7
Facilitating CQI
While continuous quality improvement (CQI) tools and approaches differ, a common feature is that they harness the knowledge, skills, experience and views of a range of people involved in, or affected by, care. This is the essence of CQI. It is through participation, interaction, shared decision-making and ongoing engagement in CQI cycles that improvement needs are identified, and changes are implemented and sustained. People who are actively engaged in CQI processes are generally more invested in seeing their efforts succeed. The facilitation of these processes is crucial to improving care. This chapter shares knowledge and techniques for facilitating CQI in PHC settings.
What is facilitation?
Facilitation is a technique where an individual makes things easier for others, by providing support to help them develop their thinking and ways of working.1 Put simply, it is a process of enabling groups or teams to work effectively together to achieve a common goal.2 The humanistic principles of participation, engagement, shared decision-making and enabling that underpin facilitation3 align well with the core principles of CQI.4
In health care, facilitation has been defined as the “active ingredient” that matches a proposed improvement to the individuals and teams involved and the context in which they work, thereby enabling successful implementation.5 Facilitators are agents of change.
The focus of facilitation varies according to the underpinning theory being used (for examle, change management theory, community development theory) and the aim. Facilitation may focus on empowering participants, for example, by harnessing individual strengths to challenge existing practice and find new ways of thinking and doing to improve care. A common focus of CQI facilitation is on tasks and team processes for achieving defined goals.6
Some health services employ CQI facilitators, but often CQI facilitation is done by appointed CQI leaders within PHC services or practices, or in community-based programs. In some CQI models, external facilitators provide support across a network of PHC services and practices.7 Facilitators may come from clinical or non-clinical backgrounds. Regardless of the model used, a key aim of a CQI facilitator is to drive and motivate a practice or system change and to act as a resource for making changes happen.8
Facilitation works to improve care
There is evidence that facilitation of team-based, goal-focused CQI that responds to local context can enhance the uptake of evidence-based care9 and improve health outcomes.10 International research found that PHC practices supported by facilitators are almost three times more likely to adopt evidence-based clinical guidelines.11 This should not surprise, given the complexity of implementing best-practice guidelines across the scope of clinical PHC. Further evidence of the effectiveness of facilitation comes from a large trial in Vietnam engaging women with maternal and newborn care. Groups who received support from community workers trained as quality improvement facilitators demonstrated a significant reduction in neonatal mortality after three years.12
International research found that PHC practices supported by facilitators are almost three times more likely to adopt evidence-based clinical guidelines.
Numerous factors at a local, organisational and health system level can influence the success of an improvement program. Effective facilitation is key to PHC staff making sense of data, identifying improvement goals and successfully tailoring evidence-based improvement interventions to context.13 In Indigenous Australian settings, for example, facilitation is important for adapting CQI approaches to suit PHC settings,14 and for adjusting CQI processes to respond to local needs.15
Example: embedding a CQI facilitator in a centralised support team
A study conducted across a network of eleven Aboriginal community controlled PHC services investigated barriers and enablers to implementing a CQI program. Participants in management and clinical roles identified dedicated facilitation support as a key enabler for initiating and sustaining CQI activity.
In this context, it was important for the CQI facilitation role to be embedded in a centralised team that offered integrated CQI delivery support to member services. The approach promoted a coherent and systems-based approach to planning and improvement across the organisation.16
Another study explored CQI implementation in six PHC services that had demonstrated significant improvement. Locally facilitated team meetings, community input to health service organisation, and shared decision-making contributed to CQI that responded to the sociocultural context of the service. The harnessing of collective intent and action were motivating for teams and supported the development of shared goals and improved health outcomes for service users.17
What does CQI facilitation look like?
As defined above, CQI facilitation is an enabling role, as opposed to persuading, directing or telling people what to do. A facilitator helps groups to work collaboratively to agree on areas for improvement and to create and sustain change in the way care is provided.18 Working in this way stimulates learning. It helps to embed capacity for change within healthcare or program teams by influencing workplace culture, and by empowering and upskilling team or community members, or both, to facilitate change.19 Sustainable change is more likely to result from CQI processes that actively involve a range of stakeholders in identifying improvement needs, and in planning and implementing changes.
CQI facilitation is an enabling role.
Many CQI resources refer to “quality improvement teams”. Bringing together a quality improvement team is best suited to large-scale organisations, such as hospitals, or to healthcare support organisations that serve a network of services or practices. It is not necessarily feasible to nominate a quality improvement team in a small health centre or practice, because the entire PHC team is likely to be involved in identifying improvement priorities and planning improvement strategies. When we refer to teams, we are referring to PHC or program teams.
Facilitating with PHC teams
Services with well-functioning CQI programs generally demonstrate good teamwork and collaboration, including supportive leadership for CQI. A striking feature of six high-improving PHC services studied by Larkins and colleagues was staff commitment to working together towards the same goal —improved health for their clients and their communities. Facilitators were likely to encourage teamwork through team meetings, shared decision-making and linking with CQI support networks.20
A range of strategies can be facilitated as part of a CQI process, such as these:
- educating participants in core concepts of CQI and how to use appropriate tools
- engaging staff, managers and other key stakeholders in CQI processes
- undertaking a baseline assessment that involves assessing readiness for CQI (motivation and capability); surveying the operating environment; and identifying who needs to be involved
- collecting data using CQI tools and methods (for example, undertaking an audit, surveying community perspectives)
- analysing and interpreting data, identifying improvement priorities and developing an action plan
- implementing improvement strategies, providing feedback on the activities in real time, and tracking progress
- repeating data collection to measure improvement and reflecting on CQI implementation (what worked well and less well)
- sharing results with a wider group as relevant, celebrating success, testing further changes as needed and sustaining improvement.21
The way in which the strategies are facilitated depends on the PHC context, the skills, knowledge and characteristics of the PHC team, management approaches, the focus of the improvement work and the evidence used for informing change.22 Tailoring facilitation to needs and context leads to more effective CQI.23
Tailoring facilitation to needs and context leads to more effective CQI.
Story: tailoring a CQI process to the needs of a PHC service
Experienced CQI facilitators were invited by a PHC team in a remote area to help develop an action plan to improve systems of care for clients with diabetes. It was a multidisciplinary team with resident nurses, Aboriginal health practitioners, a diabetes educator and health promotion staff, and two general practitioners who flew in and out on a weekly roster. Half the team were Aboriginal people from the community.
“We began by clarifying the quality problem. We looked at the data – how many clients had a diabetes diagnosis, HbA1c [blood glucose level] and blood pressure results and so on, and paid particular attention to trends over time. Did the data show things were improving or getting worse? We considered qualitative data. What was the feedback from the clients themselves and from the community? The large number of local Aboriginal staff made it a lot easier to understand the situation from a client perspective, as many had family members who had diabetes, or had a diagnosis themselves.
Once we had a clear picture, we spent time mapping out those things that made effective diabetes management more difficult and what the health service could do to improve their systems of care, the patient experience and hopefully improve outcomes for their clients. We used a mind mapping tool to do this. This led to a prioritising process. We discussed what could they change straight away to improve care and what could be addressed down the track.
When the team had identified their priorities for improvement, we used the plan-do-study-act (PDSA) tool to set goals, plan measurement and outline the steps they would take to make changes. The team wrote out a plan. As we all know how easy it is to write a plan and not follow through on it, people were identified to take responsibility for ensuring each part of the plan was actioned. The manager of the team also put the CQI process for diabetes on their health centre meeting agenda to ensure it didn’t get lost in the busyness of the health centre activities.”
– Kerry Copley and Louise Patel, CQI program coordinators, Aboriginal Medical Services Alliance Northern Territory.
For more information, see Aboriginal Medical Services Alliance Northern Territory n.d.
Engaging clients, families, carers and communities in CQI
Engaging clients, their families or carers, and communities in CQI is consistent with concepts of client-centred and value-based care. It signals a shift in thinking from asking “What is the matter?” to asking “What matters to you or to us (or both)?”.
Facilitation strategies for engaging clients, families/carers and communities are likely to focus on:
- working with organisational leadership to manage expectations and to clarify the expected contribution of clients and their families or carers, the resources required and potential risks and benefits
- developing mechanisms for community members and staff to share ideas, information and make joint decisions about quality improvement
- training and supporting community members to take on a community facilitator role
- engaging in genuine learning and sharing of perspectives through relationships as well as through structured learning opportunities (in some contexts, this involves building relationships with client participants through an appointed staff “partner”)
- engaging clients and carers in quality improvement sessions and encouraging them to share their lived experience and local knowledge
- reaching out to clients through focus groups, interviews, surveys or gathering stories about clients’ experiences, or a combination of these
- supporting staff to take on client input
- consulting client and community representatives on advisory committees and governing boards
- getting leadership commitment to implement suggestions or plans that come from client engagement in CQI. This may require advocacy with policy makers and funders.
Example: seeking community input about service quality
A health service providing PHC for an Indigenous community in a remote region of northern Australia held annual whole-of-community meetings to discuss the quality of care delivered. At the meetings, community members and service staff came together to share information and ideas, and to make joint decisions about quality improvement.
“We go out yearly and hold open community meetings . . . Management staff will go out, put ourselves in front of the community . . . give an update on what we’ve done for the last twelve months . . . open that up to the community and our performance review begins at that point. You tell us from a grass roots perspective . . . and if we’ve got challenges then [they] will certainly let us know.”
– Indigenous service manager24
Community participation in health care is expected to build a better understanding of community needs and priorities,25 build client expectations for quality care and strengthen community leadership for health.26
In many settings, knowledge about the ways in which social and cultural determinants (including historical and political events) affect health and access to care is important for improving service delivery.27 Facilitation can bring care providers and community members together to support two-way learning for improving care.
Turner and colleagues studied the link between community participation and CQI in Aboriginal and Torres Strait Islander PHC services. Different mechanisms were used to encourage community engagement in quality improvement.
Example: engaging clients in identifying improvement priorities
The health service in an Aboriginal and Torres Strait Islander community was keen to introduce a culturally based model for care that supported clinicians to work with Indigenous families in a holistic and empowering way. There were regular discussions between groups of community people and health service staff for identifying improvement priorities in different areas of care.
“There was a whole morning talking with the women [about maternal care]. It’s a two-way conversation around what we already provide and what women really feel they need, and the issues around birthing in a different place when they have to leave town.” – clinician28
Example: a facilitated partnership to improve health
In an Aboriginal and Torres Strait Islander community in northern Australia, there was strong participation in the health service and a whole-of-community approach to quality improvement. “Driving the health of the community” was a facilitated partnership between healthcare providers, service users and community members, which empowered the community for quality improvement. The health committee had representation from the local council, Elders and different health units and government agencies who came together for sharing, joint planning, and action, including group advocacy.
“People are taking control of their own health and we’ve got a Health Committee here. That’s been set up to look after the health in general of the community – things that work hand-in-hand with the clinical side.” – community member29
In each of the examples in the boxes, the PHC service set out to create an environment where the health service was actively engaged with the community to build trust and improve the health and wellbeing of the community.
What characterises a good facilitator?
In this section, we summarise the skills, knowledge and attributes that are used to describe expert facilitators in the quality improvement literature.
- An experienced CQI facilitator is able to clarify the improvement task (for example, its purpose, complexity, and what is involved), and decide who needs to be closely involved in the work: the roles and expertise needed, groups to be included and collaborating organisations.
- In PHC settings, facilitators need a credible knowledge base in PHC (for example, core concepts, scope of clinical care and how it is provided), how data can be used for improvement, CQI tools and methods, and the local and organisational environment.
- Facilitators need skills to engage effectively with the people involved and in the proposed change. This requires the ability to develop positive and effective working relationships with managers, staff, other service providers and client representatives.
- Good CQI facilitators have skills to communicate clearly and consistently, to appraise evidence and prepare resource materials.
- Facilitators are able to set ground rules for group work, and work with participants to dismiss fears and manage expectations. They are respectful and can listen actively, build trust, and encourage participation and different points of view to arrive at team decisions and actions.
- Facilitators may need skills in negotiation and conflict management.
- Good facilitators are also reflective on their own practice.
- Facilitators have personal attributes that contribute to effective facilitation. Expert facilitators are described as empathetic, sensitive, flexible and pragmatic. They come across as credible and passionate about their work.30
It is not suggested that effective CQI facilitation depends on the facilitator having expertise in all aspects. Skills, knowledge and confidence are developed over time through informal and formal learning opportunities and on-the-ground experience. Furthermore, it takes experience to be able to act effectively in the moment: to decide if, when and how to intervene into discussions as a group works towards its goals. Over the course of a single meeting, multiple decisions may need to be made about when and how to act, particularly if the facilitator does not know the group well.31
Facilitation skills, knowledge and confidence are developed over time through informal and formal learning opportunities and on-the-ground experience.
CQI facilitation may be shared across a PHC team, with members taking on roles according to their areas of expertise. This approach can help to sustain CQI in the event of a skilled facilitator leaving the service or program and has implications for where and how facilitator training is delivered.
Example: spreading facilitation skills across teams
For participants in Newham and colleagues’ study of barriers and enablers to implementing a quality improvement program, developing CQI capability within PHC teams was seen as key to the uptake of CQI.
“You need . . . one or two key people that have got the understanding and can drive it.” – manager and clinician, service A
Staff talked about the importance of training local staff to facilitate learning and improvement.
“I think it’s very important that [the external CQI facilitator] come and teach the staff . . . and those people who are trained by [the facilitator] can act as champions and as trainers to other health workers.” – manager and clinician, service B32
Sharing CQI facilitation across a team can help sustain CQI in the event of a skilled facilitator leaving the service or program.
Supporting continuous learning and improvement
Continuous learning is a core concept of CQI. An understanding of adult learning principles and concepts supports effective CQI facilitation.
Facilitation and adult learners
People learn in different ways. In the 1960s, adult educator Malcolm Knowles identified principles of adult learning. These internationally accepted principles underpin current adult learning programs:
- our willingness to learn as adults is connected to what we want to learn more about
- we are independent and self-directed in our learning
- we bring life experiences and prior knowledge to learning
- our readiness to learn is often connected to a need to do something in real life (for example, work tasks)
- we are goal-oriented and problem-centred learners
- our motivation to learn comes from within.33
Other characteristics of adult learners should also be considered when planning and facilitating CQI learning activities. We tend to lead complex and busy lives, have set habits and preferences, and established attitudes (including attitudes about a learning situation). Some adults can be afraid of participation in group learning – we may fear embarrassment or a loss of dignity. Adults can resent being told what to do, particularly by a person in authority. We may also worry about keeping pace with the demands made on us in a learning environment (for example, to understand CQI data). These concerns can influence the way people engage with CQI processes.
Responding to learning and communication styles
Skilled facilitation takes account of individual learning styles and presents information in a range of ways to engage all group members. We all use a range of ways to learn, but we tend to respond to one method above others. These are some of the different learning preferences people have:
- taking in information visually (preferring charts, symbols, graphics)
- taking in information by reading and writing (preferring hand-outs, PowerPoint presentations and taking notes)
- hearing and discussing information (preferring group activities)
- doing a task and getting the feel for it (with hands-on, participatory learning in work settings).
Some adults are social and interpersonal learners; others prefer solitary learning activities. Personality styles influence learning, and the way individuals behave and respond in group sessions: introverted or extroverted; logical or emotional; task-oriented or process oriented. The ability of a facilitator to recognise and respond to these preferences and communication styles develops through learning and practice.
Skilled facilitation takes account of individual learning styles and presents information in a range of ways to engage all group members.
Responding to diversity
Understanding who the participants are is important for successful facilitation outcomes and ultimately for effective improvement interventions. Diversity encompasses race, ethnic group, culture, gender, age, religion, ability/disability, sexual orientation, personality, cognitive style, knowledge bases (for example, Euro-Western and Indigenous knowledge systems) work roles, skill sets, education and more. These factors influence how people perceive themselves and how they perceive others. Those perceptions affect interactions within social settings, including the facilitation of CQI. It can be challenging to ensure that all group members feel safe to contribute to discussion when participants come from a range of backgrounds, or when the facilitator and participants come from different backgrounds.
Supporting cultural safety
Culture and language influence the way people learn, hold and share knowledge, and engage in group activities. In Indigenous health settings, culturally safe facilitation practice is crucial for engaging participants in CQI for client-centred care.
Cultural safety involves actions that recognise, respect and nurture the unique cultural identity of a person and safely meet their needs, expectations and rights. It is part of a rights-based approach to health care supported by the United Nations Declaration on the Rights of Indigenous Peoples. Cultural safety was first defined by a Māori nurse, Irihapeti Ramsden, in the cultural context of Aotearoa/New Zealand, in response to the harmful effects of colonisation and its ongoing legacy on the health and health care of Māori people.34 It has been embraced in Australian health care involving Aboriginal and Torres Strait Islander peoples, and by some other nations with a history of colonisation, discrimination and disempowerment of First Nations peoples. Similar terms are used: for example, cultural awareness, cultural respect, cultural responsiveness and cultural competence.35 Cultural safety is the term generally preferred by Aboriginal and Torres Strait Islander organisations, as being a more realistic aspiration.36
While being culturally aware involves sensitivity to the similarities and differences that exist between different cultures, working in a culturally safe way generally involves centring the cultural perspective of the other person, valuing and validating their experiences.37 It involves being aware of culture, history and racism as determinants of health, being open to different cultural understandings of health and wellbeing, and being open to different models of health care (for example, Indigenous, Western and Eastern models). Services that provide care to First Nations communities, for example, can improve cultural safety by employing and investing in the career development of First Nations staff, supporting non-Indigenous staff to develop and uphold culturally safe and respectful practices, and having strong representation of First Nations peoples in management and governance positions.38 Services can create an environment where their First Nations clients feel welcome and set up mechanisms for effective engagement with the community.
Working in a culturally safe way generally involves focusing on the cultural perspective of the other person, valuing and validating their experiences.
CQI facilitators who strive to work in a culturally safe way appreciate and validate cultural differences. Those within the dominant culture engage in critical self-reflection to question how their beliefs, values and practices inform how they work. They recognise how the systems of power and privilege affect health worker teams, and work to prevent bias and racism.39
CQI facilitation that honours Indigenous ways of knowing, being and doing40 is able to draw on participants’ cultural strengths to interpret data and plan interventions that reflect community values and priorities. Establishing a culturally safe space at the outset is essential.
Example: creating a culturally safe space for CQI training
Louise Patel and Kerry Copley are non-Indigenous CQI leaders/program coordinators with experience in facilitating CQI training workshops with Aboriginal and Torres Strait Islander staff.
“We start the day by acknowledging the traditional custodians of the land we are working on and by building a relationship with those in the room – connection before content. In a PowerPoint presentation, we confirm the importance of family (with photos) and where we come from (our homes and work history), our close working relationship with each other and the relationship we have with PHC staff and community. We’ve been in these roles for twelve years now, so we are familiar with cultural and health issues around PHC, and people know and trust us. We can tell stories to make CQI real.
We share the history of the workshops; how senior Aboriginal health practitioners saw the need for CQI training specifically for the Aboriginal and Torres Strait Islander health workforce. We invite the participants to share their learnings – that we all have important knowledge to offer. English is not the first language for many, and we assure participants it’s okay to ask for clarification, or to stop us if we don’t use plain language. We reinforce that we want the environment to be a safe place to talk, discuss issues and tell stories – confidentiality and respect are high priorities. We only take photos with permission.”
Establishing a safe environment for sharing experiences and working collaboratively can be challenging when the focus of improvement intersects with people’s lived experience. The following example describes strategies used to achieve cultural and psychological safety in workshops to improve skills in mental health care.
Example: facilitating workshops to improve responses to mental health needs
Danielle Cameron is a Yuibera woman from the Birragubba nation in Queensland, Australia, a quality improvement researcher and facilitator specialising in mental health, trauma and workforce development.
“Walking into a room, I need to know who the traditional custodians are of the area I am working in, also if there has been any ‘sorry business’ and whatever else may be going on in the community. I ask what people need to enhance their learning experience. I talk about where my family is from and always honour the land I am on.
I normally start off with an icebreaker to create safety and help people relax – this is especially important when talking about social and emotional wellbeing. As a facilitator, it is a fine line between that storytelling process and ensuring that you are creating safety for others so they can feel they can be open, but they don’t become traumatised. I generally walk around the room, keeping a warm and engaging tone and connecting with everyone so they know they are heard and seen. I think it is so important to know the material, so you can then focus on how you work the room.
I discuss suicidal ideation and other complex mental health concerns, so I always check in with people and use a thumbs-up and thumbs-down strategy for when they need to take a break. I use somatic grounding techniques. It’s very important that people feel okay when they leave.”
Resources and training for culturally safe PHC practice are offered through specialised consultants, community groups, health care, education and training providers. They include online resources and training relevant to specific First Nations settings.
Managing relationships and group dynamics
As highlighted in Part I, PHC is delivered through diverse organisational models, settings and staff. The facilitation of CQI needs to respond to each group and context. Individual engagement, behaviours and group dynamics can be influenced by multiple factors.
- Staff may feel they are being diverted from their primary role of providing care.
- Top-down power structures in health care, where traditionally doctors and medical specialists are in charge and nurses and other staff defer to their authority, may intimidate less senior team members.
- Other power relationships, such as the influence of governing boards, board members, practice owners or Indigenous Elders, may inhibit some individuals in the group.
- Managers and leaders may expect to, and be expected to, lead decision-making.
- Individual staff may feel a sense of ownership over a particular area of care and feel threatened by that area coming under scrutiny.
- Individuals may fear that changes to systems and processes will negatively affect their jobs, status or work environment.
- Individuals from diverse cultural and linguistic backgrounds need to feel culturally safe.
- Individuals may have differing perceptions of the role and value of other staff members: this can be a strength or a point of tension in the team.
These tensions need careful management by a CQI facilitator. People are more likely to participate actively in a CQI process if they feel heard and believe the improvement plan is relevant for them and the work they are doing.
The following tips (Box 7.1) were developed by highly experienced CQI facilitators who work with PHC teams.
Box 7.1 Tips for facilitating groups
Before a group session
If you are “external” to the services or practice, find out about the group you are working with and the context – team size, skill or role mix, how long people have been in the team, their experience in using CQI and issues such as workforce turnover and changes in management. Don’t go in blind.
Have a plan for how you will facilitate the discussion but be prepared to change the plan in response to where the team is at and what happens on the day.
At the start
Discuss ways of working. Set group rules for interacting in a safe and respectful way. This process often follows an icebreaker activity.
Take time to connect with the group. Find out what matters to them in relation to the topic or topics you are discussing, and their expectations for the session. You will need to get buy-in to tease out their priorities for improvement and get input for planning change.
Acknowledge that change can be difficult, especially if people feel they have little influence on the direction of the change. Ensure everyone knows that their input matters.
Throughout the session
Always remember that as the facilitator you set the tone for the discussion.
Create and maintain a safe space where people feel valued, respected and comfortable to contribute.
- Model respect for different roles and cultures within the team and how that adds value and brings different perspectives to the discussion.
- Make sure everyone has opportunities to contribute to the discussion and planning. This may mean creating different ways for people to have a voice. Not everyone feels comfortable speaking up in a large group or in front of managers.
- Make clear the expectation that everyone will be professional and respectful and that the session isn’t an opportunity to air grievances. When that happens (and it does), have a strategy for managing it. You might simply thank the person for their comment and put it into a “parking space” for later, while reminding everyone of the purpose of the discussion.
Be real! People connect with others who are genuine and congruent. A good facilitator makes connections with people and builds rapport by being open, honest and true to themselves.
– Kerry Copley and Louise Patel, CQI program coordinators, Aboriginal Medical Services Alliance Northern Territory.
For more information, see Aboriginal Medical Services Alliance Northern Territory n.d.
Facilitation is a complex task. Skills and confidence in facilitating CQI processes develop over time through formal and informal learning opportunities and through practice. Strategies for developing facilitation skills and knowledge may include:
- undertaking relevant training
- observing and learning from experienced facilitators
- identifying a mentor facilitator
- joining or building a network of people in similar roles to share learning
- taking opportunities to facilitate CQI processes and other group work
- building a tool kit of quality improvement tools and techniques for working with groups.
A wealth of resources is available about facilitating groups. Check online sources for resources that meet your needs. Encourage others who facilitate CQI in similar settings to share useful resources.
Features of effective facilitation
We have adapted the characteristics of facilitation from those identified by Harvey and Kitson in their guide to implementing evidence-based practice in health care:
- participation and involvement of key stakeholders
- development of a shared understanding of the improvement activity
- ownership and control of the CQI process by the people who are responsible for making change
- sensitivity to the local context and culture
- iterative processes integrated into routine systems and processes
- linkage of local initiatives to wider system changes
- provision of feedback on improvement activities through simple real-time mechanisms
- empowerment and enablement of others in decision-making and action
- management of group dynamics and supporting learning.41
Finally, facilitation should give PHC teams ownership of their CQI data and process and acknowledge their efforts in delivering quality care with the resources they have available. This is particularly important in settings where there is a high acute care load and a high burden of client illness. It helps to embed a culture of CQI. In the following examples, CQI facilitators reflect on key aspects of their role.
Supporting ownership of CQI
“In the early days of the CQI research, we were testing the CQI tools and the language we used, continually improving the protocols and noting what resources we needed to support PHC teams in their CQI processes. When we facilitated audits and systems assessments on the ground, we were making notes at every point about what was happening in the clinic on that day – visiting service providers, issues, how busy the clinic was – anything that would add to the data story when we fed back the results, that would help the team to understand and interpret their data. That’s when I really started to see that how I facilitated CQI was important for helping to embed CQI in those health services.”
– Lynette O’Donoghue, CQI facilitator, Menzies School of Health Research
Building trust and respect
“Reciprocal trust and respect grew as relationships developed between the CQI research facilitators and local participating health services and teams. That process fostered two-way learning. It was critically important for engagement in CQI that each health service’s CQI story was their own and confidentiality was paramount – it was up to services how they wanted to share their feedback reports.”
– Lynette O’Donoghue, CQI facilitator, Menzies School of Health Research
Acknowledging and supporting the work of PHC teams
“I have worked in remote health centres for eighteen years now. My role for the last eleven years has been as a CQI facilitator. I assist the local staff to develop, implement and evaluate quality activities that address their local needs . . . I love being able to show people how to manage what they do and see the improvement in their [key performance indicators] and just generally in the way they work, because they work very hard and – like we say in CQI – it’s about working smarter not harder.”
– Eva Williams, CQI facilitator, Northern Territory Department of Health 42
CQI facilitation should give PHC teams ownership of their CQI data and process and acknowledge their efforts in delivering quality care.
Useful group techniques
Brainstorming
Brainstorming can help a team to quickly generate ideas. Designed to encourage spontaneous ideas, lateral thinking and creative problem solving, brainstorming enables people to participate without feeling bound to represent their role, to present alternative views, to offer critique or find group consensus. In CQI, brainstorming is used in conjunction with CQI tools, for purposes such as these:
- to identify the possible causes of a quality problem identified through a clinical audit and systems assessment
- to develop a cause-and-effect diagram
- to develop a driver diagram (see Chapter 5)
- to generate change ideas (possible solutions to identified problems) for strategy development and testing through plan-do-study-act cycles.
Brainstorming requires a facilitator and clear rules. Criticism, rejection or discussion of ideas is avoided (unless for clarification). Ideas are generated rapidly and are recorded for later discussion. They should be specific enough for the group to make meaning of them (for example, “staff don’t have cultural competency training” rather than “training”).
Brainstorming aloud has potential to trigger ideas amongst the team. Silent brainstorming limits the potential for dominance by individuals; it may be more productive with reserved team members, or when participation is influenced by hierarchical work relationships. Writing each idea on a new note also makes it easier to sort ideas into categories afterwards, and to prioritise ideas based on how many people had similar thoughts.
Five Whys brainstorming
Five Whys (also known as the Toyoda technique after Sakichi Toyoda, who developed it) is a specific brainstorming technique used to identify the underlying cause of a quality problem that has been identified through a CQI process (Box 7.2). It is useful when doing root cause analysis. Use of Five Whys can help the team to understand what is really happening, rather than what appears to be happening – which may simply be another symptom of the problem. It can help the team to understand the system issues that underlie gaps in care processes or delivery of care. This understanding enables effective action to be taken to address a problem and to prevent it from happening in the future.
- The team starts with a clear problem statement and asks the question: “Why is this happening?”
- The answer is recorded. The question “Why is that?” is asked.
- This process is repeated three more times (at least) until the team reaches the root cause of the problem.
- By then asking, “What can we do to change this?”, you can develop and test a solution.
Box 7.2 Example of the Five Whys technique
Problem statement: A number of our elderly clients missed out on their vaccination.
1. Why did the elderly clients miss out on their vaccinations?
The clients were not flagged as eligible for the vaccination by the electronic client information system.
2. Why weren’t the clients flagged as eligible for the vaccination in the information system?
Dates of birth for these clients were incorrectly formatted or were missing from their client records.
3. Why were the dates of birth incorrectly formatted or missing from their client records?
Staff were unclear about the required format. Some elderly clients could not specify their date of birth, so that data field was not filled in.
4. Why were staff members unclear about the required format, or what to do when birthdates are unknown?
Staff haven’t received training in how to enter data and there is no advice on the electronic template for entering this information or for estimating date of birth.
5. Why haven’t staff received training or advice on how to enter data in the electronic template?
The information technology support team is under-resourced. Team members don’t have capacity to train staff in data entry and updating the system to include this advice hasn’t been a priority. They don’t appreciate the importance of these data in the delivery of care.
Yarning
Yarning is an Indigenous way of communicating: a conversational process for sharing stories and for developing and passing on knowledge. Yarning is used by many Indigenous peoples as a way of learning collectively, sustaining relationships and preserving and passing on cultural knowledge.43
When used appropriately as a research method by and with Indigenous peoples, yarning can help to promote cultural safety, empower participants to tell their stories in their own way and create meaningful data. Yarning has potential for engaging Indigenous participants in CQI. It can be an informal process of “having a yarn” about a topic, with the facilitator taking on the information provided throughout the conversation. Collaborative yarning can be used to identify priorities, to analyse and interpret data, and to generate improvement projects in community settings.44
Six Thinking Hats®
Six Thinking Hats® is a technique created by Edward De Bono based on a principle of parallel thinking: group members thinking in the same direction at the same time to create a broad discussion about a topic.45 In CQI, use of the Six Thinking Hats® technique can stimulate analytical thinking and evaluate potential improvement strategies from several perspectives. It can encourage individuals with entrenched views to consider other viewpoints and, as a facilitated CQI process, can prevent conflict between people with opposing perspectives.
Six different coloured hats symbolise different thinking roles. The facilitator wears a blue hat, which represents management of the thinking process. The group is given a short time to think about the improvement issue or strategy from each role perspective and to share thoughts with the group, before mentally and sometimes actually switching hats. The hats can be used in different orders and combinations to suit the purpose of the CQI session, and particular hats can be revisited if more exploration is needed.
The most promising improvement strategies can be tested using PDSA cycles, or further developed in collaboration with other PHC stakeholders. Table 7.1 presents the coloured hats and the thinking they represent with example questions. Parallel thinking can, of course, be facilitated without using the concept of hats.
|
Hat |
Think about . . . |
Example questions |
|---|---|---|
|
White |
Data Facts Information |
What data do we have about this issue? What other data do we need to decide next steps? |
|
Yellow |
A positive view Optimism Identifying benefits |
What would be the benefits of using this strategy? |
|
Black |
Risks Negatives Cautions |
What could go wrong? What negative outcomes or obstacles might there be? |
|
Green |
New ideas Possibilities Creative thinking |
What improvement strategy could we use? Is there another way of looking at this? How can the strategy or idea be developed? |
|
Red |
Emotion Gut feeling Intuitions |
What do you feel about this? |
|
Blue |
Managing the process Summarising information Moving forward |
What are our findings so far? What should we do next? |
|
Questions adapted from Advancing Quality Alliance (Aqua) 2024. | ||
Table 7.1 Using the Six Thinking Hats® technique.
Many resources are available about the Six Thinking Hats®. Training is available.46
Using Six Thinking Hats®
“One of the benefits of using Six Thinking Hats® with a team is that it puts everyone in the position of having to consider the topic from each viewpoint, rather than just the ones that they are personally more comfortable with.
The Thinking Hats is a great tool to use with Aboriginal Health Boards and Community members as well as primary healthcare teams. It can be used to really get to the root of a problem and then to use that information to formulate a plan to drive the improvement process.
It gives everyone a voice and can be a fun and energising way to conduct a discussion that can lead to a much clearer picture of what the important next steps should be.”
– Kerry Copley, CQI program coordinator, Aboriginal Medical Services Alliance Northern Territory
Stakeholder mapping
The complex and comprehensive nature of PHC and the systems focus of CQI mean that most improvement initiatives involve multiple stakeholders. Stakeholder mapping is a useful technique. It is relevant to understanding the causes of variation in care quality and identifying who needs to be engaged in developing improvement plans and progressing improvement strategies. This will include individuals, groups and organisations who are affected by, and influence, the quality of care and the effectiveness and sustainability of the CQI initiative.
After the quality issue or improvement goal has been identified, stakeholder mapping involves three steps:
- listing stakeholders and organising them into groups (for example, clients, carers and families; other PHC teams, other health professionals, other service providers; managers; community groups, councils; support organisations, researchers)
- conducting a stakeholder analysis by “mapping” their relationships to the quality problem and to each other (for example, using sticky notes)
- identifying potential roles for stakeholders in developing and implementing improvement programs and interventions.
Many online resources are available to support stakeholder mapping and analysis. The usefulness of these resources will vary, based on the variables that are most relevant to your CQI project.
Resources for stakeholder mapping
“I think that good old-fashioned sticky notes are probably most helpful for stakeholder mapping – then you can organise and reorganise and fiddle with placements until you get the categories and relationships right. There are digital tools available that work pretty well to visualise and communicate relationships, as well as diagrams and matrices to help think through concepts, but sticky notes are the most flexible, simple and easy way to get started.”
– Katie Conte, public health and systems thinking researcher
Developing a power–interest grid
As part of stakeholder mapping, a power–interest grid technique may be helpful for prioritising whom to engage in your improvement initiative and how to manage their involvement. This technique puts stakeholders into categories according to their influence and interest.
When putting stakeholders into categories, consider the positions of individuals within their organisation and their abilities to exercise change, and their interest in the quality problem.47 The example at Figure 7.1 offers a general guide for engaging stakeholders according to their power and interest.
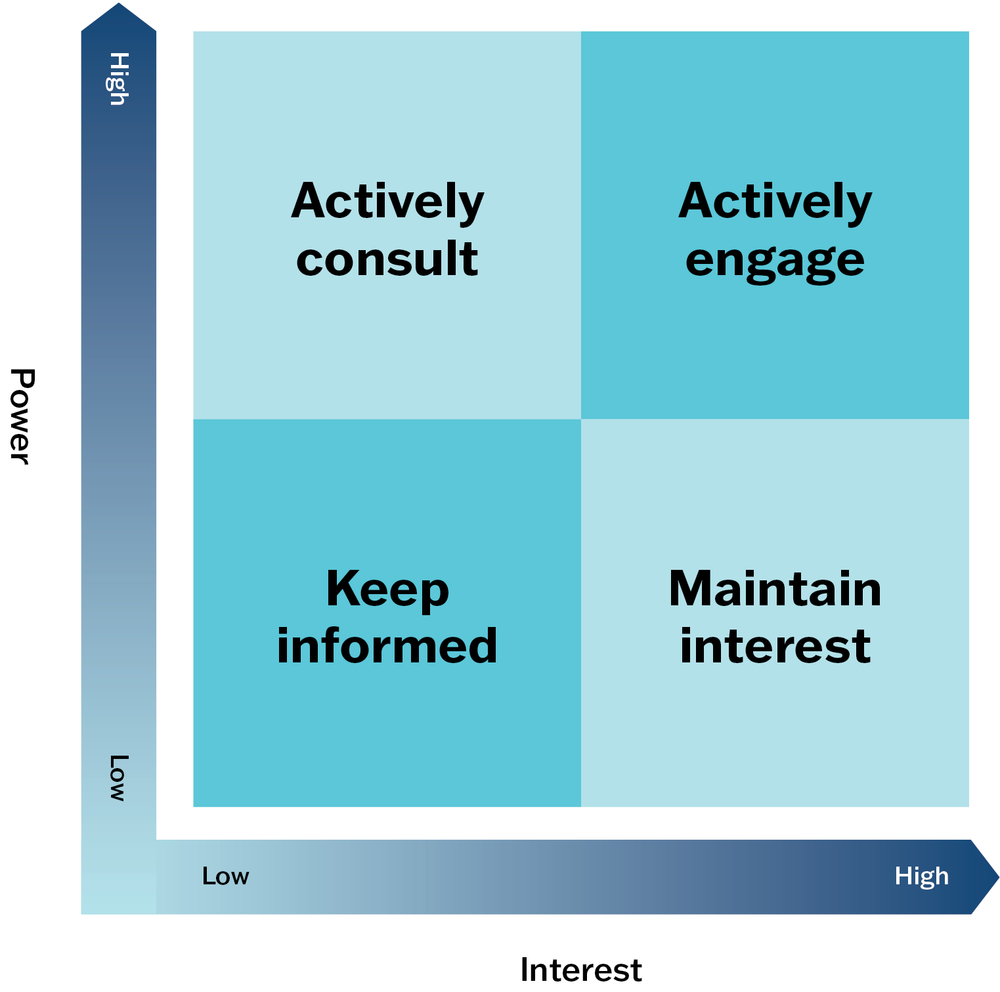
Figure 7.1 Example elements of a power-interest grid.
The improvement goal will influence the strategies you use to engage different stakeholders. For example, while important to actively engage stakeholders with high power and high interest, building relationships and gaining support from influential stakeholders with less interest in your project may be necessary for achieving your goal. Stakeholders with low power and low interest in the quality issue may require less regular and detailed communication, but if you aim to empower an interested group through the CQI process, you will be wanting to engage them actively in the project.
Continuous quality improvement collaboratives
CQI collaboratives are “groups of professionals coming together, either from within an organisation or across multiple organisations, to learn from and motivate each other in order to improve the quality of health services”.48 These collaboratives are widely adopted as an approach to shared learning and improvement in health care. There is some evidence that collaboratives can improve care processes, client outcomes, service use or cost (or both).49
Many CQI collaboratives are based on the Institute for Healthcare Improvement’s “Breakthrough Series” approach,50 which uses a series of learning workshops, action periods, local support and continuous measurement. Some collaboratives use aspects of the chronic care model (see Chapter 1) and communities of practice approach.51 The underpinning theory of change is that teams learn faster and are more effective in implementing improvement ideas and assessing their own progress when collaborating and benchmarking with other teams. Effective teams are, in turn, able to improve the quality of care they deliver.52
CQI collaboratives have been successfully applied in PHC.
CQI collaboratives have been successfully applied in PHC. In Australia, for example, a Primary Care Collaboratives project aimed to improve CQI capacity in general practices, Aboriginal and Torres Strait Islander health services and pharmacies by building capacity in the regional organisations that support them. Fifty teams engaged 341 frontline services in collaboratives, nominating diverse topics including diabetes, cardiovascular disease, data quality, e-health and men’s health. After initial challenges, repeated CQI cycles recorded greater than 30 per cent improvement in the measured competence of participants in quality improvement activities.53
Facilitating CQI collaboratives
Quality improvement collaboratives may be large or small scale. Regardless of scale, a CQI collaborative has five essential features:
- identifying a specified topic based on a shared quality problem (for example, large variations in care or gaps between best and current practice)
- engaging clinical and CQI experts in sharing evidence, change concepts and CQI methods, consolidating ideas and providing support for improvement
- bringing together multi-professional teams from multiple sites to share findings, innovations and lessons learnt from their improvement efforts
- working with participants to set clear and measurable goals, and to plan and undertake data collection to test changes on a small scale, using CQI tools and processes
- facilitating planned activities that promote collaboration to learn and share ideas, innovations and experiences (for example, meetings, site visits, web-based activities, coaching and feedback) over a limited time.54
The facilitation of a CQI collaborative is structured around these features.
Box 7.3 offers tips for facilitating a CQI collaborative.
Box 7.3 Facilitation tips – CQI collaboratives
At the outset
- Get buy-in from senior leaders (clinical and administrative) in the participating organisations ahead of the start date. Time, resources, work, and supportive conditions will be needed to make and sustain improvements.
- Ensure there is solid IT infrastructure for collecting data and sharing practice.
- Establish participants’ reasons for taking part and the main objectives of the collaborative.
- Clarify expectations and adjust the collaborative to meet participants’ needs. Be realistic and open about what is possible.
- Develop a “theory of change” that links activities and planned outcomes.
- Team building may be needed to encourage collaboration and develop the trust needed to share data and less successful lessons amongst participants.
During the learning activities
- Emphasise mutual learning and open sharing of outcome data and details of practice.
- Ensure participants set SMART goals (see Chapter 6).
- Use simple measurement tools.
- Equip and support teams to deal with data and change challenges, and to adapt ideas.
- Pay attention to motivating and empowering participants and teams.
- Use multiple methods of communication to build a close participant network.
- Towards the end of the collaborative
- Plan for sustaining the improvements, involving organisation leaders.
- Plan for continued use of CQI by participants in their PHC services.
- Promote the benefits of maintaining an informal CQI learning network after the collaborative ends.55
Example: the Childhood Anaemia Collaborative, Northern Territory, Australia
The Childhood Anaemia Collaborative brought interested Aboriginal community controlled health services together over two years (from mid-2019 to 2021) to focus on improving the prevention and rates of testing and treatment of anaemia in Aboriginal children.
Services who participated shared their data for anaemia care and met online once a month. Online activities enabled small teams in widely dispersed services to participate, and to continue working together during the Covid-19 pandemic. Dashboards were used to display monthly data and trends over time, enabling teams to benchmark data, track progress and identify areas for improvement.
Based on the improvement priorities identified through analysis of their health service’s data, each of the participating teams undertook monthly plan-do-study-act cycles to implement and test strategies for improving the quality of anaemia care. The collaborative enabled teams to discuss their experiences and exchange improvement ideas, strategies and resources.56
Summary
CQI facilitation is an individual role as well as a process involving individuals and groups. Facilitation enables staff and others involved in CQI processes to put evidence into practice to improve care. CQI facilitators need skills in improvement methods, interpersonal communication, group processes, negotiation and empowering others. Leadership and management are important components of facilitation: management of people, meetings, projects and change. The ability to tailor facilitation to the local context and to participants is crucial.
A range of facilitation techniques is available to support the implementation of CQI cycles. The techniques we have described in this chapter reflect core concepts of CQI. All of the techniques focus on improving systems and processes rather than individual performance, recognition that those who work in the system have the knowledge and insight to improve the system, the use of data and systematic planning at the local level, and continuous learning and improvement.
References
Aboriginal Medical Services Alliance Northern Territory (n.d.). Continuous quality improvement (CQI). http://www.amsant.org.au/cqi-new/.
Advancing Quality Alliance (Aqua) (2024). Six Thinking Hats. Quality, Service Improvement and Redesign (QSIR) Tools. https://aqua.nhs.uk/qsir-tools/.
Atkinson, P., M. Baird and K. Adams (2021). Are you really using yarning research? Mapping social and family yarning to strengthen yarning research quality. AlterNative: An International Journal of Indigenous Peoples 17(2): 191–201. DOI: 10.1177/11771801211015442.
Australian Health Practitioner Regulation Agency and National Boards (2020). The National Scheme’s Aboriginal and Torres Strait Islander Health and Cultural Safety Strategy 2020–2025. https://www.ahpra.gov.au/About-Ahpra/Aboriginal-and-Torres-Strait-Islander-Health-Strategy/health-and-cultural-safety-strategy.aspx.
Baskerville, B., C. Liddy and S. Hogg (2012). Systematic review and meta-analysis of practice facilitation within primary care settings. Annals of Family Medicine 10(1): 63–74. DOI: 10.1370/afm.1312.
Berta, W., L. Cranley, J. Dearing, E. Dogherty, J. Squires and C. Estabrooks (2015). Why (we think) facilitation works: insights from organizational learning theory. Implementation Science 10(1): 141. DOI: 10.1186/s13012-015-0323-0.
Bessarab, D. and B. Ng’Andu (2010). Yarning about yarning as a legitimate method in Indigenous research. International Journal of Critical Indigenous Studies 3(1): 37–50. DOI: 10.5204/ijcis.v3i1.57.
Best, A., T. Greenhalgh, S. Lewis, J. Saul, S. Carroll and J. Bitz (2012). Large-system transformation in health care: a realist review. Milbank Quarterly 90(3): 421–56. DOI: 10.1111/j.1468-0009.2012.00670.x.
Brimblecombe, J., R. Bailie, C. van Den Boogaard, B. Wood, S. Liberato, M. Ferguson et al. (2017). Feasibility of a novel participatory multi-sector continuous improvement approach to enhance food security in remote Indigenous Australian communities. SSM – Population Health 3(C): 566–76. DOI: 10.1016/j.ssmph.2017.06.002
Congress of Aboriginal and Torres Strait Islander Nurses and Midwives (CATSINaM) (2014). Towards a shared understanding of terms and concepts: strengthening nursing and midwifery care of Aboriginal and Torres Strait Islander peoples. Canberra: CATSINaM.
Copley, K. and L. Patel (2021). The Northern Territory Continuous Quality Improvement Strategy. Darwin: Aboriginal Medical Service Alliance Northern Territory.
Cranley, L., G. Cummings, J. Profetto-McGrath, F. Toth and C. Estabrooks (2017). Facilitation roles and characteristics associated with research use by healthcare professionals: a scoping review. BMJ Open 7: e014384. DOI: 10.1136/bmjopen-2016-014384.
Cross, T., B. Bazron, K. Dennis and M. Isaacs (1989). Towards a culturally competent system of care: a monograph on effective services for minority children who are severely emotionally disturbed. Washington, DC: Georgetown University Child Development Center.
de Bono (n.d.). de Bono. www.debono.com.
de Bono, E. (2000). Six Thinking Hats. London: Penguin.
de Silva, D. (2014). Improvement collaboratives in health care. Evidence scan no. 21. London: Health Foundation.
Dogherty, E., M. Harrison and I. Graham (2010). Facilitation as a role and process in achieving evidence-based practice in nursing: a focused review of concept and meaning. Worldviews on Evidence-Based Nursing 7(2): 76–89. DOI: 10.1111/j.1741-6787.2010.00186.x.
Dogherty, E., M. Harrison, I. Graham, A. Vandyk and L. Keeping-Burke (2013). Turning knowledge into action at the point-of-care: the collective experience of nurses facilitating the implementation of evidence-based practice. Worldviews on Evidence-Based Nursing 10(3): 129–39. DOI: 10.1111/wvn.12009.
Geia, L., B. Hayes and K. Usher (2013). Yarning/Aboriginal storytelling: towards an understanding of an Indigenous perspective and its implications for research practice. Contemporary Nurse: A Journal for the Australian Nursing Profession 46(1): 13–17. DOI: 10.5172/conu.2013.46.1.13.
Gollan, S. and K. Stacey (2021). Australian Evaluation Society First Nations Cultural Safety Framework. Melbourne: Australian Evaluation Society.
Harvey, G. and A. Kitson (2016). PARIHS revisited: from heuristic to integrated framework for the successful implementation of knowledge into practice. Implementation Science 11: 33. DOI: 10.1186/s13012-016-0398-2.
Harvey, G. and A. Kitson (2015). Implementing evidence-based practice in healthcare: a facilitation guide. London: Taylor & Francis Ltd.
Harvey, G. and E. Lynch (2017). Enabling continuous quality improvement in practice: the role and contribution of facilitation. Frontiers in Public Health 5: 27. DOI: 10.3389/fpubh.2017.00027.
Harvey, G., B. McCormack, A. Kitson, E. Lynch and A. Titchen (2018). Designing and implementing two facilitation interventions within the “Facilitating Implementation of Research Evidence (FIRE)” study: a qualitative analysis from an external facilitators’ perspective. Implementation Science
13: 141. DOI: 10.1186/s13012-018-0812-z.
Hogan, C. (2002). Understanding facilitation: theory and principles. London: Kogan Page.
Institute for Healthcare Improvement (2003). The Breakthrough Series: IHI’s collaborative model for achieving breakthrough improvement. Innovation series 2003. Cambridge, MA: Institute for Healthcare Improvement.
Kitson, A., G. Harvey and B. McCormack (1998). Enabling the implementation of evidence based practice: a conceptual framework. Quality in Health Care 7(3): 149–58. DOI: 10.1136/qshc.7.3.149.
Knight, A., M. Dhillon, C. Smith and J. Johnson (2019). A quality improvement collaborative to build improvement capacity in regional primary care support organisations. BMJ Open Quality 8(3): p.e000684–e84. DOI: 10.1136/ bmjoq-2019-000684.
Knowles, M. (1990). The adult learner: a neglected species. Houston, TX: Gulf Publishing.
Larkins, S., K. Carlisle, N. Turner, J. Taylor, K. Copley, S. Cooney et al. (2019). “At the grass roots level it’s about sitting down and talking”: exploring quality improvement through case studies with high-improving Aboriginal and Torres Strait Islander primary healthcare services. BMJ Open 9(5): e027568. DOI: 10.1136/bmjopen-2018-027568.
Laycock, A., G. Harvey, N. Percival, F. Cunningham, J. Bailie, V. Matthews et al. (2018). Application of the i-PARIHS framework for enhancing understanding of interactive dissemination to achieve wide-scale improvement in Indigenous primary healthcare. Health Research Policy and Systems 16: 117. DOI: 10.1186/s12961-018-0392-z.
Lindenauer, P.K. (2008). Effects of quality improvement collaboratives. BMJ 336(7659): 1448–9. DOI: 10.1136/bmj.a216.
Lowitja Institute (2022). Tools for supporting culturally safe evaluation. Melbourne: Lowitja Institute.
Martin-Booran Mirraboopa, K. (2003). Ways of knowing, being and doing: a theoretical framework and methods for Indigenous and indigenist re-search. Journal of Australian Studies: Voicing Dissent 27(76): 203–14. DOI: 10.1080/14443050309387838.
McCalman, J., R. Bailie, R. Bainbridge, K. McPhail-Bell, N. Percival, D. Askew et al. (2018). Continuous quality improvement and comprehensive primary health care: a systems framework to improve service quality and health outcomes. Frontiers in Public Health 6: 76. DOI: 10.3389/fpubh.2018.00076.
Mukerji, G., I. Halperin, P. Segal, L. Sutton, R. Wong, L. Caplan et al. (2019). Beginning a diabetes quality improvement project. Canadian Journal of Diabetes 43(4): 234–40. DOI: 10.1016/j.jcjd.2019.02.003.
Newham, J., G. Schierhout, R. Bailie and P.R. Ward (2016). “There’s only one enabler; come up, help us”: staff perspectives of barriers and enablers to continuous quality improvement in Aboriginal primary health-care settings in South Australia. Australian Journal of Primary Health 22(3): 244–54. DOI: 10.1071/PY14098.
Northern Territory Remote Locum Program and Aboriginal Medical Services Alliance of the Northern Territory (AMSANT) (n.d.). Continuous Quality Improvement in the NT. eLearning module. https://www.rahc.com.au/elearning-resources/elearning.
Øvretveit, J. (2014). Perspectives on context: how does context affect quality improvement? London: Health Foundation.
Øvretveit, J., P. Bate, P. Cleary, S. Cretin, D. Gustafson, K. McInnes et al. (2002). Quality collaboratives: lessons from research. Quality and Safety in Health Care 11: 345–51. DOI: 10.1136/qhc.11.4.345.
Papps, E. and I. Ramsden (1996). Cultural safety in nursing: the New Zealand experience. International Journal for Quality in Health Care 8(5): 491–7. DOI: 10.1093/intqhc/8.5.491.
Percival, N., L. O’Donoghue, V. Lin, K. Tsey and R. Bailie (2016). Improving health promotion using quality improvement techniques in Australian Indigenous primary health care. Front Public Health 4: 53 DOI: 10.3389/fpubh.2016.00053.
Persson, L., N. Nga, M. Målqvist, D. Thi Phuong Hoa, L. Eriksson, L. Wallin et al. (2013). Effect of facilitation of local maternal-and-newborn stakeholder groups on neonatal mortality: cluster-randomized controlled trial. PLOS Medicine 10(5): e1001445–e45. DOI: 10.1371/journal.pmed.1001445.
Schouten, L., M. Hulscher, J. van Everdingen, R. Huijsman and R. Grol (2008). Evidence for the impact of quality improvement collaboratives: systematic review. BMJ 336(7659): 1491–4. DOI: 10.1136/bmj.39570.749884.BE.
Schwarz, R. (2002). The skilled facilitator: a comprehensive resource for consultants, facilitators, managers, trainers, and coaches. New York: Jossey-Bass.
Shaw, E., A. Looney, S. Chase, R. Navalekar, B. Stello, O. Lontok et al. (2010). “In the moment”: an analysis of facilitator impact during a quality improvement process. Group Facilitation 10: 4–16.
Turner, N., J. Taylor, S. Larkins, K. Carlisle, S. Thompson, M. Carter et al. (2019). Conceptualizing the association between community participation and CQI in Aboriginal and Torres Strait Islander PHC services. Qualitative Health Research 29(13): 1904–15. DOI: 10.1177/1049732319843107.
Walker, M., B. Fredericks, K. Mills and D. Anderson (2014). “Yarning” as a method for community-based health research with Indigenous women: the Indigenous women’s wellness research program. Health Care for Women International 35(10): 1216–26. DOI: 10.1080/07399332.2013.815754.
Wells, S., O. Tamir, J. Gray, D. Naidoo, M. Bekhit and D. Goldmann (2018). Are quality improvement collaboratives effective? A systematic review. BMJ Quality and Safety 27(3): 226–40. DOI: 10.1136/bmjqs-2017-006926.
Wise, M., S. Angus, E. Harris and S. Parker (2013). National appraisal of continuous quality improvement initiatives in Aboriginal and Torres Strait Islander primary health care: final report. Melbourne: Lowitja Institute.
Woods, C., K. Carlisle, S. Larkins, S.C. Thompson, K. Tsey, V. Matthews et al. (2017) Exploring systems that support good clinical care in Indigenous primary health-care services: a retrospective analysis of longitudinal systems assessment tool data from high-improving services. Frontiers in Public Health 5: 45. DOI: 10.3389/fpubh.2017.00045.
1 Kitson, Harvey and McCormack 1998, adapted.
2 Schwarz 2002.
3 Hogan 2002.
4 Harvey and Lynch 2017.
5 Harvey and Kitson 2016.
6 Harvey, McCormack et al. 2018.
7 Best, Greenhalgh et al. 2012; Dogherty, Harrison and Graham 2010.
8 Cranley, Cummings et al. 2017.
9 Baskerville, Liddy and Hogg 2012.
10 Persson, Nga et al. 2013.
11 Baskerville, Liddy and Hogg 2012.
12 Persson, Nga et al. 2013.
13 Harvey and Lynch 2017.
14 Brimblecombe, Bailie et al. 2017; Larkins, Carlisle et al. 2019; Percival, O’Donoghue et al. 2016.
15 Newham, Schierhout et al. 2016; Woods, Carlisle et al. 2017.
16 Newham, Schierhout et al. 2016.
17 Larkins, Carlisle et al. 2019.
18 Harvey and Lynch 2017.
19 Berta, Cranley et al. 2015.
20 Larkins, Carlisle et al. 2019.
21 Harvey and Lynch 2017.
22 Harvey and Kitson 2015; Larkins, Carlisle et al. 2019; Laycock, Harvey et al. 2018; Øvretveit 2014.
23 Baskerville, Liddy and Hogg 2012.
24 Larkins, Carlisle et al. 2019.
25 McCalman, Bailie et al. 2018.
26 Wise, Angus et al. 2013.
27 Turner, Taylor et al. 2019.
28 Turner, Taylor et al. 2019, 1908.
29 Turner, Taylor et al. 2019, 1908.
30 Dogherty, Harrison et al. 2013; Harvey and Kitson 2015; Harvey and Lynch 2017.
31 Shaw, Looney et al. 2010.
32 Newham, Schierhout et al. 2016, 250.
33 Knowles 1990.
34 Papps and Ramsden 1996.
35 Cross, Bazron et al. 1989.
36 Congress of Aboriginal and Torres Strait Islander Nurses and Midwives (CATSINaM) 2014.
37 Lowitja Institute 2022.
38 Australian Health Practitioner Regulation Agency and National Boards 2020.
39 Gollan and Stacey 2021.
40 Martin-Booran Mirraboopa 2003.
41 Harvey and Kitson 2015.
42 Northern Territory Remote Locum Program and Aboriginal Medical Services Alliance of the Northern Territory (AMSANT), n.d.
43 Atkinson, Baird and Adams 2021.
44 Bessarab and Ng’Andu 2010; Geia, Hayes and Usher 2013; Walker, Fredericks et al. 2014.
45 de Bono 2000.
46 de Bono n.d.
47 Mukerji, Halperin et al. 2019.
48 de Silva 2014.
49 de Silva 2014; Lindenauer 2008; Schouten, Hulscher et al. 2008; Wells, Tamir et al. 2018.
50 Institute for Healthcare Improvement 2003.
51 de Silva 2014.
52 Wells, Tamir et al. 2018
53 Knight, Dhillon et al. 2019.
54 Schouten, Hulscher et al. 2008; Wells, Tamir et al. 2018.
55 de Silva 2014; Øvretveit, Bate et al. 2002.
56 Copley and Patel 2021.