8
Embedding a culture of CQI
The final chapter in Part II builds on the content of the previous chapters to discuss what is meant by a culture of CQI, and how to embed and sustain such a culture. We begin by considering the concept of organisational culture, and how it translates into a quality culture in PHC services. The chapter then discusses leadership for CQI and team building for change management. We draw attention to some tools that can be used to promote understanding of the current culture of your PHC service and organisation and what to think about when selecting an appropriate tool for this purpose.
What is organisational culture in health care?
“Organisational culture” is defined as the shared values, beliefs and norms of an organisation that shape members’ attitudes, feelings and behaviours – or the way things are done.1 In healthcare organisations, it represents the shared ways of thinking, feeling and behaving. Poor organisational culture is often blamed for failures in service delivery, and the need for culture change is frequently suggested as a remedy for improving performance.2
There are many theories relating to organisational culture and two distinct views. One view sees culture as something an organisation “has”: a characteristic that can be assessed and then adjusted as required around an aspect of organisational culture, such as “client-centredness”. The other view sees culture as something that cannot be separated from the organisation itself: something that just “is”. This view prompts reflection, learning and action but is less optimistic about the potential to bring about cultural change within an organisation.3
In Edgar Schein’s commonly used definition, organisational culture is discovered or developed as a group adapts to the external environment, and to the way its internal structures function.4 Schein described three layers of organisational culture: artefacts and rituals (aspects of culture that are visible); adopted values (shared ways of thinking); and the shared assumptions that underpin them. Box 8.1 offers examples relevant to PHC. Together, the layers form the culture of an organisation.
Box 8.1 Three layers of organisational culture
Artefacts and rituals (what’s visible) – such as how the health service is structured, how facilities are designed, role boundaries, care pathways, rules and procedures, reward systems and dress codes. Artefacts may include how CQI is implemented and how safety risks and complaints are managed.
Adopted values (shared ways of thinking) – such as the service’s or practice’s mission and strategic goals. These values provide the rationale for what is visible and may reflect prevailing views on client needs and autonomy, the type of evidence that influences decision-making, and expectations about quality and service performance.
Shared assumptions – are tacit beliefs that are “taken for granted” and which underpin values, decision-making and day-to-day practice. Examples might be assumptions about levels of health literacy among clients, or about which professional group holds most power in the health service. Understanding these “hidden” assumptions is crucial for understanding the culture of an organisation.5
Organisational culture matters, because it influences what matters to the organisation, how people work together, attitudes towards change, and how the organisation learns and uses new knowledge. It influences service outcomes. A recent review of international evidence found a consistent link between positive organisational culture and positive client outcomes across multiple studies, settings and countries.6
Team culture also matters, because teams can form subcultures within the organisation that influence the quality of care provided. In addition, teams need to work with other teams in a PHC service rather than as “siloed” work units to deliver high-quality client-centred care. A PHC team may be a driving force for quality improvement or may undermine continuous quality improvement activities. It is not surprising that ideas of organisational and team culture are central to quality improvement.
The look and feel of a continuous quality improvement culture
Organisations and teams with a strong improvement culture promote CQI as an everyday whole-of-organisation process and continually strive for learning and improvement. There is a “vision” of providing better care, shared thinking and an underlying assumption that investing time and effort in CQI pays off in better systems of care, in working smarter not harder, and in better outcomes for clients. An early United States study linked the implementation of CQI with a participative, flexible and risk-taking organisational culture.7 Risk-taking in this context does not imply risking client safety, but means being prepared to innovate systems of care: to shift the status quo. The study, which involved 61 hospitals, found that more bureaucratic and hierarchical cultures were a barrier to implementing CQI, while cultures that fostered openness, collaboration, teamwork and learning led to more successful improvement initiatives with lasting effect.8 These findings reflect current thinking about organisational culture and CQI.
While every PHC practice, service or health organisation is different, some common features have been identified in organisations with a strong CQI culture:
- leadership for continuous quality improvement at all levels
- boards, senior and middle managers share the same vision and goals for continuous quality improvement
- continuous quality improvement links with the strategic plan, policies, other reporting and performance frameworks
- devolved decision-making
- open communication across the organisation
- teamwork and diversity are valued
- safe to make mistakes
- focus on outcomes not just processes
- strong external links – working with other organisations
- strong community engagement
- staff and management open to change and new ideas
- improvement strategies are in place
- continuous quality improvement is routine
- active management of continuous quality improvement (for example, a continuous quality improvement facilitator role)
- continuous quality improvement training available for all managers and staff.
These features work together to create a culture of CQI.
In Chapter 7, we referred to work undertaken by Larkins, Turner and colleagues to identify features of Aboriginal and Torres Strait Islander PHC services that had demonstrated significant improvement in the quality of care. The researchers found that health services with a strong CQI culture had many features identified in international studies (such as those listed above). But these services also had some novel features specific to Aboriginal and Torres Strait Islander PHC:
- The services took account of the historical and cultural context of the community in the way they worked. Trusting and respectful relationships were developed between staff and clients.
- There was “two-way” learning, integrating cultural knowledge and knowledge of clinical care.
- Staff were caring. They were seen to go the extra mile for their clients.
- Communities were actively driving health improvement.9
As shown in Figure 8.1, the common and novel features operated at different levels:
- micro-system level – interactions between individual clients and staff (caring staff, clients and community members engaged with PHC service)
- meso-system level – within the health service (health service CQI supports, teamwork and collaboration, prepared workforce, two-way learning)
- macro-system level – in the broader context (linkages and partnerships with external organisations, understanding and responding to historical and cultural contexts, health service external policies, communities driving health improvement).
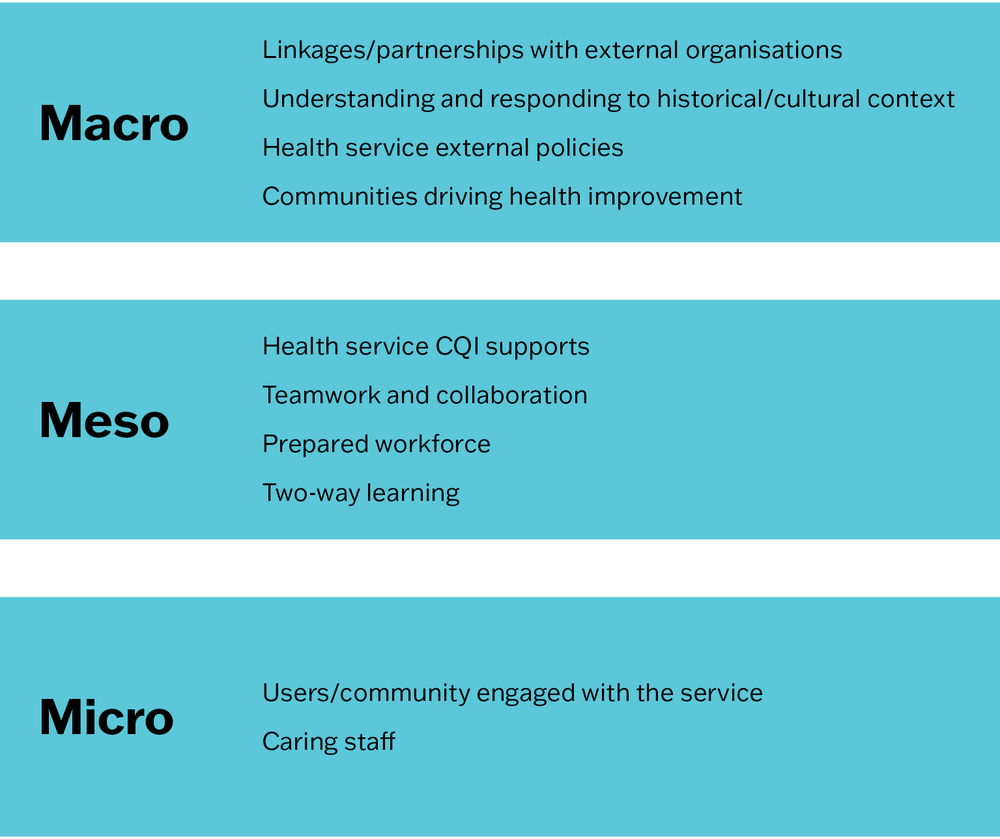
Figure 8.1 Factors influencing quality improvement at high-improving Aboriginal and Torres Strait Islander PHC services (Carlisle, Matthews et al. 2021).
Continued research by the group has highlighted the significance of PHC teams and communities having a shared purpose around improving the health of the community.10 We see these features as evidence of a strong CQI culture in Aboriginal and Torres Strait Islander PHC contexts. A culture of CQI may have unique features in other PHC contexts. It is important to be open to difference and avoid taking a one-size-fits-all approach when evaluating the CQI culture in your PHC setting.
Embedding and sustaining the culture
A literature review by Willis and colleagues identified six guiding principles for sustaining cultural change in health systems: align vision and action; make incremental changes; foster distributed leadership across the organisation; promote staff engagement; create collaborative relationships; and continuously assess and learn from change.11 The principles are strikingly similar to principles for guiding CQI, supporting the evidence that continuously implementing CQI helps to embed and sustain a CQI culture. The skills and knowledge needed to put these shared principles into practice include:
- skills in quality improvement and change management
- skills in leadership, team building and collaboration
- an understanding of the current organisational culture and context of the organization
- the ability to engage clients and families or communities in CQI, so that improvement interventions can be tailored to local needs.12
We presented tools and strategies for developing CQI skills, and for engaging clients and communities in CQI in the previous chapters. We focus here on leadership for CQI, team building for change management, and understanding the current culture of an organisation.
Leadership
Leadership for CQI is essentially about leading change. Capable and passionate leaders can inspire others by setting out a vision for change, engaging others in improvement activities, leading implementation and demonstrating outcomes that align with staff or community priorities for improving care. Leadership for CQI can come from people in different roles and at different levels of a service or PHC support organisation. It can be formal or informal, strategic, operational or clinical.13 A “distributed leadership” approach, built on a foundation of good relationships, has been linked to improvements in service outcomes.14
Leadership for CQI is about leading change.
When people are engaged in CQI, they are more likely to understand and trust data, to work as a team and to see their CQI efforts result in better care outcomes for clients and communities. This in turn creates positive attitudes towards change and willingness to participate in CQI activities.15 And when more people adopt a CQI way of thinking, it more quickly becomes the way things are done.
A CQI approach can, in turn, be applied in leadership development programs. A case study with health service managers from geographically remote settings found that workplace-based action learning projects for continuous quality improvement provided managers with opportunities to apply their learning. The context-specific application of skills helped in understanding real-world competence. CQI based learning projects can also potentially produce the type of data needed for evaluating program impact and lead to better client outcomes.16
Tips for CQI leadership in PHC
We offer tips for PHC leaders about how to embed and sustain an organisational culture of CQI. Key messages from our experience are reinforced by international literature.
- Develop your skills and capabilities for CQI.
- Share responsibility for quality improvement with leaders at different levels and work together. Work to your individual strengths (for example, in communication, negotiation, finance, or community engagement) to collaboratively lead improvement.
- Take responsibility for strengthening poor systems that result in poor-quality processes or outcomes. Advocate and collaborate with senior managers and policymakers to develop solutions and embed system changes.
- Be prepared to invest time and resources into implementing CQI. Work to maintain staff engagement. Enable staff training in CQI and provide support for leadership development. Create time for teams to engage in CQI processes.17
- Use data effectively. Make a clear distinction between collecting data for accountability purposes and using data for learning and improvement.18
- Work to create a “no blame, no shame” culture that fosters respect, measurement and learning. It is natural for people to fear that their performance will be judged negatively, possibly with personal consequences, when gaps are identified in care quality. Have strategies for overcoming resistance to change and getting staff involved in change processes.19
- Actively engage teams in CQI. Aim for input and engagement in all phases of the CQI cycle and encourage innovation. Tap into staff motivation; celebrate small and large successes; build on what is working well.
- Involve clients, carers and communities in co-producing change. Be open to different, context-specific ways of thinking about and implementing CQI.20
- Have a systematic, coherent approach to CQI and commit for the long term. Remember: improvement is usually made in small increments over continuous CQI cycles. There are no quick fixes.21
- Identify and work with champions of change, both in the PHC service and the community.
Team building for change management
Competent leadership is essential, but successful and sustainable CQI also requires capable teams.22 Building a capable, well-prepared PHC team is a key leadership function. It begins with identifying the skills and knowledge needed across the team, recruiting the right people and properly orienting new staff (for example, to the organisation, job, team, population, context). Those who join a PHC team need these supports:
- a shared sense of purpose
- clear roles and responsibilities
- understanding of each other’s roles
- a safe workplace with open lines of communication.
Successful and sustainable CQI requires capable teams.
Workplace systems need to be designed to support teamwork and coordinated care, and team members need to feel confident in using the systems. Opportunities to do training and professional development as a team, or to share new learning with other team members, also build a sense of teamwork. Training needs to be matched to the team, the nature of the PHC work and the context. Examples might include cross-cultural competency training for cross-cultural teams and for teams working with people from cultural backgrounds other than their own, and training in mental health first aid or trauma-informed care.
As stated above, staff who are actively engaged in CQI are more likely to work as a team. The use of participatory CQI processes – including some of the group techniques described in Chapter 7 – can act as an effective team-building strategy.
“Probably the most powerful aspect of continuous quality improvement is that opportunity to reflect, and particularly if you can reflect with your team. It helps to strengthen the understanding between the team members, strengthen the knowledge and skill set between the team members, and strengthen the cohesiveness of the team.”
– Dr Christine Connors, executive director, Population and Primary Health Care, Top End Health Services Northern Territory23
Online resources and expert services are available for team building. They should be selected based on organisational and team needs, and available resources.
Understanding the current organisational culture
Some understanding of the current organisational culture is important for facilitating and evaluating cultural change. Specific tools have been developed for measuring organisational culture in health care.24 Some of these tools are categorised as CQI tools. A systems assessment tool, for example, measures aspects of organisational culture and can measure a shift when use is repeated over time (for example, improvement in teamwork or links with the community). Quantitative tools for assessing organisational culture tend to cover the visible dimensions of culture (Schein’s “artefacts and rituals”), such as leadership, teamwork, training, organisational structures and processes. Qualitative and mixed-methods tools cover both visible dimensions and those that are less tangible, such as trust, commitment, power, blame and support for each other.25
These tools can provide a general picture of organisational culture, but they may have limitations for understanding the underlying causes and dimensions of organisational culture and for identifying the nuanced strategies needed to bring about or sustain change.26 Questions have also been raised about whether tools developed for assessing organisational culture in, for example, Western settings, are transferable to non-Western settings.
Other tools worth considering are critical reflection tools that encourage staff to reflect on shared values and beliefs. Evaluation approaches, such as principles-focused evaluation, can be used to explore members’ and clients’ views on how well an organisation adheres to its espoused principles and values.27 Evaluation tools designed to stimulate thinking about program or service success in specific settings (such as Indigenous health services) may help alleviate concerns about the transferability of tools. The selection of a suitable tool for assessing the organisational culture of an organisation will be based on the purpose of the assessment and how you intend to use the findings, the healthcare setting (for example, community controlled service, private practice) and the resources available. An understanding of the current organisational culture will often develop as CQI processes are implemented.
Example: embedding a CQI culture in a PHC service
A large, well-established metropolitan PHC service was experienced in using CQI, but management was concerned that the organisation’s approach to quality improvement was stop-start, rather than continuous, and that this had prevented CQI from gaining real traction. Some staff had a low level of awareness of CQI and their potential role in improving systems of care. The management team identified the need for CQI to be considered within the context of the business of the whole organisation. They identified the need for a CQI framework that would guide quality improvement work across the service.
The Quality, Safety and Reporting team took the lead to develop the strategy. First, they reviewed literature on quality and quality improvement, focusing on literature relating to their client population (Aboriginal and Torres Strait Islander peoples). The team then held a series of face-to-face meetings with staff and managers (at senior and team levels), and the executive team, to develop a draft framework for their review. This process reinforced the role of managers in leading and supporting CQI initiatives within their teams.
Developing the framework enabled the health service to articulate the organisation’s understanding, commitment and approach to CQI. The finalised framework aimed to:
- guide employees, and particularly managers, in a systematic approach to improving organisational and service-delivery level systems, processes and outcomes
- provide information to support orientation, induction and training activities that enable everyone to contribute towards continually improving the delivery of quality services.
“Defining QI [quality improvement] roles and responsibilities was one of the most important pieces of work we achieved. This was a gap identified early on, which prevented successful CQI from occurring more often . . . We have embedded [our health centre’s] approach to CQI in the broader context of organisational performance management, quality management and clinical and practice governance” – executive manager28
Lesson learnt
Strategies must include the whole of the organisation and connect activity to broad organisational aims and goals to be sustainable and successful.
The following example describes an approach to Covid-19 testing and management in a PHC service with an embedded culture of CQI.
Example: applying CQI in a Covid-19 response
The PHC service in the remote island community of Galiwin’ku in Australia’s Northern Territory serves a population of approximately 3,000 mostly Aboriginal residents. Comprehensive PHC is delivered by Northern Territory Health and is provided by a multidisciplinary team including resident staff and fly-in, fly-out health professionals. Seriously ill residents are evacuated by air to hospital. Policy support and funding for CQI has been provided for more than a decade.
The PHC team drew on their CQI experience to develop a Covid-19 surge response plan. The plan was developed collaboratively with information systems and public health teams and was designed to scale up in the event of a surge in Covid-19 cases in the community. It includes a vaccination program, detailed Covid-19 screening, treatment and management protocols, and a standardised approach for recording and entering client data into a centralised client information system. All staff undertook training before using the client information system. Five community members were trained in rapid antigen testing (RAT), data entry and tasks considered essential for community engagement.
The PHC clinic offers walk-in and in-home RATs with culturally appropriate hand-outs about testing and managing Covid-19. Community residents are encouraged to do the testing at the clinic, where red and green zones are set up according to people’s known exposure to Covid-19, and where client data (name, contact details, number of people living in the house, age, RAT results) can be recorded immediately in the client information system. A recall list is printed each day and is used to guide home assessments for reviewing medium- and high-risk Covid-19 positive clients. Review data are entered into the system for triage, treatment planning and recall. Acutely unwell people are transferred to a larger clinic in the regional town.
CQI processes were built into the plan, including these features:
- monitoring the procedures used for administering RATs with residents (red and green zones in the clinic, home testing) to ensure processes are effective, timely and acceptable
- trialling a system for recording the data from positive RATs and home assessments each day, with attention to data quality and confidentiality
- daily checking of data reports and recall lists to ensure data are accurately captured and clients are appropriately triaged
- getting feedback from clients about their experiences and care priorities (for example, the need for community-based treatment options)
- refining community information processes, Covid-19 testing and management, data entry and data reporting to improve health service systems for responding to Covid-19.
– Amanda Robinson, medical practitioner, Dani Jordan, CQI facilitator, Shawn Cartwright, occupational therapist, Mark Ramjan, nurse/midwife education and research consultant, Northern Territory Health, Northern Territory.
Summary
The final chapter in Part II has explored the concept of organisational culture, with a focus on embedding and sustaining a culture of CQI in PHC services. A positive culture of CQI enables evidence to be used effectively for improving care. It supports the use of CQI tools and techniques into routine care and the effective facilitation of CQI. To this end, we have briefly discussed leadership for CQI, team building for change management and offered tips for leaders. Tools for understanding the current culture of an organisation have been suggested and examples of an embedded CQI culture have been included. It is important to remember that implementing CQI cycles can help to gradually shift organisational or team culture in a positive direction as changes to systems and processes are collaboratively developed, tested, evaluated and adopted.
“CQI is everybody’s business” is a widely used motto in Aboriginal and Torres Strait Islander PHC. It embraces the concept of a CQI culture, reinforcing the message that all people who work or access health services have a voice and a role in improving high-quality care.
References
Bailie, J., A. Laycock, K. Conte, V. Matthews, D. Peiris, R. Bailie et al. (2021). Principles guiding ethical research in a collaboration to strengthen Indigenous primary healthcare in Australia: learning from experience. BMJ Global Health 6(1): e003852. DOI: 10.1136/bmjgh-2020-003852.
Best, A., T. Greenhalgh, S. Lewis, J. Saul, S. Carroll and J. Bitz (2012). Large-system transformation in health care: a realist review. Milbank Quarterly 90(3): 421–56. DOI: 10.1111/j.1468-0009.2012.00670.x.
Braithwaite, J., J. Herkes, K. Ludlow, L. Testa and G. Lamprell (2017). Association between organisational and workplace cultures, and patient outcomes: systematic review. BMJ Open 7(11): e017708. DOI: 10.1136/bmjopen-2017-017708.
Carlisle, K., V. Matthews, M. Redman-MacLaren, K. Vine, N. Turner, C. Felton-Busch et al. (2021). A qualitative exploration of priorities for quality improvement amongst Aboriginal and Torres Strait Islander primary health care services. BMC Health Services Research 21(1): 431. DOI: 10.1186/s12913-021-06383-7.
Davies, H., S. Nutley and R. Mannion (2000). Organisational culture and quality of health care. Quality in Health Care 9: 111–19. DOI: 10.1136/qhc.9.2.111.
Davis, M., E. Mahanna, B. Joly, M. Zelek, W. Riley, P. Verma et al. (2014). Creating quality improvement culture in public health agencies. American Journal of Public Health 104(1): e98–e104. DOI: 10.2105/AJPH.2013.301413.
Fitzgerald, L., E. Ferlie, G. McGivern and D. Buchanan (2013). Distributed leadership patterns and service improvement: evidence and argument from English healthcare. Leadership Quarterly 24(1): 227–39. DOI: 10.1016/j.leaqua.2012.10.012.
Gardner, K., M. Dowden, S. Togni and R. Bailie (2010). Understanding uptake of continuous quality improvement in Indigenous primary health care: lessons from a multi-site case study of the Audit and Best Practice for Chronic Disease project. Implementation Science 5: 21. DOI: 10.1186/1748-5908-5-21.
Hart, C., C. Dykes, R. Thienprayoon and J. Schmit (2015). Change management in quality improvement: the softer skills. Current Treatment Options in Pediatrics 1(4): 372–9. DOI: 10.1007/s40746-015-0028-2.
King’s Fund (2017). Making the case for quality improvement: lessons for NHS boards and leaders. https://www.kingsfund.org.uk/publications/making-case-quality-improvement#what-should-nhs-leaders-do-.
Larkins, S., K. Carlisle, N. Turner, J. Taylor, K. Copley, S. Cooney et al. (2019). “At the grass roots level it’s about sitting down and talking”: exploring quality improvement through case studies with high-improving Aboriginal and Torres Strait Islander primary healthcare services. BMJ Open 9(5): e027568. DOI: 10.1136/bmjopen-2018-027568.
Malik, R., M. Buljac-Samardžić, N. Akdemir, C. Hilders and F. Scheele (2020). What do we really assess with organisational culture tools in healthcare? An interpretive systematic umbrella review of tools in healthcare. BMJ Open Quality 9(1): e000826. DOI: 10.1136/bmjoq-2019-000826.
Mannion, R. and H. Davies (2018). Understanding organisational culture for healthcare quality improvement. BMJ 363: k4907. DOI: 10.1136/bmj.k4907.
Newham, J. and F. Cunningham (2015). Continuous quality improvement success stories: identifying effective strategies for CQI in Aboriginal and Torres Strait Islander primary health care – study report. ABCD National Research Partnership. Brisbane: ABCD National Research Partnership, Menzies School of Health Research.
Northern Territory Remote Locum Program and Aboriginal Medical Services Alliance of the Northern Territory (AMSANT) (n.d.). Continuous Quality Improvement in the NT. eLearning module. https://www.rahc.com.au/elearning-resources/elearning.
Onnis, L., M. Hakendorf, M. Diamond and K. Tsey (2019). CQI approaches for evaluating management development programs: a case study with health service managers from geographically remote settings. Evaluation and Program Planning 74: 91–101. DOI: 10.1016/j.evalprogplan.2019.03.003.
Øvretveit, J. (2009). Evidence: leading improvement effectively. London: Health Foundation.
Redman-MacLaren, M., N. Turner, J. Taylor, A. Laycock, K. Vine, Q. Thompson et al. (2021). Respect is central: a critical review of implementation frameworks for continuous quality improvement in Aboriginal and Torres Strait Islander primary health care services. Frontiers in Public Health
16: 9. DOI: 10.3389/fpubh.2021.630611.
Riley, W., H. Parsons, G. Duffy, J. Moran and B. Henry (2010). Realizing transformational change through quality improvement in public health. Journal of Public Health Management Practice 16(1): 72–8. DOI: 10.1097/PHH.0b013e3181c2c7e0.
Schein, E. (2010). Organizational culture and leadership. San Francisco, CA: Jossey-Bass.
Schierhout, G., J. Hains, D. Si, C. Kennedy, R. Cox, R. Kwedza et al. (2013). Evaluating the effectiveness of a multifaceted, multilevel continuous quality improvement program in primary health care: developing a realist theory of change. Implementation Science 8: 119. DOI: 10.1186/1748-5908-8-119.
Scott, T., R. Mannion, H. Davies and M. Marshall (2003). The quantitative measurement of organizational culture in health care: a review of the available instruments. Health Services Research 38(3): 923–45. DOI: 10.1111/1475-6773.00154.
Shojania, K. and J. Grimshaw (2005). Evidence-based quality improvement: the state of the science. Health Affairs 24(1): 138–50. DOI: 10.1377/hlthaff.24.1.138.
Shortell, S., J. O’Brien, J. Carman, R. Foster, E. Hughes, H. Boerstler et al. (1995). Assessing the impact of continuous quality improvement/total quality management: concept versus implementation. Health Services Research 30(2): 377–401. https://pubmed.ncbi.nlm.nih.gov/7782222.
Simpson, D., S. Hamilton, R. McSherry and R. McIntosh (2019). Measuring and assessing healthcare organisational culture in the England’s National Health Service: a snapshot of current tools and tool use. Healthcare 7(4): 127. DOI: 10.3390/healthcare7040127.
Sollecito, W. and J. Johnson (2019). McLaughlin and Kaluzny’s continuous quality improvement in health care. Burlington, MA: Jones & Bartlett Learning.
Turner, N., J. Taylor, S. Larkins, K. Carlisle, S. Thompson, M. Carter et al. (2019). Conceptualizing the association between community participation and CQI in Aboriginal and Torres Strait Islander PHC services. Qualitative Health Research 29(13): 1904–15. DOI: 10.1177/1049732319843107.
Wensing, M., H. Wollersheim and R. Grol (2006). Organizational interventions to implement improvements in patient care: a structured review of reviews. Implementation Science 1: 2. DOI: 10.1186/1748-5908-1-2.
Willis, C., J. Saul, H. Bevan, M. Scheirer, A. Best, T. Greenhalgh et al. (2016). Sustaining organizational culture change in health systems. Journal of Health Organization and Management 30(1): 2–30. DOI: 10.1108/JHOM-07-2014-0117.
Wise, M., S. Angus, E. Harris and S. Parker (2013). National appraisal of continuous quality improvement initiatives in Aboriginal and Torres Strait Islander primary health care: final report. Melbourne: Lowitja Institute.
1 Davies, Nutley and Mannion 2000; Shortell, O’Brien et al. 1995.
2 Malik, Buljac-Samardžić et al. 2020; Mannion and Davies 2018.
3 Mannion and Davies 2018.
4 Schein 2010.
5 Mannion and Davies 2018 (adapted).
6 Braithwaite, Herkes et al. 2017.
7 Shortell, O’Brien et al. 1995.
8 Shortell, O’Brien et al. 1995.
9 Larkins, Carlisle et al. 2019; Redman-MacLaren, Turner et al. 2021; Turner, Taylor et al. 2019.
10 Carlisle, Matthews et al. 2021.
11 Willis, Saul et al. 2016.
12 Hart, Dykes et al. 2015.
13 Øvretveit 2009.
14 Fitzgerald, Ferlie et al. 2013.
15 Gardner, Dowden et al. 2010; Riley, Parsons et al. 2010; Schierhout, Hains et al. 2013; Wise, Angus et al. 2013.
16 Onnis, Hakendorf et al. 2019.
17 King’s Fund 2017.
18 Shojania and Grimshaw 2005; Sollecito and Johnson 2019; Wensing, Wollersheim and Grol 2006.
19 Willis, Saul et al. 2016.
20 Larkins, Carlisle et al. 2019.
21 King’s Fund 2017.
22 Hart, Dykes et al. 2015.
23 Northern Territory Remote Locum Program and Aboriginal Medical Services Alliance of the Northern Territory (AMSANT) n.d.
24 Scott, Mannion et al. 2003; Simpson, Hamilton et al. 2019.
25 Malik, Buljac-Samardžić et al. 2020.
26 Malik, Buljac-Samardžić et al. 2020.
27 Bailie, Laycock et al. 2021.
28 Newham and Cunningham 2015, 15, 16.