Chapter 7
PUBLIC HEALTH AND THE SUSTAINABILITY OF CITIES: SYDNEY AIRPORT’S NOISE POLLUTION AND COMMUNITY WELLBEING
The development of international airports is a driving force behind globalisation. But growth in air traffic is also a threat to sustainable community health in the vicinity of airports. Airports are an increasingly important dimension to the economic sustainability of cities but the health and wellbeing of its citizens must also be considered in the process of development assessment and impact mitigation.
Human health impacts (that are both positive and negative) should be accounted for in the planning, development and management of urban environments (Capon and Blakely, 2007). Public health and environmental health impacts clearly have a spatial dimension. Capon and Blakely (2007, p. 54) describe a 10-point checklist for the planning and development of healthy and sustainable communities. The ten domains in the checklist are essentially physical characteristics of places: outdoor air quality; water supply and sanitation; housing and buildings; food; local shops and services; schools and other educational institutions; community spaces; transport and street connectivity; communication technology; economy and employment.
The complexity of these emerging public health problems presents a major new challenge for sustainable development. Integrated solutions will require health care professionals, epidemiologists, engineers, environmental scientists, urban planners, designers and managers, policy specialists, economists and social scientists to grapple with working together in new ways. We have already argued for the application of the trans-disciplinary approach that is advocated in medical science by Higginbotham et al. (2001) to research into quality of life and environmental health (Black and Hayashi, 2005; Issarayangyun et al., 2005a) – a framework that is helpful in the formulation of common conceptual approaches and for integrated solutions that match the 154spatial scale and pace of these emerging health problems in urban environments.
The issues of event, time and place are the basis of public health and environmental health studies, as noted over a century and a half ago by Dr John Snow, the founder of geographical epidemiology. In this chapter, we use space to articulate how geographers, urban planners and urban managers might, at the local, neighbourhood scale, comprehend the close interrelationship between human activity, industry, the physical environment and human disease, ill health and mortality. To do this we review the fundamental approaches adopted by public health specialists. Both the University of Sydney and the University of New South Wales have contributed substantially to the literature on public health (next section). In the following section, concepts from the new public health curriculum at Sydney University are illustrated by the case of aircraft noise at Sydney International Airport and noise impacts on individual stress and hypertension. Whilst we see the contemporary approach in forging greater collaboration between planners and public health specialists as a desirable step in the right direction, we conclude the paper with suggestions on more integrated solutions that emphasise the importance of GIS (Geographic Information Systems), the modern-day equivalent technique so powerful in Dr Snow’s towering intellect and painstaking site investigations.
Public and environmental health – new approach
Innovation is necessary to achieve socially-sustainable solutions. As pointed out by Kearns et al. (2007, p. 49) partial solutions generated by traditionally distinct professional disciplines are unlikely to result in real innovation. Therefore, our suggestion, in responding to the challenges posed by Capon and Blakely, is that urban planners and urban managers might start with the public health literature, in particular, the diagrammatic representation of the way in which a variety of influences (including the social environment and the physical environment) interact to affect individual health and wellbeing (Baume and Irvine, 1995: p. 9) and examples of the non-health sectors (including housing and public planning) which may have a role in working with the health sector (Bauman, 1995). Furthermore, it should be noted that there has been a change in approach to environmental studies within public health that 155emphasises the close interrelationship between human activity, industry, the physical environment and human disease, ill health and mortality (Frith, 1995: p. 104). This background is explained using a public health paradigm developed by the University of New South Wales. The population health integration within the medical curriculum at the University of Sydney similarly aims to bridge the gap between the traditional, individual-level health care approach and population-based health care (Trevena et al., 2005).
We believe the eight key concepts of the population-health learning outcomes of this new curriculum are equally applicable to the way that research studies of the public and environmental health issues in cities could be designed so as to promote sustainable outcomes. The concepts are: 1) distribution – How common is the problem in the total population and in different subgroups?; 2) cause – what causes the problem?; 3) prevention – How can the problem be prevented?; 4) management – What is the most appropriate management of the problem at individual system and population levels, and how can systems be continually improved?; 5) evidence base – How strong is the evidence about the distribution and cause of the problem, its prevention and its management?; 6) personal effects – What are the personal effects of having the problem?; 7) societal effects – What are the effects of the problem (and its management) on, and in, society?; and 8) societal response – How does (and could) society respond to the problem? Later, these concepts are illustrated with reference to aircraft noise in communities around Sydney airport, but firstly we review contemporary research and practice.
Contemporary planning and public health approach
There is a body of literature that links urbanisation and urban layout with obesity (for example, Frank et al., 2003). There is also an increasing awareness of the need for planners and health specialists to work together more closely. Kearns et al. (2007) have defined some of the research challenges for urban researchers from a socio-ecological perspective as:
The spatial and temporal dynamics of social and environmental determinants of human health in urban systems. Who gets sick and where do they live? What are the 156relative contributions of social versus environmental factors? What types of interventions are available and appropriate?
Measures of health in different urban forms. What contribution does urban pattern and social–ecological processes in urban environments make to the functionality of urban habitats? Can we identify the characteristics of dysfunctional and functional urban landscapes and incorporate this knowledge into better urban planning, design, construction and management?
Harris et al. (2007: p. 150) consider that a range of practical actions from a public health perspective are required, such as:
- a shift towards ‘healthy’ public policy that increases the capacity of the health sector to engage inter-sectorally with urban planning;
- understanding the regulatory framework that governs urban planning and development;
- learning from past lessons (literature review) concerning advocating for health as part of the urbanisation process; and
- building on the strengths of, and meeting the challenges set by, health impact assessments.
There is already a body of knowledge from which to respond to the challenges articulated by these authors. The influence of built-form factors on health (and wellbeing) is already established from evidence cited in the literature, locally in Sydney for Granville (NSW Health, Sydney West Area Health Service, 2006: pp. 24–25; see also Appendix 2), and, more generally, in the international literature (Meade and Earickson, 2000: pp. 136–140; Jackson, 2003; Frumkin et al., 2004; Galea and Vlahov, 2005a, 2005b; Giles-Corti, 2006; Capon and Dixon, 2007; Harris et al., 2007). The Granville Health Impact Study (NSW Health, Sydney West Area Health Service, 2006) considers five themes: transport, traffic and parking, and pedestrians; business, industry and neighbourhood nodes; community facilities, medical services, child care and schools; landscape, parks, recreation, access to a local river; and housing and urban design. 157
Within this broad literature linking urban development and public health sits the more specific and widely researched topic of the social and environmental impacts of transport (see Chapter 2). For example, the eight concepts from the University of Sydney’s medical curriculum that are applicable to the way studies of the public and environmental health issues in cities can be designed so as to promote sustainable outcomes can be illustrated from our broadly-focused research, such as: road traffic noise (Black et al., 1997); lead in petrol and the impact on children’s IQs (Cowie et al., 1997); accident risk to pedestrians crossing the road (Black and Black, 2001); and the stress and hypertension caused by aircraft noise (Black et al., 2007; Black and Black, 2007).
All events that impact on the health and wellbeing of the urban population, whether they have been a result of the built form in general or motor vehicles or jet aircraft in particular exhibit a geographical pattern of incidence. It is the appropriate management of such factors that contribute to more sustainable cities. To further illustrate patterns of geographical incidence and management, we focus on one specific illustration of an individual heath problem in environmental health that is literally in Sydney University’s backyard (or over its backyard): that is, aircraft noise at Sydney Airport.
Aircraft noise and environmental health
Aircraft noise is one of the best illustrations of the important health issues that are a major component of sustainable health in cities. Our research on aircraft noise was of sufficient social importance to be included in The Sydney Morning Herald, Sydney Magazine (Issue #60 of April, 2008: p. 58). The example is also a timely reminder that in cities the ‘dose’, in this case aircraft noise, may have variable spatial impacts over time. The research was undertaken when all three runways were operational so as to share the noise north-south and east-west of the airport. In November 2007, immediately after the results of the federal election were announced, the Sydney Airport Corporation Ltd notified that the East-West Runway would be closed for two years from 2008 to complete some necessary safety construction works at the ends of the runways. As a consequence, those suburbs north and south of the airport will be exposed to substantially more flights under parallel runway operations and hence more noise events. 158
Distribution
How common is the noise problem (annoyance, quality of life, stress and hypertension) in the total population (spatial patterns) and in different subgroups (socioeconomic status and equity)? These are important questions for both urban geographers and planners. Aircraft noise has been a vexing health and wellbeing issue for residents near major commercial and military airports in cities throughout the world especially with the introduction of commercial jets in the 1950s. Construction and operation of the third runway at Sydney airport in the mid-1990s highlighted this issue for the University of Sydney’s backyard neighbours.
Figure 40: Aircraft noise at Sydney Airport, 1999
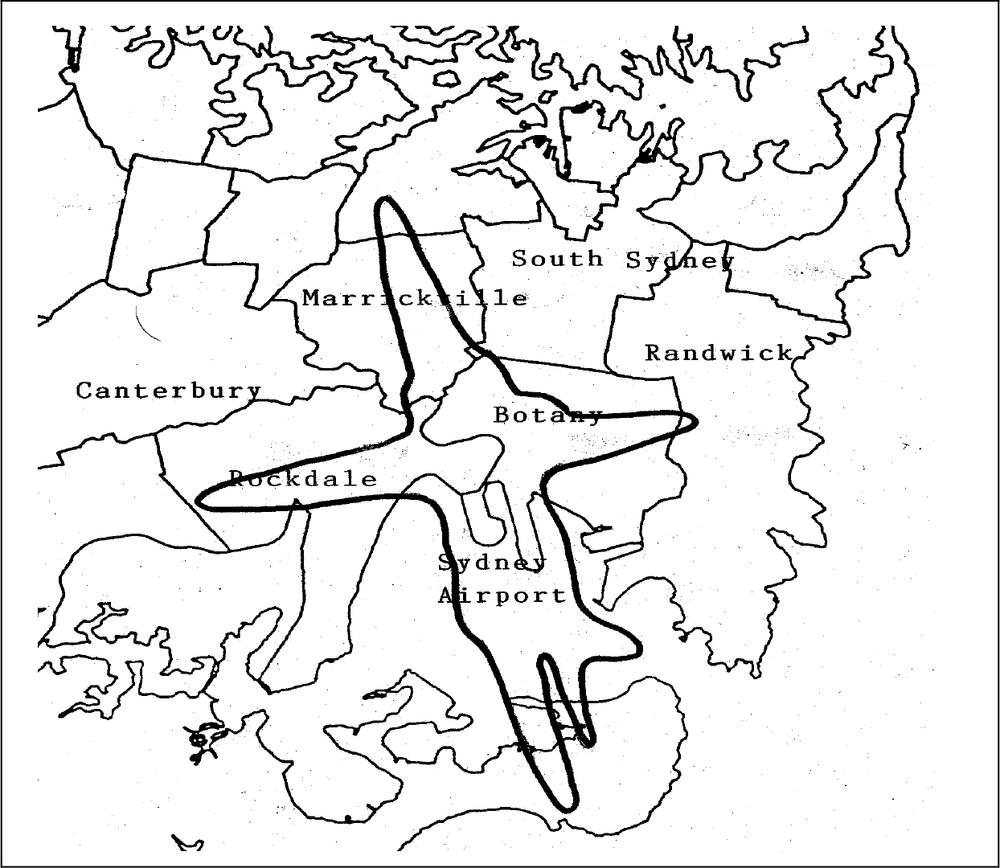
Source: based on http://www.airservicesaustralia.com/reports/anei/eo20_085.pdf 159
Figure 40 shows the 1999 ANEI (Australian Noise Exposure Index) 25 contour from which detailed demographic analyses of census data will reveal the number and categories of people highly affected by the annoyance from aircraft noise.
The Australian Noise Exposure Forecast (ANEF) is the metric, calculated from a standard computer program, and used in compatible land use planning in the vicinity of airports based on projections of air traffic growth and the types of jet aircraft flying in the future (AirServices Australia, 1999). The ANEF 25 contour is a critical piece of information because social surveys throughout the world demonstrate a high proportion of residents living within this boundary are ‘highly annoyed’ or ‘moderately annoyed’ from aircraft noise (Fidell et al., 1991). When the actual aircraft movements (aircraft type, flight tracks, etc.) recorded for one year at the airport are fed into the same computer software, the noise contours produced are called the ANEI.
The Number-Above (NA) metric is defined as the number of noise events during a given period that are louder than a selected threshold level and provides another approach to the distributional question. Our research (Issarayangyun et al., 2005b) obtained the average annual day of N70 contour maps around Sydney Airport which are periodically produced by AirServices Australia (see Figure 40. The level of 70 dB(A) was chosen because it is commonly the case that the outdoor sound level will be attenuated approximately 10 dB(A) by the structure of a house. An internal noise level of 60 dB(A) is the sound pressure level of a noise event that is likely to interfere with conversation or with listening to the radio or the TV (Southgate et al., 2000).
Cause
The source of aircraft noise is obvious, even to the casual observer, although the area of air traffic control and noise management is a highly specialised area of engineering as it entails the measurement, modelling and estimation of aircraft noise. Airport noise is caused by aircraft in their cycle of landing, taxiing and taking-off. There is additional noise from an airport as an industrial land use, especially where ground running of aircraft takes place during routine maintenance. Traffic control in terminal airspace conforms to international regulations (ICAO). However, there are additional local operational procedures 160aimed at minimising aircraft noise on surrounding land uses, such as the arrival flight paths for jet aircraft arriving at Sydney airport (the use of flight paths over Botany Bay where possible).
Prevention
How this noise problem for those living and working in the vicinity of Sydney Airport, in general, and in Sydney University’s backyard, in particular, can be eliminated is purely a political, not a technical, question. The prevention involves building a second Sydney airport outside of the Sydney metropolitan basin. For example, Goulburn has been evaluated as a potential site some 20 years ago and Newcastle Airport at Williamstown – which is currently shared by the RAAF with civilian flights – has been mooted recently with suggestions of a high-speed rail to Sydney (The Sydney Morning Herald, 13 June, p. 15).
Closing down the existing airport at Mascot is unlikely. Despite the political statements about a second Sydney airport that have been made since the 1970s, and detailed assessments of alternative sites undertaken, there is still no resolution to this issue. A Commonwealth Green Paper on Australian aviation is scheduled for release later in 2008. The practical reality is that aircraft noise at Sydney Airport cannot be prevented by its relocation: noise can only be mitigated as discussed next under management. By 2020, 62 million annual passengers are projected to use Sydney airport and the number of aircraft movements will increase considerably.
Management
What is the most appropriate management of the noise problem at the individual system and population levels, and how can systems be continually improved? These are critical questions given that the most likely prospects are for civil aviation operations to continue for a long time at Sydney airport, where already there are several management strategies in place. The first planning instrument is the dose-response relationship which uses the Australian Noise Exposure Forecast (ANEF) as the relevant metric to define land use compatibility surrounding airports. This is a land use regulation designed to make sure new residential dwellings are not approved in proximity to the airport by local governments. 161
The Long Term Operating Plan which incorporates a noise-sharing principle with the use of 10 modes of runway operations (AirServices Australia, 1996) aims to avoid concentration of noise impacts for existing residents near the airport as would be the case under parallel runway operations affecting primarily residents to the north and south of the two parallel airport runways. The federal government has imposed an hourly cap on aircraft movements of 80 at Sydney Airport. The Sydney Airport Noise Amelioration Program also aims to reduce noise at the point of reception. From 1995 to the end of 1997, 93 public buildings (schools, religious buildings, such as churches, and health care facilities) and 4600 residences were provided with acoustical treatment at a capital cost of nearly $400 million, approximately the cost of the construction of the third runway at Sydney Airport. The eligibility criterion was location within the 30 ANEF contour.
It should be noted that adverse community reaction to aircraft noise within the 25 ANEF contour is substantial (Commonwealth of Australia, Senate Select Committee, 1995). Airport environmental management systems initiated by the owners of Australian privatised airports are designed for continuous improvement in performance, but the noise from arriving and departing aircraft is regulated by Commonwealth Government laws. Hence, any future innovative systems are likely to come from federal government initiatives.
Evidence base
The evidence about the world-wide distribution and cause of the aircraft noise problem in suburbs surrounding airports is compelling (Southworth, 2007: p. 3) and renders further discussion unnecessary. However, elimination of aircraft noise is impossible given the role of international aviation in the expansion of the global economy. Even given technological advances in aircraft engine design (for example, jet engines on the A380), there is no such thing as a ‘quiet aircraft’.
Personal effects
What are the personal effects of experiencing the problem of aircraft noise? Annoyance is well documented in the literature (Hede and Bullen, 1982; Fidell et al., 1991), but stress and hypertension has only been identified in more recent years (Meister and Donatelle, 2000; HECS, 1622001; Rosenlund et al., 2001; Issarayangyun et al., 2005b; Jarup et al., 2005). In our research fully discussed in Black et al. (2007), a self-reported questionnaire using the validated instrument SF-36 measured health quality of life, prevalence of hypertension, chronic noise stress, noise sensitivity, noise annoyance, confounding factors, and demographic characteristics. After controlling for confounders, subjects around Sydney airport (aged 15–87) who have been chronically exposed to high aircraft noise level have the odds of 2.61 (95% CI 1.42–4 .80) of having chronic noise stress, and these chronic noise stress persons have the odds of 2.74 (95% CI 1.55–4.84) of having hypertension compared with those without. The control group was surveyed in an area of similar demographic characteristics not affected by aircraft noise.
Societal response
How could society respond to the problem of alleviating stress and hypertension? One possibility proposed here is the practice of meditation, a form of ‘mind body therapy’ that has arisen from the ancient Eastern spiritual tradition. It is important to define ‘meditation’ as there has been a recent shift by the US National Centre for Complementary and Alternative Medicine (NCCAM) from a Western understanding of meditation as ‘a conscious mental process that induces a set of integrated physiological changes termed the relaxation process’ to a definition more consistent with the traditional Eastern concept of ‘in meditation, a person learns to focus his attention and suspend the stream of thoughts that normally occupy the mind’ (National Center of Complementary and Alternative Medicine, 2007; Manocha, 2002). Health professionals are enthusiastic about meditation; a survey of Australian GPs in 2000 found that almost 80% of respondents had recommended meditation to patients at some time in the course of their practice yet less than 35% had any formal training or education in the field (Pirotta et al., 2000).
The authors have designed a research study that uses mediation techniques to reduce stress from suffers of aircraft noise around both commercial and military airports. The hypothesis to be tested is that the impact of stress associated with aircraft noise can be alleviated by meditation. This has proven successful with asthma, work stress and menopause (Manocha et al., 2002). The aim is to demonstrate that 163meditation, whose central characteristic is the experience of mental silence, can alleviate stress in adults caused by long-term exposure to aircraft noise. A secondary aim is to look at the cost of such an intervention and compare the cost to prescription medication for stress. To our knowledge, no study has attempted to determine how stress from airport noise can be alleviated from methods other than pharmaceutical drugs.
Subject to funding, people aged 55 years or more in aircraft noise exposed suburbs will be recruited to four focus groups. The research is targeting those adults most likely to be at home during the day and exposed to aircraft noise. It would draw on members of this network, plus advertisements placed in local newspapers, to assist in the recruitment of the elderly is noise affected suburbs near Sydney Airport. The purpose of the focus groups is to identify attitudes to aircraft noise and methods used to ameliorate the effects of aircraft noise. Knowledge of, and attitudes towards, behavioural modification techniques will also be explored.
The intervention group will be taught a meditation technique called Sahaja Yoga. The Sahaja Yoga meditation technique is proposed because it utilises a ‘classical’ understanding of meditation, in which ‘mental silence’ is regarded as the defining feature, vis-a-vis the conventional understanding of meditation as method of relaxation. The technique uses a simple series of silent affirmations based on a traditional understanding of yogic psychophysiology. Subjects will be encouraged to meditate while sitting quietly in a chair or in a comfortable position that facilitates their meditation experience. They will be encouraged to develop a sustainable state of ‘mental silence’ (Sanskrit ‘nirvichara samadhi’ or ‘thoughtless awareness’). Each subgroup will meet separately for 2 hours each week over an 8 week period, and will be given supporting tapes and asked to devote 10–20 minutes per day to this practice.
The questionnaire will be designed to capture all potential confounders. Questions concerning employment status, exercise activities, smoking status, alcohol consumption, nutrition and demographic characteristics will be adapted from the Australian Bureau of Statistics, but some questions will be designed specifically for this research. For instance, a question measuring smoking status of other members of the household will be included to eliminate the impact of passive smoking. A question 164asking how long the respondent has lived in his/her house will be included to satisfy the research assumption that long-term aircraft noise exposure has negative impacts on human health. A noise-confounding question (which is: ‘Have you recently insulated your house from noise?’) will be added to the questionnaire to eliminate the effect from acoustic insulation (which has been a feature of the noise management plan at Sydney Airport).
Participants in the intervention and the control group will be followed up using the same mail-out procedure of the three questionnaires at 6 months and at 12 months. At 6 months, we will measure whether stress, hypertension and health and wellbeing measures are significantly different between the two groups. At 12 months, the research team will ascertain whether the hypothesised lower stress levels and general health and wellbeing have been maintained in the intervention group.
Suggestions for integrated solutions
Whilst aircraft noise is especially annoying in residents’ backyards, there was definitely one place and backyard not to be: in the vicinity of Broad Street, London in 1854. Henry Whitehead located 700 deaths within a 250-yard radius and showed that use of water from the Broad Street pump was strongly correlated with death from cholera, as Dr John Snow had once hypothesised (Newson, 2006: p. 211). Thus, ‘geographical epidemiology’ began. One can imagine John Snow asking: how serious is the problem of cholera in the total population (deadly!)? What caused the problem (faeces in the water supply)? How can the problem be prevented (clean water)? What is the most appropriate management of the problem at individual system and population levels, and how can systems be continually improved (sanitary engineering)? How strong is the evidence about the distribution and cause of the problem (highly), its prevention (public hygiene), and its management (mapping)? What are the personal effects of having the problem (death)? What are the effects of the problem (and its management) on, and in, society? Finally, how does (and did) society respond to the problem (public health, engineering, and urban planning)?
Through exploring these questions, Snow pioneered ‘geographical’ epidemiology. The breadth of his work has made him one of the most revered scientists of his age. UCLA School of Public Health has devoted 165a website to his life and work. The backyard of Broadwick Street contains the ‘John Snow’ pub with a first floor display devoted to his work, a replica of the famous pump, and his picture on the inn’s sign. What might modern ‘geographical epidemiology’ look like with the availability of today’s technologies?
Many of these questions have been partially answered by the University of Sydney population health integration within the Medical Curriculum, as outlined above. In addition, we suggest that an initial research project would be to classify evidence on public health and urban form with particular reference to geographical location, as we have provided in the example of aircraft noise, and tease out built form effects from socioeconomic confounders, including the role of the law in supporting urban dysfunction (for a US example, see Buzbee, 2003).
In order to properly plan, manage and monitor any public health program, it is vital that up-to-date, relevant information is available to decision-makers at all levels of the public health system. As every public or environmental health event requires a different response and policy decision, information must be available that reflects a realistic assessment of the situation at the local level. This must be done with the best available data and taking into consideration demographics, availability of, and accessibility to, existing health and social services as well as other geographic and environmental features, including climate change impacts.
Geographic information systems (GIS) provide ideal platforms for the convergence of public and environmental health information and their analyses in relation to urban settlements, surrounding social and health services and the natural environment (Zhan et al., 2006). They are highly suitable for analysing epidemiological data, revealing trends and interrelationships that would be more difficult to discover in tabular format. Moreover, GIS allows policy makers to easily visualise problems in relation to existing health and social services and the natural environment and so more effectively target resources. The World Health Organisation (WHO) has a public health and GIS mapping program but this is at the global or national scale and not at the spatial resolution of the city, or parts of the city, that is necessary in our research design. 166
There is a clear need to create public health informatics that focus on problems of public and environmental health. Whilst this is an ambitious research and development agenda, it is also at the forefront of international competitive research where there are obvious gaps. Figure 41 provides a picture of dominant topic areas of research in health informatics in the United Kingdom, United States and Canada. These countries are at the cutting edge of research in this area according to the Queensland e-health strategy. The international classifications and codes are:
| AI | Artificial Intelligence | |
| BCS | Biomedical Cognitive Science | |
| BIO | Bioinformatics | |
| CBT | Computer Based Training | |
| CCT | Coding, Classification, Terminology | |
| CGL | Computerised Clinical Guidelines | |
| CHI | Consumer Health Informatics | |
| CIM | Clinical Information Management | |
| DI | Dental Informatics | |
| DSS | Decision Support Systems | |
| EDU | Education and Training | |
| EPR | Electronic Patient Records | |
| IR | Information Retrieval | |
| IRV | Imaging, Robotics, Virtual Reality | |
| MLP | Medical Language Processing | |
| NI | Nursing Informatics | |
| OA | Outcomes Assessment | |
| PHI | Public Health Informatics | |
| SIG | Signal processing | |
| SSL | Standards, Social and Legal Issues | |
| TEL | Telemedicine |
The gaps identified in Figure 41 of particular relevance to integrated solutions for the sustainability of cities and regions include public health informatics and outcomes assessment (see, for example, Scotch and Parmanto, 2006). There is also a clear practical need for public health informatics systems (Waitakere City Council, 2005). A stakeholder survey of 522 leaders and professionals in the 25 largest cities of the world found that health care is a major infrastructure challenge 167(Lofthouse, 2007: pp. 44–49), and furthermore noted that IT in health care has a major role to play, supporting both treatment and administration (p. 48).
Figure 41: Classification of research fields on health informatics
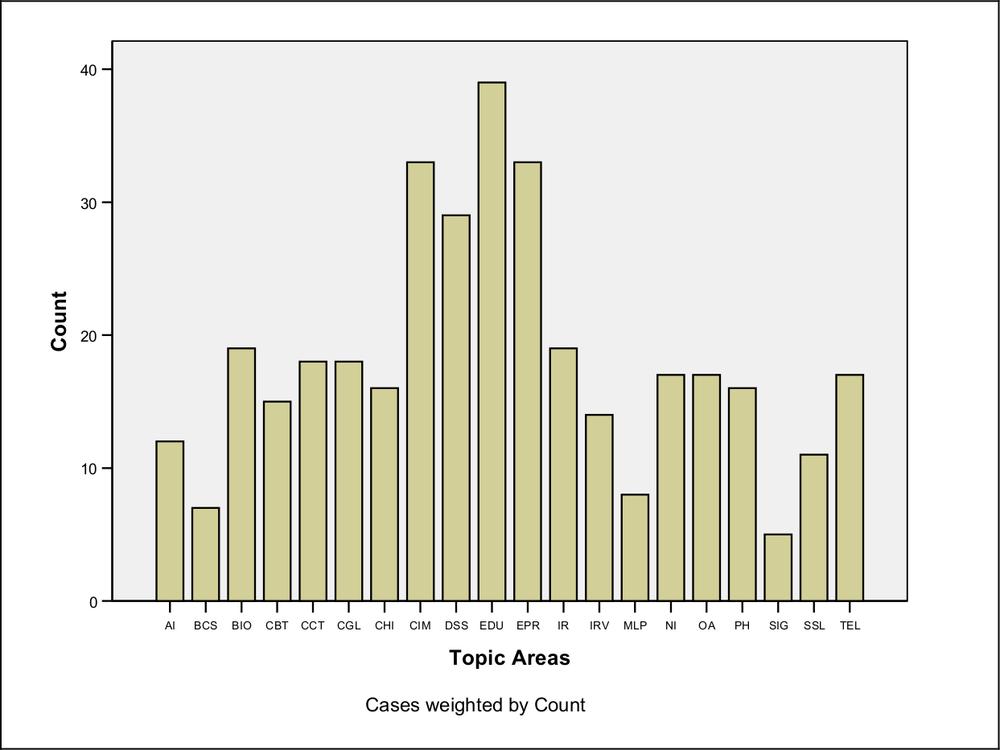
Source: web searches undertaken by authors. Data from Canada, the United Kingdom and the United States
The logical extension of this challenge is to incorporate visualisation for decision makers. As a starting point in the development of such systems, there are books on GIS and public health (Cromley and McLafferty, 2002), public health information visualisation technology (Lu, 2005), and a range of recent University initiatives linking geography, web-based spatial analysis (GIS) and epidemiology (for example, Grigg et al., 2006; Maclachlan et al., 2007). Cutchin (2007) suggests a number of geographic perspectives on health and environment that could create 168useful connections between geography and public health via social epidemiology.
Health service providers argue consistently that improved information systems will assist in providing more efficient ways of rationing health services. An important question less frequently asked about such information systems is: will improved health information systems make the services more effective? Improved information systems, which are an integral part of outcomes assessment and a continuous quality improvement model, will result in more effective decision-making leading to improved patient outcomes. If health information systems are to make a practical contribution to the health system, then there is, according to De Lone and McLean (1992), a need to measure the output concisely. As discussed extensively in the literature, there is now an emphasis on ‘customer-focus’ in health systems in Australia and overseas. The ‘customer’ in the health system is the patient, so it is argued that the output should be measured in terms of patients’ health outcomes.
If information system research is to make a contribution to the world of practice, a well-defined outcome measure (or measures) is essential. It does little good to measure various independent or input variables … if the dependent or output measure … cannot be measured with a similar degree of accuracy (De Lone and McLean, 1992: p. 61).
Conclusions
The issues of event, time and place are the basis of epidemiological studies. Integrated solutions, based on a trans-disciplinary approach and using the power of computers to link data and GIS to produce visualisation, need the specialised contributions of different professions working with a common conceptual framework. From a public health perspective, integrated solutions for the sustainability of cities and regions include public health informatics and outcomes assessment. Eight key concepts are applicable to the way that research studies of the public and environmental health issues in cities could be designed so as to promote sustainable outcomes. 169
The concepts are: 1) distribution – the problem in the total population and in different subgroups; 2) cause – the causes the problem; 3) prevention – interventions to prevent the problem; 4) management – determine the most appropriate management of the problem at individual system and population levels, and identify how to continually improve the systems; 5) evidence base – determine how strong the evidence is about the distribution and cause of the problem, its prevention and its management; 6) personal effects – specify the personal effects of having the problem; 7) societal effects – analyse the effects of the problem (and its management) on, and in, society?; and 8) societal response – How does (and could) society respond to the problem?
We have illustrated this methodology and each of the eight concepts with an example of aircraft noise at Sydney airport and an individual’s health and quality of life in, what has been described as, the ‘noise sewer’ of the University of Sydney’s backyard. The further development of public health informatics and the assessment of outcomes could be thought of as a fertile backyard meeting place of urban planners, geographers, health informatics specialists and epidemiologists. Dr John Snow pioneered ‘geographical’ epidemiology, and he breadth of his work has made him one of the most revered scientists of his age. Today, innovation across once traditionally separate disciplines is necessary to achieve more economic, social and environmentally sustainable cities and regions.
Notes
This chapter was written specifically for this book, although some of the research on aircraft noise was based on previously peer-reviewed published work with Dr Stephen Samuels (University of New South Wales) and Dr Tharit Issarayangyun (Institute of Transport and Logistics Studies, University of Sydney).
170
References
AirServices Australia (1996) The long term operating plan for Sydney (Kingsford Smith) airport and associated airspace. Canberra: AirServices Australia.
AirServices Australia (1999) The Australian noise exposure forecast system and associated land use compatibility advice for areas in the vicinity of airports. Canberra: AirServices Australia.
Bauman, A. (1995) ‘Working across sectors,’ in P. Baume and A. Bauman, A. (eds.), Public health: an introduction. Sydney: Eriador Press, pp. 54–57.
Baume, P. and Irvine, S. (1995) ‘The concept of health,’ in P. Baume and A. Bauman (eds.) Public health: an introduction. Sydney: Eriador Press, pp.8–17.
Black, D. A. and Black, J. A. (2001) ‘Main street redesign and pedestrian accident risk’. 24th Australasian Transport Research Forum (ATRF), 17–20 April, Hobart, Zero road toll – a dream or a realistic vision? (CD-Rom).
Black, D. A. and Black, J. A. (2007) ‘Aircraft noise and public health: a research design for innovative airport environmental management’. 11th World Conference on Transport Research, University of California Berkeley, CA, 24–28 June, 2007 (CD-Rom).
Black, D. A., Black, J. A., Issarayangyun, T. and Samuels, S. E. (2007) ‘Public health responses to aircraft noise and its mitigation.’ Journal of Air Transport Management. 13(5): pp. 264–276.
Black, J. and Hayashi, Y. (2005) ‘A trans-disciplinary framework: challenges in modelling the sustainable city’. Proceedings of the 9th International Conference on Computers in Urban Planning and Urban Management, University College London, 29 June to 1 July, 2005.
Black, J. A., Samuels, S. E., Masters, E., Trinder J., Morrison, J. C. and Tudge, R. (1997) ‘Road traffic noise prediction using object oriented and geographic information system technologies’. Transportation Research Record, No 1601 Environmental Issues in Transportation. Washington DC: National Academy Press. pp. 77–83.
Buzbee, W. W. (2003) ‘Urban form, health, and the Law’s limits.’ American Journal of Public Health. 93(9): pp. 1395–1399.
Capon, A. G. and Blakely, E. J. (2007) ‘Creating healthy, just and eco-sensitive cities,’ New South Wales Public Health Bulletin: 18(3–4): pp. 51–54. 171
Capon, A. G. and Dixon, J. M. (2007) ‘Cities, sustainability and health (special edition)’. New South Wales Public Health Bulletin. 18(3–4): pp. 37–72.
Commonwealth of Australia, Senate Select Committee (1995) Falling on deaf ears: report of the Senate Select Committee on Aircraft Noise in Sydney. Canberra: Department of the Senate, Senate Select Committee.
Cowie, C., Black, D. and Fraser, I. (1997) ‘Blood lead levels in preschool children in Eastern Sydney.’ Australian and New Zealand Journal of Public Health. 21(7): pp. 755–761.
Cromley, E. K. and McLafferty, S. L. (2002) GIS & Public Health. New York: Guilford Press.
Cutchin, M. P. (2007) ‘The need for the “new health geography” in epidemiologic studies of environment and health.’ Health & Place. 13(3): pp. 725–742.
De Lone, W. H. and McLean, E. R. (1992) ‘Information systems success: the quest for the dependent variable.’ Information Systems Research. 3(1): pp. 60–95.
Fidell, S., Barber, D. S., and Schultz, T. J. (1991) ‘Updating a dosage-effect relationship for the prevalence of annoyance due to general transportation noise.’ Journal of the Acoustics Society of America. 111(4): pp. 1743–1750.
Frank, L., Engelke, P. and Schmid, T. (2003) Health and community design: the impact of the built environment on physical activity. Washington DC: Island Press.
Frith, J. (1995) ‘Environmental health,’ in P. Baume and A. Bauman (eds.) Public health: an introduction. Sydney: Eriador Press, pp. 104–128.
Frumkin, H., Frank, L., and Jackson, R. (2004) Urban sprawl and public health: designing, planning and building for healthy communities. Washington DC: Island Press.
Galea, S, and Vlahov, D. (2005a) Handbook of urban health: populations, methods and practice. New York: Springer.
Galea, S. and Vlahov, D. (2005b) ‘Urbanization,’ in H. Frumkin (ed.) Environmental health: from global to local. San Francisco: Jossey-Bass, pp. 387–413.
Giles-Corti, B. (2006) The impact of urban form on public health: Current or emerging issues paper. Paper prepared for the 2006 Australian State of 172the Environment Committee, Australian Government, Department of the Environment and Water Resources, Canberra.
Grigg, M., Alfred, B., Keller, C., and Steele, J. A. (2006) ‘Implementation of an internet-based geographic information system: the Florida experience.’ Journal of Public Health Management & Practice. 12(2): pp. 139–145.
Harris, P. J., Harris-Roxas, B. F. and Kemp, L. (2007) ‘Health impact assessment in urban settings.’ New South Wales Public Health Bulletin. 18(10): pp. 149–150.
HECS (2001). Noise from civilian aircraft in the vicinity of airports: implications for human health, I. Noise, stress and cardiovascular disease. Ottawa: Minister of Public Works and Government Services Canada.
Hede, A. J. and Bullen, R. B. (1982) ‘Aircraft noise in Australia: a survey of community reaction’. National Acoustics Laboratory Report, No. 88. Canberra: Australian Government Publishing Service.
Higginbotham, N., Albrecht, G. and Connor, L. (eds.) (2001) Health social science: a trans-disciplinary and complexity perspective. Melbourne: Oxford University Press.
Issarayangyun, T., Black, J., Black, D. and Samuels, S. (2005a) Aircraft noise and environmental health: a trans-disciplinary approach. 28th Australasian Transport Research Forum Sydney, 28–30 September 2005 (CD-Rom)
Issarayangyun, T., Black, J., Black, D. and Samuels, S. (2005b) ‘Aircraft noise and methods for the study of community health and well-being.’ Journal of the Eastern Asia Society for Transportation Studies. vol. 6: pp. 3293–3308.
Jackson, L. E. (2003) ‘The relationship of urban design to human health and condition.’ Landscape Urban Planning. vol. 64: pp. 191–200.
Jarup, L., Dudley, M. L., Babisch, W., Houthuijs, D., Swart, W., Pershagen, G., Bluhm, G., Katsouyanni, M., Cadum, E. and Vigna-Taglianti, F. (2005) ‘Hypertension and exposure to noise near airports (HYENA): study design and noise exposure assessment.’ Environmental Health Perspectives. 113(11): pp. 1473–1478
Kearns, A., Beaty, M. and Barnett, G. (2007) ‘A social–ecological perspective on health in urban environments’. New South Wales Public Health Bulletin. 18(4): pp. 48–50. 173
Lofthouse, G. (ed.) (2007) Megacity challenges: a stakeholder perspective: a research project conducted by GlobeScan and MRC McLean Hazel sponsored by Siemens. Munich: Siemens A.G. Corporate Communications.
Lu, X. (2005) ‘A framework of Web GIS based unified public health information visualization platform.’ Computational Science and Its Applications. Volume 3482/2005. Berlin: Springer.
Maclachlan, J. C., Jerrett, M., Abernathy, T. Sears, M., and Bunch, M. J. (2007) ‘Mapping health on the internet: a new tool for environmental justice and public health research.’ Health & Place. 13(1): pp. 72–86.
Manocha, R., Marks, G. B., Kenchington, P., Peters, D. and Salome, C. M. (2002) ‘Sahaja Yoga in the management of moderate to severe: a randomised controlled trial.’ Thorax. 57(2): pp. 110–115.
Meade, M. S. and Earickson, R. J. (2000) Medical Geography. New York: The Guilford Press.
Meister, E., and Donatelle, R. (2000) ‘The impacts of commercial aircraft on human health: a neighborhood study in metropolitan Minnesota.’ Journal of Environmental Health. 63(4): pp. 9–15.
National Center of Complementary and Alternative Medicine (2007) http://nccam.nih.gov/health/meditation/overview.htm (consulted 5th December, 2007).
Newsom, S. W. B. (2006) ‘Pioneers in infection control: John Snow, Henry Whitehead, the Broad Street pump, and the beginnings of geographical epidemiology.’ Journal of Hospital Infection. 64(3): pp. 210–216.
NSW Health, Sydney West Area Health Service (2006) Health impact assessment report: Greater Granville Regeneration Strategy: Stage 1 consultants report. NSW Health, Sydney West Area Health Service.
Pirotta, M. V., Cohen, M. M., Kotsirilos, V. and Farish, S. J. (2000) ‘Complementary therapies: have they become accepted in general practice?.’ Medical Journal of Australia. 172(3): pp. 105–9.
Rosenlund, M., Berglind, N., Pershagen, G., Jarup, L., and Bluhm, G. (2001) ‘Increased prevalence of hypertension in a population exposed to aircraft noise.’ Journal of Occupational and Environmental Medicine. vol. 58: pp. 769–773.
Scotch, M. and Parmanto, B. (2006) ‘Development of SOVAT: a numerical-spatial decision support system for community health 174assessment research.’ International Journal of Medical Informatics. 75(10–11): pp. 771–784.
Southgate, D., Aked, R., Fisher, N. and Rhynehart, G. (2000). Discussion paper: expanding ways to describe and assess aircraft noise. Canberra: National Capital Printing.
Southworth, M. (2007) Urban forms and metropolitan spaces. Berkeley.it università degli studi di roma sapienza, facoltà di ingegneria, 2nd–3rd April, 2007.
Trevena, L. J., Sainsbury, P., Henderson-Smart, C., Clarke, R., Rubin, G. and Cumming, R. (2005) ‘Population health integration within a medical curriculum: an eight-part toolkit.’ American Journal of Preventive Medicine. 29(3): pp. 234–239.
Waitakere City Council (2005) Towards sustainable urban form: connecting research and practice II: workshop summary 15 April 2005. Waitakere City: Waitakere City Council.
Zhan, F. B., Brender, J. D., Han, Y., Suarez, L. and Langlois, P. H. (2006) ‘GIS-EpiLink: a spatial search tool for linking environmental and health data.’ Journal of Medical Systems. 30(5): pp. 405–412.