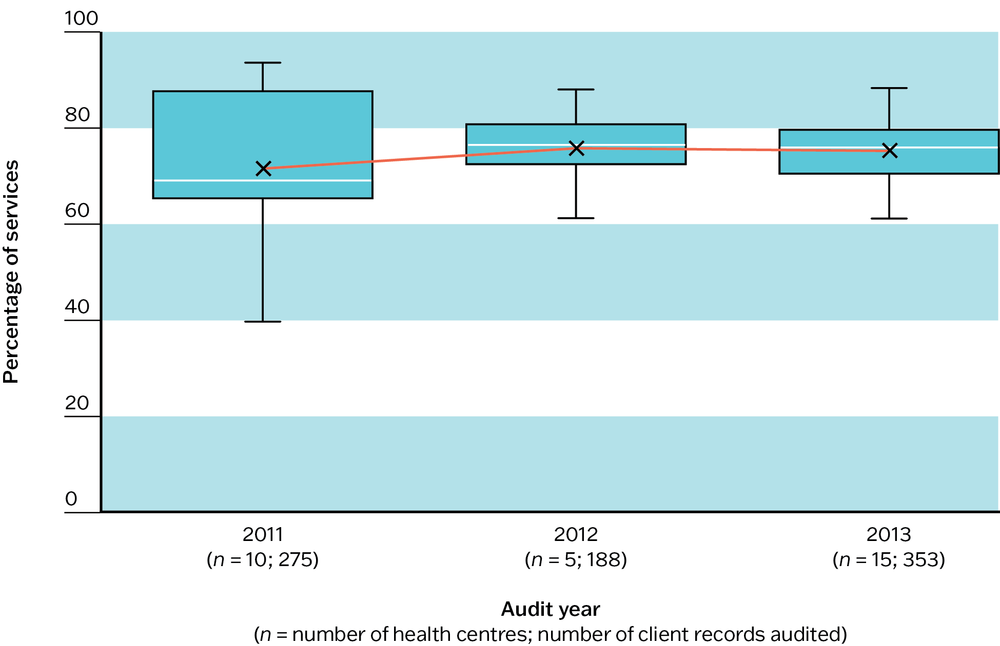
Figure 15.3 Trends in overall mental health care for 12 best-practice indicators. Source: Matthews, J. Bailie et al. 2016.
The 12 best-practice indicators were recording of alchohol, tobacco and drug use; brief interventions for alcohol and drug misuse; health check withing the last 12 months; blood pressure check within the last 6 months; mental health assessment, if client had attended within the last 3 months; provision of social issues and family or individual counselling, if client had attended within the last 3 months; joint discussion regarding culturally appropriate interventions, if client had attended within the last 3 months; liver function test; serum creatinine; thyroid function test; full blood count; and follow-up action, including medication review and adjustment, referral or psychosocial or culturally appropriate intervention if deterioration in symptoms.
Systems supporting mental health care
Twenty-nine assessments of the PHC systems supporting mental health care were also analysed by researchers and PHC stakeholders. Systems assessments evaluate delivery system design, information systems and decision support, client self-management support, links with community, other health services and resources, and organisational influence and system integration.42 There were two key findings for informing system improvement:
- 100 per cent of surveyed stakeholders viewed organisational commitment to structures and processes for safe, high-quality mental health care as a priority for improvement
- 90 per cent viewed community involvement in planning mental health and wellbeing services as a priority.43
Findings: quality of screening and care for social and emotional wellbeing
The findings about the quality of screening and care for social and emotional wellbeing come from the use of four ABCD audit tools: adult preventive care, type 2 diabetes care, maternal care and child health. Altogether, more than 9,400 health records were analysed. Across the audit data, patterns emerged about the quality of social and emotional wellbeing care.
Preventive care
Preventive health records for 3,407 adults in 100 PHC centres (2012–2014) were analysed. According to health records:
- social and emotional wellbeing screening was not undertaken for 73 per cent of clients
- no further action was taken for 25 per cent of screened clients for whom a concern was recorded
- when a treatment plan was documented, follow-up was poor.
As Figure 15.4 illustrates, this represents a combined management gap of 75 per cent.
The analysis also found there was more screening of younger adults (younger than 30 years) and people older than 55 years compared with other age groups. Lower rates of screening were associated with larger service populations (more than 1,000) and health service participation in fewer CQI cycles.44
It is a similar story across care for health conditions, not just for preventive care.
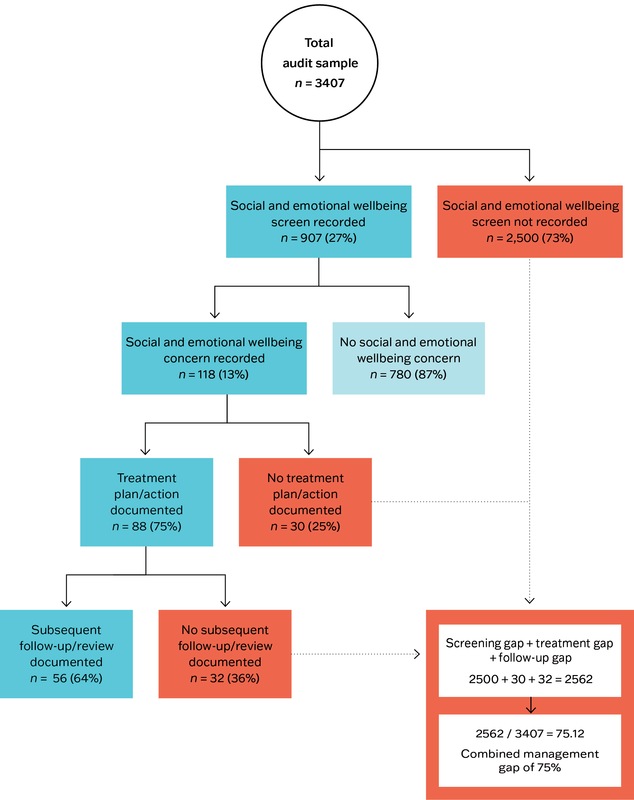
Figure 15.4 Social and emotional wellbeing screening and management: gaps in screening, treatment and follow-up. Source: Langham, McCalman et al. 2017.
Diabetes care
Comorbidity of mental health disorders with chronic conditions is common. Given the increased likelihood of poor levels of SEWB for those with diabetes, screening and follow-up action is an important aspect of clinical care. A study of 1,174 records of people with diabetes from 44 PHC centres (2009) also found low screening rates for social and emotional wellbeing.
- Only 5 per cent of clients with diabetes had been screened, with only four of the 44 PHC centres using a standard depression or distress screening tool in the past year.
- 37 to 67 per cent of people with diabetes were screened in those health centres where screening had been done. A record of screening was much less likely for people with severe diabetes-related disease compared to people with less severe disease.
- Documented depression ranged from 0 to 33 per cent between health centres. Regardless of whether they had been screened, 6 per cent of clients across 24 health centres had a documented diagnosis of depression, while 5 per cent had a diagnosis of another mental illness.
- 39 per cent of clients with a current prescription for antidepressant medication did not have a documented diagnosis of depression or other mental illness in their health records.45
An earlier study of 1,592 records of people with diabetes from 62 PHC settings had also found inconsistencies in the recording of diagnoses for depression and prescribed medications:
- 62 out of the 140 clients with a recorded diagnosis of depression had no record of antidepressant medication being prescribed
- 45 clients with diabetes had a prescription for selective serotonin reuptake inhibitors (SSRIs) recorded, without a recorded diagnosis of depression.46
The study raised questions about whether health professionals working in Indigenous settings chose not to use screening tools based in Western medical models (see “Improving mental health and wellbeing care in Aboriginal and Torres Strait Islander PHC” section below), whether they resisted making a diagnosis of depression, or whether other mental disorders were being treated with antidepressant medications.
Pregnancy care
Analysis of 797 maternal health records from 36 PHC settings (2010–2012) found scope for improvement, particularly for emotional wellbeing screening.
- Only 17 per cent of all women had a record of emotional wellbeing screening during pregnancy, despite 86 per cent of women having at least four antenatal visits.
- Most women had records of assessment for social (79 per cent) and medical (86 per cent) risk factors, and risk factors such as use of cigarettes (78 per cent), alcohol (57 per cent) and illicit drugs (53 per cent) in pregnancy.
- Emotional wellbeing screening was more likely when social risk factors were noted, and when health professionals noted plans for care and birthing, antenatal education and breastfeeding.47
- 16 per cent of women identified at risk of depression were prescribed antidepressant drugs during their pregnancy.48
- Non-pharmaceutical interventions for pregnant women assessed as being at risk of having their SEWB affected included brief intervention (61 per cent), counselling (57 per cent) and cognitive behaviour therapy (5 per cent).
- About 39 per cent of women at risk of having their SEWB affected were referred to external services.49
Care for families of young children
Analysis of 2,466 health records of Indigenous children from 109 PHC centres (2012–14) found scope for improvement in service provision and in follow-up or referral when concerns were noted.
- PHC centres used the national best-practice guidelines for social and emotional wellbeing care and included important services (for example, advice about child stimulation and behaviour, and parent–child interaction).
- The proportion of families receiving social and emotional wellbeing services ranged from 11 per cent (advice about nutrition and food security) to 75 per cent (assessment of parent–child interaction).
- Almost 25 per cent of families had no clinical follow-up or referral for concerns about domestic environment, family support and financial situation, housing condition and food security.
- Families of children aged 3–11 months (40 per cent) were more likely to receive social and emotional wellbeing services than families of children aged 12–59 months (30 per cent).
- Families living in remote areas received similar services to rural and urban families.50
Emerging patterns and recent developments
Our research found that some aspects of social and emotional wellbeing care were being done well (for example, assessment of risk factors for pregnant women). However, data collected using four different audit tools (adult preventive care, type 2 diabetes care, maternal care and child health) showed many opportunities for improvement. There was considerable variation in quality of care between health centres. This is not surprising. Until recently, social and emotional wellbeing care received relatively less attention than care for physical conditions in PHC. Since we analysed these CQI data, there have been important developments in mental health, social and emotional wellbeing care and in suicide prevention for Aboriginal and Torres Strait Islander communities. Culturally sensitive screening tools (for example, aPHQ-9), 51 clinical guidelines and social and emotional wellbeing services have become more widely available. We would expect these developments to be reflected in more recently collected CQI data. Services that start from a low baseline have greater potential for large and rapid improvements in care quality.
Services that start from a low baseline have greater potential for large and rapid improvements in care quality.
Australia has adopted a stepped care model of primary mental health care. Stepped care aims to deliver the most effective yet least resource-intensive treatment to clients first, only “stepping up” to intensive and specialist services as clinically required.52 CQI has an important role in advancing the system changes needed to strengthen stepped care and to implement further evidence-based developments. CQI processes can be used to improve systems at each of the five steps:
- health promotion and preventive care for well populations
- early intervention for at-risk groups
- access to low-intensity services for those with mild mental illness
- provision of services and interventions for people with moderate illness
- adequate levels of intervention to maximise recovery, prevent escalation and provide wraparound coordinated care for people with severe mental illness.
Key messages for improving mental health and wellbeing care in PHC
Although there are important differences between settings, the patterns of delivery for mental health and wellbeing care in Aboriginal and Torres Strait Islander PHC are likely to reflect care delivery in many international settings. In addition, the issues experienced and the solutions suggested by Aboriginal and Torres Strait Islander communities may be relevant to other populations that experience a high burden of grief and trauma.
The CQI research (2005–14) supports long-standing key messages from international PHC53 about how to improve mental health and wellbeing care across the life span, as part of PHC. There is a need for these features to be acted on:
- organisational commitment to a culture, structures and processes that promote high-quality mental health and wellbeing care across the life span
- integrated care strategies that are tailored to PHC and community settings
- teamwork that creates collaborative healthcare teams with the right mix of skills and clear allocation of roles and responsibilities
- training, supervision and support of PHC staff by mental health professionals
- strong links between PHC services, communities, schools and support groups for mental health promotion and prevention, service planning and resource development
- connection by PHC services with other agencies and sectors that address social, economic and environmental determinants of health (for example, safety, social support, housing, education, employment, food security)
- embedding of CQI processes into mental health and wellbeing services and programs.
Common gaps
To improve care for people diagnosed with a mental health disorder, systems need to be strengthened in these ways:
- increase staff understanding of mental health and disorders, and ability to recognise and respond to psychosocial distress and depression
- record mental health plans, shared care arrangements and referrals
- record risk factors and brief interventions, particularly for alcohol and drug misuse
- follow up clients with mental disorders whose symptoms are getting worse.
To improve social and emotional wellbeing care for all clients, systems need to be strengthened in these ways:
- educate staff to understand the many influences on social and emotional wellbeing, including risk factors and protective factors specific to population groups served (for example, LGBTQI+ people, refugees, Indigenous people)
- train PHC staff in social and emotional wellbeing assessment, brief interventions, counselling and management
- provide social and emotional wellbeing screening across client groups of all ages as part of holistic care
- document wellbeing assessments, actions taken and follow-up care in client health records54
- integrate community-based, youth-guided and children- and family-centred care into social and emotional wellbeing services55 (see also Chapter 14).
All of these strategies require ongoing policy commitment to improve PHC systems and resources for providing high-quality mental health and wellbeing care.
Improving mental health and wellbeing care in Aboriginal and Torres Strait Islander PHC
Our CQI research findings support calls for strategies that integrate mental health and social and emotional wellbeing care into PHC; engage communities in social and emotional wellbeing programs; and strengthen cross-sector action to address mental health risks and protect wellbeing. Community-controlled health services are well positioned to lead the way in developing such strategies, because they have developed from models of comprehensive PHC based on a holistic concept of health with the cultural, social and emotional wellbeing of families at their centre.56
Whatever governance arrangements are in place, responding to high demands for acute and chronic illness care amongst service populations can constrain the capacity of PHC services to provide social and emotional wellbeing services. In addition, practitioners working in Aboriginal and Torres Strait Islander communities are often confronted with complex client presentations for mental health care. For example, community members may be simultaneously experiencing mental health issues, loss and cultural disconnection, financial hardship and child removal.57 Aboriginal and Torres Strait Islander staff may themselves experience significant wellbeing stressors, including stressors that come from identifying with the trauma experienced by their clients. Supporting the social and emotional wellbeing of the Aboriginal and Torres Strait Islander workforce is critical.
Our CQI research identified enablers for improving mental health and wellbeing care for Aboriginal and Torres Strait Islander clients and communities, including these features:
- good systems for recruiting, supporting and retaining PHC staff, particularly Aboriginal and Torres Strait Islander staff
- strong systems for providing PHC teams with training and support from mental health professionals
- effective strategies for building and sharing staff understanding and skills in culturally appropriate mental health and wellbeing care
- strong links between health services, communities and other agencies providing mental health and SEWB care, focusing on holistic and strengths-based approaches.58
The research findings showed that, at the time of data collection, many opportunities for social and emotional wellbeing screening and care were not taken up. One suggested reason was practitioners’ concern about the cultural suitability of screening tools based on Western medical models. This concern is being tackled through the development or adaptation of assessment tools such as the Here and Now Aboriginal Assessment tool,59 the Aboriginal and Torres Strait Islander Perinatal Mental Health guide for PHC professionals60 and the adapted Patient Health Questionnaire 9, which has phrasing culturally adapted for five Australian Aboriginal language groups.61 The Centre of Best Practice in Aboriginal and Torres Strait Islander Suicide Prevention Clearing House has links to a range of validated tools and checklists. The National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people includes guidance for the prevention of depression and suicide.62 The uptake of screening tools should continue to improve as more culturally based tools and guidelines are developed.
Screening alone provides minimal benefit and has the potential to cause harm.63 To be beneficial at an individual client or population level, screening needs to be part of a broader, culturally competent assessment process entailing these aspects:
- formal training in culturally appropriate assessment
- a comprehensive client interview to explain and determine the appropriate assessment processes and any required screening
- reflective documentation of the process
- interpretation and reporting of results using cultural explanations and avoidance of labelling.64
As with all clinical assessments, there must be systems in place to ensure that a diagnosis of abnormal findings is followed by guideline-based treatment and follow-up care.65
Screening tools focus on identifying deficits and risk factors. While these are useful, identifying strengths and protective factors is integral to a comprehensive assessment66 and can support a social and emotional wellbeing care plan that helps to empower the person. Such a plan builds on individual, family and community strengths (for example, education, loving family, support networks, cultural involvement). Resources for frontline health and wellbeing workers, made by and for Aboriginal and Torres Strait Islander people, are brought together on the Wellmob website.67 Other resources are available.68
Aboriginal and Torres Strait Islander leadership and policy support for social and emotional wellbeing, mental health and suicide prevention are well established.69 In communities, culturally capable and responsive PHC services, shaped by community-led health initiatives, have a key role in protecting social and emotional wellbeing, improving mental health and wellbeing care and supporting the self-determination of individuals and communities. PHC teams need to be supported by respected community leaders and organisations, using best-practice guidelines that identify appropriate strategies for developing care plans, including protocols for treatment, referral pathways and follow-up with PHC staff.70
The use of CQI supports PHC teams and communities to improve mental health and social and emotional wellbeing care. Coordination between health and other service providers, such as education, employment, housing and justice, will help to support a holistic approach to promoting social and emotional wellbeing (see Box 15.2).71
Box 15.2 Improving social and emotional wellbeing services for boarding school students
In recent years, Australian government policies have promoted access to secondary education through boarding schools for Aboriginal and Torres Strait Islander students from remote communities. These students experience the poorest health of any Australian adolescent group. Adjusting to being away from family and community, changes in culture and language, school and academic expectations can further challenge wellbeing. While these students have high levels of risk and distress, they report themselves as having good health: this raises the possibility that they are normalising stress. This in turn creates the potential that boarding schools may fail to identify students’ needs and refer the students appropriately.72
Boarding school health staff support student-centred health care and wellbeing by weaving a relational network with students, families, school staff and external healthcare providers, but as one Aboriginal and Torres Strait Islander healthcare practitioner commented: “It can’t just be left to individuals to know everybody. It’s gotta be in the system and we’ve got to work out ways to make sure that none of our students drop through holes.”73
Providing and integrating care to meet the needs of remote-dwelling Indigenous students is complex and needs an integrated, systems approach. Communication and feedback linkages between students, parents and kin, healthcare services and schools are key.74 A CQI approach can help to identify and take opportunities to strengthen systems for student care.
See also Chapter 14.
References
Anaf, J., F. Baum, T. Freeman, R. Labonte, S. Javanparast, G. Jolley et al. (2014). Factors shaping intersectoral action in primary health care services. Australian and New Zealand Journal of Public Health 38(6): 553–9. DOI: 10.1111/1753-6405.12284.
Australian Bureau of Statistics (2019). National Aboriginal and Torres Strait Islander health survey, 2018–19. Cat. no. 4715.0. Canberra: ABS.
Australian Indigenous HealthInfoNet. n.d. Edith Cowan University. https://healthinfonet.ecu.edu.au/.
Australian Institute of Health and Welfare (2022a). Australia’s health 2022: First Nations People – Indigenous health and wellbeing. Canberra: Australian Government.
Australian Institute of Health and Welfare (2022b). Mental health services in Australia: mental health: prevalence and impact. Canberra: Australian Government.
Australian Institute of Health and Welfare (2016). Australian Burden of Disease study: impact and causes of illness and death in Aboriginal and Torres Strait Islander people 2011. Australian Burden of Disease Study. Canberra: AIHW.
Beyondblue (2013). Aboriginal and Torres Strait Islander perinatal mental health: a guide for primary care health professionals. Melbourne: beyondblue.
Carson, B., T. Dunbar, R. Chenhall and R. Bailie, eds (2007). Social determinants of Indigenous health. Sydney: Allen & Unwin.
Commonwealth of Australia (2017). National Strategic Framework for Aboriginal and Torres Strait Islander Peoples’ mental health and social and emotional wellbeing 2017–2023. Canberra: Department of the Prime Minister and Cabinet.
Davis, M., B. Balasubramanian, E. Waller, B. Miller, L. Green and D. Cohen (2013). Integrating behavioral and physical health care in the real world: early lessons from Advancing Care Together. Journal of the American Board of Family Medicine 26(5): 588–602. DOI: 10.3122/jabfm.2013.05.130028.
Department of Health (2017). My life my lead – opportunities for strengthening approaches to the social determinants and cultural determinants of Indigenous health: report on the national consultations December 2017. Canberra: Commonwealth of Australia.
Dobrow, M., T. Sullivan, L. Rabeneck, V. Hagens and R. Chafe (2018). Consolidated principles for screening based on a systematic review and consensus process. Canadian Medical Association Journal 190(14): E422–E29. DOI: 10.1503/cmaj.171154.
Drake R., A. Binagwaho, H. Martell and A. Mulley. (2014). Mental health care in low and middle income countries. BMJ 349(g7086). DOI: 10.1136/bmj.g7086.
Dudgeon, P., A. Bray, D. Darlaston-Jones and R. Walker (2020). Aboriginal participatory action research: an Indigenous research methodology strengthening decolonisation and social and emotional wellbeing. Discussion Paper. Melbourne: Lowitja Institute.
Dudgeon, P., A. Bray, B. D’Costa and R. Walker (2017). Decolonising psychology: validating social and emotional wellbeing. Australian Psychologist 52(4): 316–25. DOI: 10.1111/ap.12294.
Dudgeon, P., H. Milroy and R. Walker, eds (2014). Working together: Aboriginal and Torres Strait Islander mental health and wellbeing principles and practice, 2nd edn. Canberra: Australian Council for Education Research and Telethon Institute for Child Health Research, Office for Aboriginal and Torres Strait Islander Health, Department of Health and Ageing.
Edmond, K., K. McAuley, D. McAullay, V. Matthews, N. Strobel, R. Marriott et al. (2018). Quality of social and emotional wellbeing services for families of young Indigenous children attending primary care centers; a cross sectional analysis. BMC Health Services Research 18(1). DOI: 10.1186/s12913-018-2883-6.
Funk, M., S. Wutzke, E. Kaner, P. Anderson, L. Pas, R. McCormick et al. (2005). A multicountry controlled trial of strategies to promote dissemination and implementation of brief alcohol intervention in primary health care: findings of a World Health Organization collaborative study. Journal of Studies on Alcohol and Drugs 66(3): 379–88. DOI: 10.15288/jsa.2005.66.379.
Gausia, K., S. Thompson, T. Nagel, A. Rumbold, C. Connors, V. Matthews et al. (2013). Antenatal emotional wellbeing screening in Aboriginal and Torres Strait Islander primary health care services in Australia. Contemporary Nurse: A Journal for the Australian Nursing Profession 46(1): 73–82. DOI: 10.5172/conu.2013.46.1.73.
Gausia, K., S. Thompson, T. Nagel, G. Schierhout, V. Matthews and R. Bailie (2015). Risk of antenatal psychosocial distress in Indigenous women and its management at primary health care centres in Australia. General Hospital Psychiatry 37(4): 335–9. DOI: 10.1016/j.genhosppsych.2015.04.005.
Gayaa Dhuwi (Proud Spirit) Australia (n.d.). Aboriginal and Torres Strait Islander Leadership in social and emotional wellbeing, mental health and suicide prevention. https://www.gayaadhuwi.org.au/.
Gee, G., P. Dudgeon, C. Schultz, A. Hart and K. Kelly (2014). Aboriginal and Torres Strait Islander social and emotional wellbeing. In P. Dudgeon, H. Milroy and R. Walker, eds. Working together: Aboriginal and Torres Strait Islander health and wellbeing principles and practice, 2nd edn, 55–68. Canberra: Australian Council for Education Research and Telethon Institute for Child Health Research, Office for Aboriginal and Torres Strait Islander Health, Department of Health and Ageing.
Getting it Right Collaborative Group, M. Hackett, A. Teixeira-Pinto, S. Farnbach, N. Glozier, T. Skinner et al. (2019). Getting it right: validating a culturally specific screening tool for depression (aPHQ- 9) in Aboriginal and Torres Strait Islander Australians. Medical Journal of Australia 211(1): 24–30. DOI: 10.5694/mja2.50212.
Haswell-Elkins, M., E. Hunter, T. Nagel, C. Thompson, B. Hall, R. Mills et al. (2005). Reflections on integrating mental health into primary health care services in remote Indigenous communities in Far North Queensland and the Northern Territory. Australian Journal of Primary Health 11(2): 62–9. DOI: 10.1071/PY05023.
Haswell-Elkins, M., E. Hunter, R. Wargent, B. Hall, C. O’Higgins and R. West (2009). Protocols for the delivery of social and emotional well being and mental health services in Indigenous communities: guidelines for health workers, clinicians, consumers and carers. Cairns: Queensland Health.
Janca, A., Z. Lyons, S. Balaratnasingam, D. Parfitt, S. Davison and J. Laugharne (2015). Here and Now Aboriginal Assessment: background, development and preliminary evaluation of a culturally appropriate screening tool. Australasian Psychiatry 23(3): 287–92. DOI: 10.1177/1039856215584514.
Kwan, B. and D. Nease (2013). The state of the evidence for integrated behavioral health in primary care. In M.R. Talen and A. Burke Valeras, eds. Integrated behavioral health in primary care: evaluating the evidence, identifying the essentials, 65–98. New York: Springer New York. DOI: 10.1007/978-1-4614-6889-9_5.
Langham, E., J. McCalman, V. Matthews, R. Bainbridge, B. Nattabi, I. Kinchin et al. (2017). Social and emotional wellbeing screening for Aboriginal and Torres Strait Islanders within primary health care: a series of missed opportunities? Frontiers in Public Health 5(159). DOI: 10.3389/fpubh.2017.00159.
Leung, S., N. Brennan, T. Freeburn, W. Waugh and R. Christie (2022). Youth survey report 2022. Sydney: Mission Australia.
Martin, M., B. Potter, A. Crocker, G. Wells and I. Colman (2016). Yield and efficiency of mental health screening: a comparison of screening protocols at intake to prison. PLOS One 11(5): e0154106–e06. DOI: 10.1371/journal.pone.0154106.
Mathers, C. and D. Loncar (2006). Projections of global mortality and burden of disease from 2002 to 2030. PLOS Medicine 3(11): e442. DOI: 10.1371/journal.pmed.0030442.
Matthews, V., J. Bailie, A. Laycock, T. Nagel and R. Bailie (2016). Priority evidence – practice gaps in Aboriginal and Torres Strait Islander mental health and wellbeing care: final report. ESP Project. Brisbane: Menzies School of Health Research.
McCalman, J., R. Bainbridge and T. Benveniste (2019). The use and satisfaction with health care services of Aboriginal and Torres Strait Islander students at boarding schools: baseline results. International Journal of Integrated Care 19(S1): A435 1–8. DOI: 10.5334/ijic.s3435.
McCalman, J., R. Bainbridge, C. Brown, K. Tsey and A. Clarke (2018). The Aboriginal Australian Family Wellbeing Program: a historical analysis of the conditions that enabled its spread. Frontiers in Public Health 6: 26. DOI: 10.3389/fpubh.2018.00026.
McCalman, J., R. Bainbridge, Y. Cadet-James, R. Bailie, K. Tsey, V. Matthews et al. (2020). Systems integration to promote the mental health of Aboriginal and Torres Strait Islander children: protocol for a community-driven continuous quality improvement approach. BMC Public Health 20(1): 1810. DOI: 10.1186/s12889-020-09885-x.
McCalman, J., E. Langham, T. Benveniste, M. Wenitong, K. Rutherford, A. Britton et al. (2020). Integrating health care services for Indigenous Australian students at boarding schools: a mixed-methods sequential explanatory study. International Journal of Integrated Care 20(1): 8. DOI: 10.5334/ijic.4669.
McGorry, P., T. Bates and M. Birchwood (2013). Designing youth mental health services for the 21st century: examples from Australia, Ireland and the UK. British Journal of Psychiatry 202(s54): s30–s35. DOI: 10.1192/bjp.bp.112.119214.
McGorry, P., R. Purcell, I. Hickie and A. Jorm (2007). Investing in youth mental health is a best buy. Medical Journal of Australia 187(7). DOI: 10.5694/j.1326-5377.2007.tb01326.x.
Menzies School of Health Research (2014). Mental health clinical audit tool. One21seventy. Darwin: Menzies School of Health Research. https://www.menzies.edu.au/page/Resources/Mental_Health_clinical_audit/
Menzies School of Health Research and One21seventy (2012). Systems assessment tool – all client groups. Darwin: Menzies School of Health Research. https://www.menzies.edu.au/page/Resources/Systems_Assessment_Tool_SAT/
National Aboriginal Community Controlled Health Organisation and Royal Australian College of General Practitioners (2024). National guide to a preventative health assessment for Aboriginal and Torres Strait Islander people, 4th edn. Melbourne: RACGP.
Ngo, V., A. Rubinstein, V. Ganju, P. Kanellis, N. Loza, C. Rabadan-Diehl et al. (2013). Grand challenges: integrating mental health care into the non-communicable disease agenda. PLOS Medicine 10(5): e1001443. DOI: 10.1371/journal.pmed.1001443.
Ngo, V.K., J.R. Asarnow, J. Lange, L.H. Jaycox, M.M. Rea and C. Landon (2009). Outcomes for youths from racial-ethnic minority groups in a quality improvement intervention for depression treatment. Psychiatric Services 60(10): 1357–64. DOI: 10.1176/ps.2009.60.10.1357.
Nguyen, T., T. Tran, H. Tran, T.D. Tran and J. Fisher (2021). Challenges in integrating mental health into primary care in Vietnam. In S. Okpaku, ed. Innovations in global mental health, 1249–69. Switzerland: Springer International Publishing. DOI: 10.1007/978-3-030-57296-9_74.
Paradies, Y., J. Ben, N. Denson, A. Elias, N. Priest, A. Pieterse et al. (2015). Racism as a determinant of health: a systematic review and meta-analysis. PLOS One 10(9): e0138511. DOI: 10.1371/journal.pone.0138511.
Patel, V., R. Araya, S. Chatterjee, D. Chisholm, A. Cohen, M. De Silva et al. (2007). Treatment and prevention of mental disorders in low-income and middle-income countries. Lancet 370(9591): 991–1005. DOI: 10.1016/s0140-6736(07)61240-9.
Prince, J., N. Jeffrey, L. Baird, S. Kingsburra and B. Tipiloura (2018). Stories from community: how suicide rates fell in two Indigenous communities. Canberra: Healing Foundation.
Rehm, J. and K. Shield (2019). Global burden of disease and the impact of mental and addictive disorders. Current Psychiatry Reports 21(2): 10. DOI: 10.1007/s11920-019-0997-0.
Schierhout, G., T. Nagel, D. Si, C. Connors, A. Brown and R. Bailie (2013). Do competing demands of physical illness in type 2 diabetes influence depression screening, documentation and management in primary care: a cross-sectional analytic study in Aboriginal and Torres Strait Islander primary health care settings. International Journal of Mental Health Systems 7(1): 16. DOI: 10.1186/1752-4458-7-16.
Si, D., M. Dowden, C. Kennedy, R. Cox, L. O’Donoghue, H. Liddle et al. (2011). Indigenous community care: documented depression in patients with diabetes. Australian Family Physician 40(5): 331–3.
Wang, P., S. Aguilar-Gaxiola, J. Alonso, M. Angermeyer, G. Borges, E. Bromet et al. (2007). Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. Lancet 370(9590): 841–50. DOI: 10.1016/S0140-6736(07)61414-7.
WellMob: healing our way (n.d.). Social, emotional and cultural wellbeing online resources for Aboriginal and Torres Strait Islander People. https://wellmob.org.au.
WHO and Wonca (2008). Integrating mental health into primary care: a global perspective. Geneva: World Health Organization and World Organization of Family Doctors (Wonca).
Woolf, S.H. and R. Harris (2012). The harms of screening: new attention to an old concern. JAMA : The Journal of the American Medical Association 307(6): 565–6. DOI: 10.1001/jama.2012.100.
World Health Organization (2019). The WHO special initiative for mental health (2019–2023): universal health coverage for mental health. Geneva, Switzerland: World Health Organization. https://apps.who.int/iris/handle/10665/310981.
World Health Organization (2018). Mental health: strengthening our response. Key facts. Geneva, Switzerland: World Health Organization.
Yin, X., N. Sun, N. Jiang, X. Xu, Y. Gan, J. Zhang et al. (2021). Prevalence and associated factors of antenatal depression: systematic reviews and meta-analyses. Clinical Psychology Review F83(101932). DOI: 10.1016/j.cpr.2020.101932.
1 World Health Organization 2018, 1.
2 Rehm and Shield 2019.
3 Australian Institute of Health and Welfare 2022b.
4 McGorry, Purcell et al. 2007.
5 Mathers and Loncar 2006.
6 Ngo, Rubinstein et al. 2013.
7 Yin, Sun et al. 2021.
8 Wang, Aguilar-Gaxiola et al. 2007; World Health Organization 2019.
9 Drake, Binagwaho et al. 2014.
10 Ngo, Asarnow et al. 2009; World Health Organization 2019.
11 Kwan and Nease 2013; WHO and Wonca 2008.
12 WHO and Wonca 2008.
13 Drake, Binagwaho et al. 2014; Ngo, Rubinstein et al. 2013.
14 WHO and Wonca 2008.
15 Funk, Wutzke et al. 2005; Patel, Araya et al. 2007.
16 Haswell-Elkins, Hunter et al. 2005; Nguyen, Tran et al. 2021.
17 Ngo, Rubinstein et al. 2013.
18 WHO and Wonca 2008.
19 Gee, Dudgeon et al. 2014.
20 Gee, Dudgeon et al. 2014, 58.
21 Gee, Dudgeon et al. 2014.
22 Dudgeon, Milroy and Walker 2014; Gee, Dudgeon et al. 2014.
23 Commonwealth of Australia 2017; Dudgeon, Milroy and Walker 2014; Paradies, Ben et al. 2015.
24 Dudgeon, Bray et al. 2020.
25 Australian Institute of Health and Welfare 2016.
26 Australian Bureau of Statistics 2019.
27 Australian Institute of Health and Welfare 2022b; Commonwealth of Australia 2017; Dudgeon, Milroy and Walker 2014.
28 Leung, Brennan et al. 2022.
29 McGorry, Bates and Birchwood 2013.
30 Department of Health 2017.
31 Dudgeon, Bray et al. 2017.
32 Prince, Jeffrey et al. 2018.
33 McCalman, Bainbridge et al. 2018.
34 Gee, Dudgeon et al. 2014.
35 Menzies School of Health Research 2014.
36 Menzies School of Health Research and One21seventy 2012.
37 Matthews, J. Bailie et al. 2016.
38 Matthews, J. Bailie et al. 2016.
39 Matthews, J. Bailie et al. 2016.
40 Matthews, J. Bailie et al. 2016.
41 Matthews, J. Bailie et al. 2016.
42 Menzies School of Health Research and One21seventy 2012.
43 Matthews, J. Bailie et al. 2016.
44 Langham, McCalman et al. 2017.
45 Schierhout, Nagel et al. 2013.
46 Si, Dowden et al. 2011.
47 Gausia, Thompson et al. 2013.
48 Gausia, Thompson et al. 2015.
49 Gausia, Thompson et al. 2015.
50 Edmond, McAuley et al. 2018.
51 Getting it Right Collaborative Group, Hackett et al. 2019.
52 Commonwealth of Australia 2017.
53 WHO and Wonca 2008; Davis, Balasubramanian et al. 2013.
54 Edmond, McAuley et al. 2018; Gausia, Thompson et al. 2015; Langham, McCalman et al. 2017; Schierhout, Nagel et al. 2013.
55 McCalman, Bainbridge et al. 2020.
56 Anaf, Baum et al. 2014; Edmond, McAuley et al. 2018.
57 Gee, Dudgeon et al. 2014.
58 Matthews, J. Bailie et al. 2016.
59 Janca, Lyons et al. 2015.
60 Beyondblue 2013.
61 Getting it Right Collaborative Group, Hackett et al. 2019.
62 National Aboriginal Community Controlled Health Organisation and Royal Australian College 2024.
63 Martin, Potter et al. 2016; Woolf and Harris 2012.
64 Langham, McCalman et al. 2017.
65 Dobrow, Sullivan et al. 2018.
66 Haswell-Elkins, Hunter et al. 2009.
67 WellMob. n.d. https://wellmob.org.au/.
68 Australian Indigenous HealthInfoNet. n.d. https://healthinfonet.ecu.edu.au/.
69 Gayaa Dhuwi (Proud Spirit) Australia. n.d. https://www.gayaadhuwi.org.au/.
70 Langham, McCalman et al. 2017.
71 Carson, Dunbar et al. 2007; McCalman, Langham et al. 2020.
72 McCalman, Bainbridge and Benveniste 2019.
73 McCalman, Langham et al. 2020, 11.
74 McCalman, Bainbridge et al. 2020.